Myocardial abscess
| Myocardial abscess | |
 | |
|---|---|
| Myocardial abscess: Candida: Gross, natural color excellent depiction myocardial abscesses caused by Candida tropicalis. A 51yo man with acute monocytic leukemia. Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Mohammed Salih, M.D. Syed Musadiq Ali M.B.B.S.[2]
overview
A cardiac abscess is a suppurative infection of the myocardium, endocardium, native or prosthetic valve tissue. Similar to other abscesses, it develops either by dissemination from a distant source such as bacteremia or sepsis or by direct extension of a pre-existing cardiac infective focus. Infective endocarditis has long been identified as the main cause of the latter. Although the incidence of cardiac abscesses continues to be investigated, it is presumably higher than noted postmortem and is of great importance when deciding the prognosis and management of patients. A single organism causes cardiac abscesses, usually Staphylococcus aureus or Escherichia coli. Less typically, polymicrobial abscesses have been noted. Important complications of a cardiac abscess, whether alone or with valve tissue, are conduction abnormalities on electrocardiogram (ECG). The incidence of perivalvular abscess among patients with infective endocarditis is between 30% to 40%, with the aortic valve having a higher predisposition than the mitral valve and annulus. Native aortic valve endocarditis, usually located in a weak part of the annulus near the atrioventricular node (AV), clearly demonstrates the anatomic predisposition and exemplifies why abscesses and heart block presents as frequent sequelae. Perivalvular abscesses are also more common with prosthetic valves. In this case, the annulus instead of the leaflet is usually the primary site of infection. The degree of conduction disruption, therefore, depends on the extent of the involvement of the conduction system and is more commonly seen in perivalvular aortic abscesses. Additionally, the severe extension of perivalvular infection can also result in extrinsic coronary compression, or disruption, leading to an acute coronary syndrome. Thus far, only aortic valve involvement and current IV drug use have been prospectively identified as independent risk factors for a perivalvular abscess. Any patient with a cardiac abscess, regardless of all other factors, has an increased risk of embolization, morbidity, and mortality. Prophylaxis remains a longstanding subject in the matter of prevention of IE or cardiac abscess. Thus far, prophylaxis is mostly based on observational studies and, in fact, places such as the United Kingdom no longer endorse antibiotic prophylaxis for dental procedures to prevent IE, the leading source of the cardiac abscess. One point against prophylaxis is the fact that tooth brushing has been proven to cause bacteremia and, therefore, makes it difficult to assess the rare versus high magnitude transient bacteremia and its effect on IE and its sequelae. For this reason, the United States and European countries have agreed that the use of prophylaxis is reserved only for those at "highest risk." On that same matter, the widespread use of antibiotics for the prevention and treatment of IE and abscesses could potentially create a setting where there will be an increased incidence of polymicrobial infection and antibiotic resistance, especially in immunocompromised patients.
Historical perspective
- In 1933, Cossio and Berconsky reported a case of coronary occlusion with myocardial infarction in which an abscess was found in the infarcted area at post-mortem examination.[1]
Pathophysiology
Myocardial abscess is a pus-containing infection of the endocardium, myocardium, prosthetic or native valves, perivalvular structures or the cardiac conduction system. [2] [3]
Pathogenesis
- Development of infective endocarditis and subsequent myocardial abscess involves interaction of multiple factors, as follows[4]:
- Vascular endothelium
- Hemostatic mechanisms
- Host immune system
- Gross anatomic abnormalities in the heart
- Surface properties of microorganisms
- Extracardiac events that introduce bacteremia
- The rarity of endocarditis despite the relatively high prevalence of transient asymptomatic and symptomatic bacteremia suggests that the intact endothelium is resistant to infection.If the endothelium on the valve surface is damaged, hemostasis is stimulated and the deposition of platelets and fibrin complex begins. This complex, called non-bacterial thrombotic endocarditis (NBTE), is more susceptible to bacterial colonization when bacteremia develops from an extracardiac source that allows the organisms access to the NBTE[5] [6].
- The intracardiac consequences of endocarditis range from trivial, characterized by an infected vegetation with no attendant tissue damage, to catastrophic, when infection is locally destructive or extends beyond the valve leaflet. Distortion or perforation of valve leaflets, rupture of chordae tendineae, and perforations or fistulas may result in progressive congestive heart failure (CHF). Infection, particularly that involving the aortic valve or prosthetic valves, may extend into paravalvular tissue and result in myocardial abscesses and persistent fever due to the infection's unresponsiveness to the antibiotic; disruption of the conduction system, with electrocardiographic conduction abnormalities; and clinically relevant arrhythmias or purulent pericarditis[7] [8] [9].
Post-mortem examination,of myocardial abscess, showed following pathological changes:
Macroscopic finding
- The cardiac area was greatly enlarged, and when the pericardial sac was opened, it was found to contain 600 cc of partially clotted blood.
- The parietal pericardium was blood tinged but smooth and glistening throughout [10] [11] [12] .
- The epicardium was normal in appearance over the anterior aspect of the heart but glassy and coated with a thin layer of fibrinous exudate in the posterior aspect.
- The tear involved the entire thickness of the myocardium so that a probe could be passed through it into the left ventricular cavity without resistance.
- The surrounding myocardium was infiltrated by blood and flabby in consistence in an area about 6 cm in diameter.
- Externally and on cut section this area displayed a variegated tinge from reddish brown to yellowish gray.
- Clusters of honey-combed pockets, each pin head in size or larger, were scattered throughout this area.
- Grossly, these pockets were suggestive of small abscesses and contained a thick, golden-yellow material.
- The coronary arteries were diffusely narrowed, with atheroma formation and calcification.
- The right coronary artery was occluded a short distance below its main stem by a firmly adherent, friable, yellowish-brown thrombotic mass.
- Examination of the cardiac chambers revealed a laminated thrombus on the posterior aspect of the left ventricle[13].
-
 Myocardial abscess: Candida: Gross, natural color excellent depiction myocardial abscesses caused by Candida tropicalis. A 51yo man with acute monocytic leukemia.
Myocardial abscess: Candida: Gross, natural color excellent depiction myocardial abscesses caused by Candida tropicalis. A 51yo man with acute monocytic leukemia. -
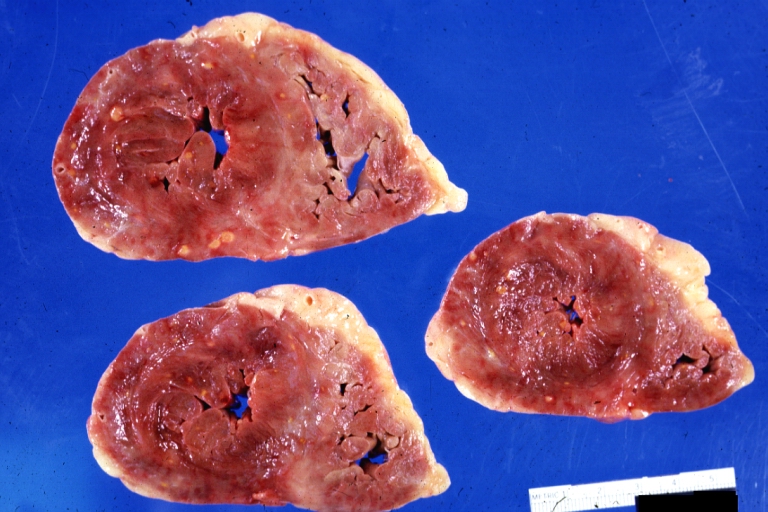 Myocardial abscess: Candida: Gross, natural color, (an excellent example) three horizontal sections of myocardium with obvious abscesses caused by Candida tropicalis. A 51yo man with acute monocytic leukemia
Myocardial abscess: Candida: Gross, natural color, (an excellent example) three horizontal sections of myocardium with obvious abscesses caused by Candida tropicalis. A 51yo man with acute monocytic leukemia

Microscopic finding
- Myocardial infarct the microscopical sections showed an almost complete obliteration of the normal architecture[14] [15].
- The muscle fibers displayed loss of striations and of nuclear patterns and seemed fused together into an amorphous mass of eosinophilic material.
- The capillaries in the area were congested, and extravasated red cells were present throughout.
- There was a concomitant marked infiltration of polymorphonuclear leukocytes either scattered or in clusters, and this extended into the epicardium.
- The leukocytes were not well preserved; the majority were fused together or showed karyorrhexis and karyolysis resulting in a scattering of cellular débris.
- The endocardial mural thrombus consisted of amorphous eosinophilic material and was interspersed with white cells and cellular débris.
- The mural thrombus merged indistinctly into the adjacent necrotic myocardium.
- The thrombotic mass in the lumen of the right coronary artery showed incipient organization with intimal histiocytic and fibroblastic proliferation and atheromatous changes[16].
-
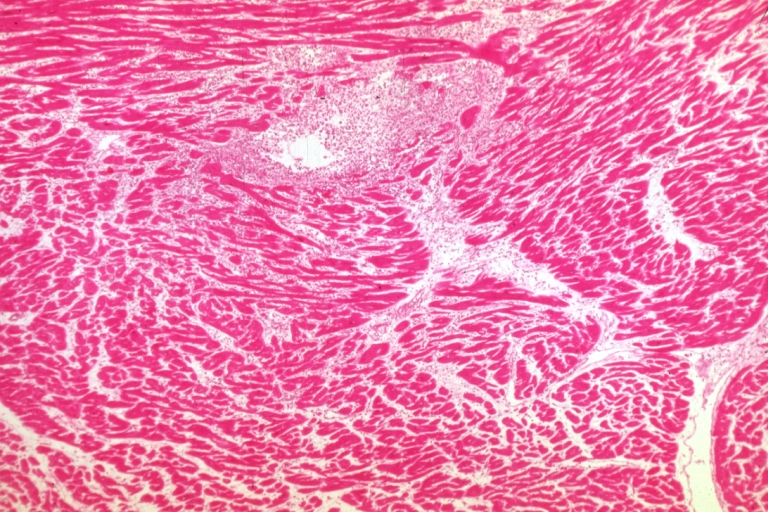 Abscess in Myocardium: Micro low mag, H&E. Obvious abscess in a drug addict with Pseudomonas endocarditis
Abscess in Myocardium: Micro low mag, H&E. Obvious abscess in a drug addict with Pseudomonas endocarditis

Causes
- Cardiac abscesses are rare in the United States. Cardiac abscesses are most commonly thought to occur primarily by the extent of a pre-existing [[cardiac] infection, as it is with the case of infective endocarditis (IE) [17] [18] [19]. Secondary causes of cardiac abscess are believed to be due to bacteremia (persistent or transient) without a known cardiac source, as well as susceptible heart tissue soon after myocardial infarction (MI), or prosthetic valve disease, usually in the setting of bacteremia. Staphylococcus aureus is the most common pathogen when the disease is present.The following are organisms noted to be involved in cardiac abscess formation[20]:
- Staphylococcus aureus
- Haemophilus species
- Enterococci
- Escherichia coli
- Beta-hemolytic streptococci
- Streptococcus pneumoniae
- The most common clinical setting for myocardial abscess is as a complication of endocarditis involving either native or prosthetic valves.
- In a review of 40 cases of infective endocarditis, Gonzalez Vilchez et al (1991) found that 67.5% (27 cases) involved native valves.
- The most common site was the aortic valve, followed in descending order by the ventricular septa, mitral valves, and papillary muscles.
- Approximately one third of cases involved the base of the aortic valve.
- Staphylococcus was the most prevalent species involved, isolated from one third of all cases.
- Prosthetic valve abscess comprised 34% of cases, and 50% of these were caused by staphylococcal infection.
- An infected coronary artery stent may be a rare source of multiple myocardial abscesses[21].
Bacteremia
- In the past, the most common setting for myocardial abscess was generalized bacteremia, as described in older autopsy reports.
- Sanson and colleagues (1963) described 23 cases, 21 of which exhibited multiple abscesses in lungs, kidneys, brain, and myocardium. Myocardial abscesses were small in these patients, and the authors postulated that the patients died too early to develop larger abscesses[22].
- Myocardial abscess may develop at the site of a myocardial infarction (MI) but usually develops in the setting of bacteremia[23].
- Cossio et al (1933) reported a myocardial abscess at the site of an acute MI.
- In the case records of the Massachusetts General Hospital, Castleman and McNeely (1970) reported a secondary infection within an inferior wall MI in a patient with Bacteroides bacteremia following genitourinary surgery and placement of an infected indwelling catheter.
- In a review of 13 cases of myocardial abscess in acute MI, Weisz and Young (1977) found bronchopneumonia to be the probable source in 4 cases, gastrointestinal and renal sepsis in 2, and no definable source in the others. Organisms included Staphylococcus aureus, Clostridium perfringens, Bacteroides species, Escherichia coli, beta-hemolytic streptococci, and Streptococcus pneumoniae, in order of decreasing frequency.
- The propensity of cardiac muscle to develop myocardial abscess in the setting of acute MI and septicemia may be due to the presence of necrosis of the muscular fibers and surrounding inflammatory exudates, decreased or absent perfusion, and lack of cell-mediated immunity secondary to decreased blood flow. Such myocardium also appears to be at a greater risk of rupture than healthy myocardium (7-fold higher per Weisz and Young [1977], with a catastrophic outcome.
Other settings associated with myocardial abscesses that have been reported in the literature include the following:
- Trauma
- Deep penetrating wounds
- Deep burns
- Infected pseudoaneurysms
- Suppurative pericarditis
- Infected transplanted hearts
- Extension from sternal abscess
- HIV-associated myocarditis and suppuration
- Parasitic infections
- Infection of a left ventricular aneurysm or tumor
Differential Diagnosis
Myocardial Abscess should be differentiated from other diseases presenting with fever, chest pain and anorxia. The differentials include the following:[24][25][26][27][28][29][30][31][32][33][34][35][36][37][38][39][40][41][42][43]
| Diseases | Diagnostic tests | Physical Examination | Symptoms | Past medical history | Other Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CT scan and MRI | EKG | Chest X-ray | Tachypnea | Tachycardia | Fever | Chest Pain | Hemoptysis | Dyspnea on Exertion | Wheezing | Chest Tenderness | Nasalopharyngeal Ulceration | Carotid Bruit | |||
| Pulmonary embolism |
|
|
|
✔ | ✔ | ✔ (Low grade) | ✔ | ✔ (In case of massive PE) | ✔ | - | - | - | - |
|
|
| Infective Endocarditis | ✔ | ✔ | ✔ | - | - | ✔ | - | - | - | - |
|
| |||
| Non-Bacterial Thrombotic Endocarditis | ✔ | ✔ | ✔ (Low grade) | ✔ (Relieved by sitting up and leaning forward) | - | ✔ | - | - | - | - |
|
||||
| Libman Sack Endocarditis | ✔ | ✔ | ✔ | ✔ | - | ✔ | ✔ | - | - | - |
|
| |||
| Vasculitis |
|
|
✔ | ✔ | ✔ | ✔ | ✔ | ✔ | - | ✔ | ✔ | ✔ |
|
||
| Fever of unknown origin (FUO) | ✔ | ✔ | - | - | - | ✔ | ✔ | - | - | - |
|
| |||
Epidemiology and Demographics
- Myocardial abscess rarely occurs in the United States.
- Seventy-seven percent of the patients presented early in the disease course (ie, within the first month), with few of the classic clinical hallmarks of infective endocarditis[44].
- S aureus was the most common pathogen found (31.2% of patients). The mitral valve was found to be infected in 41.1% of cases and the aortic valve in 37.6%. The common complications included stroke (16.9%), embolization other than stroke (22.6%), heart failure (32.3%), and intracardiac abscess (14.4%). Surgical therapy was performed in 48.2% of the patients, and in-hospital mortality rates were high (17.7%).
- In the early 21st century, infective endocarditis continues to be more often an acute disease, characterized by a high rate of S aureus infection and an unacceptably high mortality rate.
- The incidence of infective endocarditis remained relatively stable from 1950-1987, at approximately 4.2 cases per 100,000 patient-years.
- During the early 1980s, the yearly incidence of infective endocarditis was 2 cases per 100,000 population in the United Kingdom and Wales.
- 1.9 cases per 100,000 population in the Netherlands. A higher incidence was noted from 1984-1990; 5.9 and 11.6 episodes per 100,000 population were reported from Sweden and metropolitan Philadelphia, respectively.
- Infections involving prosthetic valves, especially mechanical prostheses, in which the infection is entirely periannular, often extend into the adjacent myocardium, resulting in paravalvular abscess formation and partial dehiscence of the prosthetic valve with paravalvular regurgitation.
- Ben Ismail et al (1987) found annulus infection and valve dehiscence in (82%) infected mechanical valves examined at surgery or autopsy.
- Myocardial abscess formation profoundly worsens the prognosis in patients with infectiveendocarditis.
- The mortality rate associated with S aureus infective endocarditis is 42% overall. If treated with antibiotics only, the mortality rate is 75%, while a regimen that combines antibiotics and surgery reduces the mortality rate to 25%.
- Myocardial abscess have more prevalent in African Americans in urban setting.
- Myocardial abscess is also more common in women than in men. Among persons who abuse intravenous drugs, myocardial abscess is more prevalent in men (65%-80%).
Risk Factors
Any septic focus can theoretically lead to myocardial abscess. These are the primary foci in order of frequency of causing myocardial abscess.
- Spread from the urinary tract is the most common cause.
- Gastrointestinal diseases:
- Spread from the gastrointestinal tract is the second common cause (e.g. perforated appendix, perforated colon cancer, diverticulitis ,and cohn’s disease.)
- e.g. pott's disease or osteomyelitis
- Hematogenous spread[47]
- From distant septic foci.[48]
Any condition compromising the immune system is a risk factor for developing myocardial abscess. The following were the risk factors in observed patients. [49]
- Diabetes Mellitus
- Cirrhosis
- Malignancy
- Remote infection
- Glucocorticoids administration
- Chronic renal failure
Screening
According to the USPSTF, screening for retroperitoneal abscess is not recommended.
Natural History, Complications and Prognosis:
Natural history
If left untreated, myocardial abscess may cause heart block, septal rupture with very high incidence of morbidity and mortality.
Complications :
The following are potential complications of myocardial abscess[20]:
- Myocardial perforation[50]
- Significant clinical deterioration
- Worsening CHF
- Worsening heart sound and murmurs
- New-onset valvular regurgitation (100% of cases)
- Poor response to antibiotics
- Development of conduction defects or progression of heart block, such as bundle-branch block and atrioventricular block (45%)
- Sudden onset of complete heart block or Mobitz type II block (highly specific)
- Type of valve involvement, eg, aortic valve endocarditis (40%-85%)
- Miscellaneous (severe recurrent ventricular arrhythmias, pericarditis [uncommon], infection of the prosthetic valves, right-sided endocarditis in patients with congenital heart disease)
Prognosis
- Depending on the extent of the abscess at the time of diagnosis, the prognosis may vary[51] .
- The condition carries a very high mortality ranging from 30% to 75% without treatment. To reduce the morbidity and mortality of this disorder, it is imperative that a structured approach is developed to make an early diagnosis and begin treatment.
- Even with therapy, mortality rates of 5% to 15% are not uncommon.
Diagnosis
History
- A detailed history should be obtained from the patient presenting with infective endocarditis and chest pain.
- Patients who have longstanding persistent bacteremia and who do not respond to antibiotic therapy.
- Myocardial abscess is more prevalent in the period following mechanical interventions or surgery and in patients with HIV/AIDS-related myocarditis[52].
Symptoms
One must bear in mind certain constellations of symptoms that may raise the suggestion of myocardial abscess. For example, fever is the most common symptom, presenting in 80%-85% of patients. It is absent in some patients who are elderly; those who have CHF, severe debility, or chronic renal failure; and in patients with coagulase-negative staphylococcal infection and abscess. Another characteristic symptom is chills, which occurs in 42%-75% of cases[53].
Common symptoms:
Less common symptoms:
Physical Exam
General Appearance
Physical examination findings commonly encountered in myocardial abscess are mainly due to the underlying infective endocarditis. These include the following: Fever, Tachycardia, Murmur, especially changing or new murmur, Neurological abnormalities, Embolic event, Splenomegaly, Clubbing, Peripheral manifestations,Osler nodes, Splinter hemorrhages, Petechiae, Janeway lesions, Retinal lesions (Roth spots),Widening pulse pressure, especially with involvement of the aortic valve and progression of aortic regurgitation The patient is usually fatigued & looking ill due to the preexisting risk factor. In advanced cases with septicemia, the patient may be drowsy with decreased level of consciousness.[49]
Vital signs
- Fever[54]
- Tachycardia
- Tachypnea
- Hypotension (if patient is presenting with shock)
Chest Examination
- Chest tenderness is often present (localized).
- Alteration of heart sounds and murmurs (new-onset valvular regurgitation [100% of cases])
Lab Findings
- Complete blood cell count findings commonly are abnormal.
- Anemia with normochromic normocytic red cell indices is present.
- A low serum iron level is also observed. A low serum iron-binding capacity is observed in 70-90% of patients.
- Anemia worsens with increased duration of illness.
- In subacute endocarditis, the white blood cell count is usually normal.
- In contrast, a leukocytosis with increased segmented granulocytes is common in acute endocarditis and myocardial abscess.
- The erythrocyte sedimentation rate (ESR) is elevated (on average approximately 55 mm/h) in almost all patients with endocarditis and myocardial abscess; the exceptions are those with CHF, renal failure, or disseminated intravascular coagulation.
- Blood cultures are the crucial laboratory tests for confirming the diagnosis of the underlying endocarditis.
- Urinalysis results are often abnormal, even when renal function remains normal. Proteinuria and microscopic hematuria are noted in 50% of patients. Urinalysis also plays a standard role in the evaluation of azotemia, which is frequently associated with myocardial abscess[54].
Radiological Findings
- In the past, most cases of myocardial abscess were found during autopsy. however, detection of myocardial abscess can now be achieved antemortem using multiple noninvasive imaging modalities, including transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE), indium In 111 radionuclide scintigraphy, computed tomography (CT) scan, and magnetic resonance imaging (MRI).
- chest radiography is perform to look for associated pulmonary infection.
- Chest radiographic findings help assess for CHF.
Transthoracic echocardiography
- TTE helps evaluate patients in whom endocarditis or myocardial abscess is suggested clinically. Findings frequently allow the morphologic confirmation of infection and increasingly aid in making decisions regarding management.
- One must perform an echocardiographic evaluation in all patients suspected of having an intracardiac or pericardial infection, including those with negative blood culture findings[21].
- TTE has a sensitivity of 23% and specificity of 98.6%.
- According to Ellis et al (1985), the following 5 criteria are 86% sensitive and 88% specific for myocardial abscess:
- Evidence of prosthetic valve rocking
- Aneurysmal dilatation of the sinus of Valsalva
- Posterior aortic root thickness greater than 10 mm
- Perivalvular density in the septum of greater than 14 mm
- The presence of "echo-free space" - Very specific but found relatively infrequently
- Walker et al report a rare case of a myocardial abscess in valvular endocarditis that was difficult to assess with 2-dimensional TTE; however, real-time 3-dimensional contrast TTE allowed visualization of the full extent of the defect and its precise anatomical location, prior to successful surgical resection.
Transesophageal echocardiography
- Although many patients with NVE involving the aortic or mitral valve can be adequately assessed using TTE, TEE with color flow and continuous pulsed Doppler is the state-of-the-art technique. Doppler and color-flow Doppler or contrast 2-dimensional echocardiography helps optimally define fistulas and abscess pockets and extensions. See the image below.
- TEE has a sensitivity of 87% and specificity of 94.6%. Patients in whom an abscess is suggested but has not been detected using TEE should undergo MRI, including magnetic resonance angiography.[55]
- Indium In 111 leukocyte scintigraphy is especially useful in prosthetic valve endocarditis, in which echocardiography shows too much scatter[56].
- A few milliliters of venous blood is drawn and mixed with an anticoagulant solution. The white blood cells are separated and labeled with radioactive isotope111 In, centrifuged, resuspended in isotonic sodium chloride solution, and reinjected into the patient. Images are then obtained with a gamma-ray camera within 16-24 hours. *The viable radioactive leukocytes potentially accumulate in the areas of inflammation or abscess. Obtain oblique views to avoid overshadowing by sternal accumulation[57].
- The need for111 In scintigraphy is very low if TEE is used.
- This is a good modality for helping delineate myocardial abscess. However, the portability and excellent resolution of echocardiography make it more practical than MRI[58].
- Only anecdotal reports of diagnosis are available. It is not very sensitive[59].
Intraoperative echocardiography
- Although invasive, small abscesses can be detected in the operating room by means of intraoperative echocardiography, which may enable the operating surgeon to drain the abscess effectively.
Other Diagnostic Studies
Electrocardiography
- New-onset and persistent electrocardiographic conduction abnormalities may be observed. Gradual PR prolongation may be observed, and it may suggest development of valve ring abscess.
- Although not a sensitive indicator of perivalvular infection or abscess (28%), these findings are relatively specific (85-90%)[22].
Tests of immune system stimulation
- Tests results may show disease activity, but the tests are costly and not very efficient for diagnosis or monitoring response to therapy
- These may include testing of circulating immune complexes, rheumatoid factor, quantitative immune globulin, cryoglobulins, and C-reactive protein[60].
Serologic tests
- Serological test findings are used to evaluate cardiac sepsis in which blood culture findings are negative.
- Tests to detect antibodies to ribitol teichoic acids from staphylococci may help distinguish uncomplicated S aureus bacteremia from that associated with cardiac involvement.
- These tests have not been used in clinical applications because of their lack of adequate specificity or predictive value.
Procedures
- Cardiac catheterization may add very little to the imaging studies and is not recommended unless coronary angiography is needed for patients undergoing valve surgery who also may have significant coronary artery disease.
Treatment
- Intravenous antibiotics should be administered in a timely fashion once a patient is suspected of IE or a cardiac abscess. Empiric broad-spectrum antibiotics until further characterization of infective species should be monitored for at least 6 weeks of therapy in this patient population[61][62].
- Supportive treatment includes the following:
- Fluid and electrolyte balance
- Nutritional support
- Surgery consult and the time of surgical intervention is of high importance when approaching a patient with a cardiac abscess.
- There is increased morbidity and mortality in patients in whom surgery is delayed. Thus early surgery is recommended. Surgery for these patients aims toward the eradication of the infection and correction of hemodynamic abnormalities[63].
- However, some patients with periannular extension of infection or myocardial abscess could potentially be treated without surgical intervention. These patients include[64]:
- Patients with smaller (less than 1 cm) abscesses
- Patients who do not have complications of heart block, an echocardiographic progression of abscess during antibiotic therapy
- Patients who do not have valvular dehiscence or insufficiency.
- It is recommended that patients who do not undergo surgery are monitored closely with serial TEE repeated at 2, 4, and 8 weeks after completion of antibiotic therapy.
References
- ↑ Kim JS, Kang MK, Cho AJ, Seo YB, Kim KI (May 2017). "Complicated infective endocarditis: a case series". J Med Case Rep. 11 (1): 128. doi:10.1186/s13256-017-1274-7. PMC 5423006. PMID 28482860.
- ↑ Tennant R, H.W. Parks: Myocardial abscesses. Arch Pathol 68,112-6 (1959)
- ↑ Narula J, B.A. Khaw, W. Dec, I.F. Palacios, J.F. Southern, J.T. Fallon, H.W. Strauss, E. Haber, T. Yasuda: Recognition of acute myocarditis masquerading as acute myocardial infarction. NEJM 328,100-4 (1993)
- ↑ Oliveira J, Santos M, Arnoni RT, Ramos A, Togna DD, Ghorayeb SK, Kroll R, Souza L (2018). "Mortality Predictors in the Surgical Treatment of Active Infective Endocarditis". Braz J Cardiovasc Surg. 33 (1): 32–39. doi:10.21470/1678-9741-2017-0132. PMC 5873776. PMID 29617499. Vancouver style error: initials (help)
- ↑ Howitt T: Remarkable case of abscess of the heart. Lancet 1, 684-685 (1846)
- ↑ Abela GS, B. Majmudar, J.M. Felner: Myocardial abscess unassociated with infective endocarditis. South Med J 74, 432-434 (1981)
- ↑ Howitt T: Remarkable case of abscess of the heart. Lancet 1, 684-685 (1846)
- ↑ Abela GS, B. Majmudar, J.M. Felner: Myocardial abscess unassociated with infective endocarditis. South Med J 74, 432-434 (1981)
- ↑ Saphir O: Myocarditis: A general review, with an analysis of two hundred and forty cases. Arch Pathol 32,1000-1051 (1941)
- ↑ Flaxman N: Myocardial abscess. JAMA 122, 804-806 (1943)
- ↑ Sanson J, S. Slodki, J.G. Gruhn: Myocardial abscesses. Am Heart J 66, 301-308 (1963)
- ↑ Weiss S, R.W. Wilkins: Myocardial abscess with perforation of the heart. Am J Med Sci 194,199-205 (1937)
- ↑ TEDESCHI CG, STEVENSON TD, LEVENSON HM (December 1950). "Abscess formation in myocardial infarction". N. Engl. J. Med. 243 (26): 1024–7. doi:10.1056/NEJM195012282432602. PMID 14785774.
- ↑ Bateman AC, M. Richards, A.P. Pallett. Fatal myocarditis associated with a Lancefield Group B Streptococcus. J Infect 36,354-5 (1998)
- ↑ Von Kurnatowski HA, J.L.Sierra-Callejas, W. Henkel: Foudroyant todlich verlaufende myokarditis durch streptokokken der gruppe B. Dtsch Med Wschr 103,439-41 (1977)
- ↑ Tedeschi CG, T.D. Stevenson, H.M. Levenson. Abscess formation in myocardial infarction. NEJM 243,1024-7 (1950)
- ↑ Saphir O: Meningococcus myocarditis. Am J Pathol 12,677-87 (1936)
- ↑ McCue MJ, E.E. Moore: Myocarditis with microabscess formation caused by Listeria monocytogenes associated with myocardial infarct. Human Pathol 10:469-72 (1979)
- ↑ Lewis JF: Myocardial infarction during pregnancy: With associated myocardial Bacteroides abscess. South Med J 66,379-1 (1973)
- ↑ 20.0 20.1 Ramos Tuarez FJ, Law MA. PMID 29083576. Missing or empty
|title=(help) - ↑ 21.0 21.1 Zeineddin M, Stewart JA (July 1988). "Echocardiographic detection of non-valve-ring myocardial abscess complicating aortic valve endocarditis". Am. J. Med. 85 (1): 97–9. doi:10.1016/0002-9343(88)90510-4. PMID 3389387.
- ↑ 22.0 22.1 Akins EW, Slone RM, Wiechmann BN, Browning M, Martin TD, Mayfield WR (June 1991). "Perivalvular pseudoaneurysm complicating bacterial endocarditis: MR detection in five cases". AJR Am J Roentgenol. 156 (6): 1155–8. doi:10.2214/ajr.156.6.2028858. PMID 2028858.
- ↑ Kim HS, Weilbaecher DG, Lie JT, Titus JL (July 1978). "Myocardial abscesses". Am. J. Clin. Pathol. 70 (1): 18–23. doi:10.1093/ajcp/70.1.18. PMID 696668.
- ↑ Brenes-Salazar JA (2014). "Westermark's and Palla's signs in acute and chronic pulmonary embolism: Still valid in the current computed tomography era". J Emerg Trauma Shock. 7 (1): 57–8. doi:10.4103/0974-2700.125645. PMC 3912657. PMID 24550636.
- ↑ "CT Angiography of Pulmonary Embolism: Diagnostic Criteria and Causes of Misdiagnosis | RadioGraphics".
- ↑ Bĕlohlávek J, Dytrych V, Linhart A (2013). "Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism". Exp Clin Cardiol. 18 (2): 129–38. PMC 3718593. PMID 23940438.
- ↑ "Pulmonary Embolism: Symptoms - National Library of Medicine - PubMed Health".
- ↑ Ramani GV, Uber PA, Mehra MR (2010). "Chronic heart failure: contemporary diagnosis and management". Mayo Clin. Proc. 85 (2): 180–95. doi:10.4065/mcp.2009.0494. PMC 2813829. PMID 20118395.
- ↑ Blinderman CD, Homel P, Billings JA, Portenoy RK, Tennstedt SL (2008). "Symptom distress and quality of life in patients with advanced congestive heart failure". J Pain Symptom Manage. 35 (6): 594–603. doi:10.1016/j.jpainsymman.2007.06.007. PMC 2662445. PMID 18215495.
- ↑ Hawkins NM, Petrie MC, Jhund PS, Chalmers GW, Dunn FG, McMurray JJ (2009). "Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology". Eur. J. Heart Fail. 11 (2): 130–9. doi:10.1093/eurjhf/hfn013. PMC 2639415. PMID 19168510.
- ↑ Takasugi JE, Godwin JD (1998). "Radiology of chronic obstructive pulmonary disease". Radiol. Clin. North Am. 36 (1): 29–55. PMID 9465867.
- ↑ Wedzicha JA, Donaldson GC (2003). "Exacerbations of chronic obstructive pulmonary disease". Respir Care. 48 (12): 1204–13, discussion 1213–5. PMID 14651761.
- ↑ Nakawah MO, Hawkins C, Barbandi F (2013). "Asthma, chronic obstructive pulmonary disease (COPD), and the overlap syndrome". J Am Board Fam Med. 26 (4): 470–7. doi:10.3122/jabfm.2013.04.120256. PMID 23833163.
- ↑ Khandaker MH, Espinosa RE, Nishimura RA, Sinak LJ, Hayes SN, Melduni RM, Oh JK (2010). "Pericardial disease: diagnosis and management". Mayo Clin. Proc. 85 (6): 572–93. doi:10.4065/mcp.2010.0046. PMC 2878263. PMID 20511488.
- ↑ Bogaert J, Francone M (2013). "Pericardial disease: value of CT and MR imaging". Radiology. 267 (2): 340–56. doi:10.1148/radiol.13121059. PMID 23610095.
- ↑ Gharib AM, Stern EJ (2001). "Radiology of pneumonia". Med. Clin. North Am. 85 (6): 1461–91, x. PMID 11680112.
- ↑ Schmidt WA (2013). "Imaging in vasculitis". Best Pract Res Clin Rheumatol. 27 (1): 107–18. doi:10.1016/j.berh.2013.01.001. PMID 23507061.
- ↑ Suresh E (2006). "Diagnostic approach to patients with suspected vasculitis". Postgrad Med J. 82 (970): 483–8. doi:10.1136/pgmj.2005.042648. PMC 2585712. PMID 16891436.
- ↑ Stein PD, Dalen JE, McIntyre KM, Sasahara AA, Wenger NK, Willis PW (1975). "The electrocardiogram in acute pulmonary embolism". Prog Cardiovasc Dis. 17 (4): 247–57. PMID 123074.
- ↑ Warnier MJ, Rutten FH, Numans ME, Kors JA, Tan HL, de Boer A, Hoes AW, De Bruin ML (2013). "Electrocardiographic characteristics of patients with chronic obstructive pulmonary disease". COPD. 10 (1): 62–71. doi:10.3109/15412555.2012.727918. PMID 23413894.
- ↑ Stein PD, Matta F, Ekkah M, Saleh T, Janjua M, Patel YR, Khadra H (2012). "Electrocardiogram in pneumonia". Am. J. Cardiol. 110 (12): 1836–40. doi:10.1016/j.amjcard.2012.08.019. PMID 23000104.
- ↑ Hazebroek MR, Kemna MJ, Schalla S, Sanders-van Wijk S, Gerretsen SC, Dennert R, Merken J, Kuznetsova T, Staessen JA, Brunner-La Rocca HP, van Paassen P, Cohen Tervaert JW, Heymans S (2015). "Prevalence and prognostic relevance of cardiac involvement in ANCA-associated vasculitis: eosinophilic granulomatosis with polyangiitis and granulomatosis with polyangiitis". Int. J. Cardiol. 199: 170–9. doi:10.1016/j.ijcard.2015.06.087. PMID 26209947.
- ↑ Dennert RM, van Paassen P, Schalla S, Kuznetsova T, Alzand BS, Staessen JA, Velthuis S, Crijns HJ, Tervaert JW, Heymans S (2010). "Cardiac involvement in Churg-Strauss syndrome". Arthritis Rheum. 62 (2): 627–34. doi:10.1002/art.27263. PMID 20112390.
- ↑ Murdoch DR, Corey GR, Hoen B, Miró JM, Fowler VG, Bayer AS, Karchmer AW, Olaison L, Pappas PA, Moreillon P, Chambers ST, Chu VH, Falcó V, Holland DJ, Jones P, Klein JL, Raymond NJ, Read KM, Tripodi MF, Utili R, Wang A, Woods CW, Cabell CH (March 2009). "Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study". Arch. Intern. Med. 169 (5): 463–73. doi:10.1001/archinternmed.2008.603. PMC 3625651. PMID 19273776.
- ↑ Khan B, Strate RW, Hellman R (2007). "Myocardial abscess and fatal cardiac arrhythmia in a hemodialysis patient with an arterio-venous fistula infection". Semin Dial. 20 (5): 452–4. doi:10.1111/j.1525-139X.2007.00247.x. PMID 17897252.
- ↑ Smith RE, Martin JE, Mills PG (August 1989). "Myocardial abscess and sternal osteomyelitis following myocardial infarction and resuscitation". Postgrad Med J. 65 (766): 589–90. doi:10.1136/pgmj.65.766.589. PMC 2429504. PMID 2602260.
- ↑ Debelian GJ, Olsen I, Tronstad L (April 1994). "Systemic diseases caused by oral microorganisms". Endod Dent Traumatol. 10 (2): 57–65. doi:10.1111/j.1600-9657.1994.tb00061.x. PMID 8062808.
- ↑ Omran H, Reichel H, Wirtz P, Jung W, Rabahieh R, Pfeifer U, Pfeiffer D, Lüderitz B (February 1997). "[Septic myocardial aneurysm in mitral valve endocarditis. Clinical and pathological-anatomical findings]". Dtsch. Med. Wochenschr. (in German). 122 (6): 156–60. doi:10.1055/s-2008-1047590. PMID 9081801.
- ↑ 49.0 49.1 Grollier G, Burucoa C, Bonnin M, de Rautlin de La Roy Y (1992). "Identification and susceptibility testing for obligate anaerobic bacteria using a semi-automated API ATB plus system". Ann Biol Clin (Paris). 50 (6–7): 393–7. PMID 1492717.
- ↑ Shackcloth MJ, Dihmis WC (August 2001). "Contained rupture of a myocardial abscess in the free wall of the left ventricle". Ann. Thorac. Surg. 72 (2): 617–9. doi:10.1016/s0003-4975(00)02530-3. PMID 11515915.
- ↑ Grant R, Page S, Iyer A (March 2018). "Contained myocardial abscess following a myocardial infarction". J Card Surg. 33 (3): 144–145. doi:10.1111/jocs.13555. PMID 29526056.
- ↑ Borowski A, Korb H, Voth E, de Vivie ER (December 1988). "Asymptomatic myocardial abscess". Thorac Cardiovasc Surg. 36 (6): 338–40. doi:10.1055/s-2007-1022976. PMID 3232134.
- ↑ Crespo EP, Bertrán DV, Martínez CB, Foradada JT, Diz FW (April 2011). "[Myocardial abscess]". Med Clin (Barc) (in Spanish; Castilian). 136 (9): 415. doi:10.1016/j.medcli.2009.11.015. PMID 20149397.
- ↑ 54.0 54.1 54.2 Chikwe J, Barnard J, Pepper JR (June 2004). "Myocardial abscess". Heart. 90 (6): 597. doi:10.1136/hrt.2003.024646. PMC 1768256. PMID 15145849.
- ↑ Hill EE, Herijgers P, Claus P, Vanderschueren S, Peetermans WE, Herregods MC (November 2007). "Abscess in infective endocarditis: the value of transesophageal echocardiography and outcome: a 5-year study". Am. Heart J. 154 (5): 923–8. doi:10.1016/j.ahj.2007.06.028. PMID 17967599.
- ↑ Campeau RJ, Ingram C (September 1998). "Perivalvular abscess complicating infective endocarditis: complementary role of echocardiography and indium-111-labeled leukocytes". Clin Nucl Med. 23 (9): 582–4. doi:10.1097/00003072-199809000-00003. PMID 9735977.
- ↑ Ivancević V, Munz DL (March 1999). "Nuclear medicine imaging of endocarditis". Q J Nucl Med. 43 (1): 93–9. PMID 10230285.
- ↑ Pasowicz M, Klimeczek P, Wicher-Muniak E, Podolec P, Kapelak B, Sadowski J, Tracz W (2002). "[Usefulness of magnetic resonance imaging in diagnosis of mitral valve anulus abscess--case report]". Prz. Lek. (in Polish). 59 (8): 623–5. PMID 12638334.
- ↑ Reynier C, Garcier J, Legault B, Motreff P, Ponsonnaille J, Ravel A, De Riberolles C, Boyer L (June 2001). "[Cross-sectional imaging of post endocarditis paravalvular myocardial abscesses of native mitral valves: 4 cases]". J Radiol (in French). 82 (6 Pt 1): 665–9. PMID 11449169.
- ↑ Singh B (February 2000). "Stimulation of the developing immune system can prevent autoimmunity". J. Autoimmun. 14 (1): 15–22. doi:10.1006/jaut.1999.0349. PMID 10648113.
- ↑ Yamamoto S, Hosokawa N, Sogi M, Inakaku M, Imoto K, Ohji G, Doi A, Iwabuchi S, Iwata K (April 2012). "Impact of infectious diseases service consultation on diagnosis of infective endocarditis". Scand. J. Infect. Dis. 44 (4): 270–5. doi:10.3109/00365548.2011.638317. PMID 22176644.
- ↑ Sande MA, Courtney KB (July 1976). "Nafcillin-gentamicin synergism in experimental staphylococcal endocarditis". J. Lab. Clin. Med. 88 (1): 118–24. PMID 1047088.
- ↑ Arita M, Kusuyama Y, Takatsuji M, Kawazoe K, Masuyama Y (April 1985). "Septal myocardial abscess and infectious pericarditis in a case of bacterial endocarditis". Jpn. Circ. J. 49 (4): 451–5. doi:10.1253/jcj.49.451. PMID 4009931.
- ↑ Mildvan D, Goldberg E, Berger M, Altchek MR, Lukban SB (1977). "Diagnosis and successful management of septal myocardial abscess: a complication of bacterial endocarditis". Am. J. Med. Sci. 274 (3): 311–6. doi:10.1097/00000441-197711000-00010. PMID 610417.