Myocarditis: Difference between revisions
(→Toxic) |
No edit summary |
||
| Line 22: | Line 22: | ||
{{Editor Join}} | {{Editor Join}} | ||
== | ==[[Myocarditis Overview|Overview]]== | ||
==[[Myocarditis epidemiology|Epidemiology]]== | |||
==[[Myocarditis signs and symptoms|Signs and symptoms]]== | |||
== Diagnosis == | == Diagnosis == | ||
Revision as of 17:42, 17 June 2011
| Myocarditis | |
.JPG) | |
|---|---|
| Histopathological image of viral myocarditis at autopsy in a patient with acute onset of congestive heart failure. Viral etiology, however, failed to be determined in postmortem serological study. | |
| ICD-10 | I09.0, I51.4 |
| ICD-9 | 391.2, 422, 429.0 |
| DiseasesDB | 8716 |
| MedlinePlus | 000149 |
| eMedicine | med/1569 emerg/326 |
| MeSH | D009205 |
|
WikiDoc Resources for Myocarditis |
|
Articles |
|---|
|
Most recent articles on Myocarditis Most cited articles on Myocarditis |
|
Media |
|
Powerpoint slides on Myocarditis |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Myocarditis at Clinical Trials.gov Clinical Trials on Myocarditis at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Myocarditis
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Myocarditis Discussion groups on Myocarditis Patient Handouts on Myocarditis Directions to Hospitals Treating Myocarditis Risk calculators and risk factors for Myocarditis
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Myocarditis |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
| Cardiology Network |
 Discuss Myocarditis further in the WikiDoc Cardiology Network |
| Adult Congenital |
|---|
| Biomarkers |
| Cardiac Rehabilitation |
| Congestive Heart Failure |
| CT Angiography |
| Echocardiography |
| Electrophysiology |
| Cardiology General |
| Genetics |
| Health Economics |
| Hypertension |
| Interventional Cardiology |
| MRI |
| Nuclear Cardiology |
| Peripheral Arterial Disease |
| Prevention |
| Public Policy |
| Pulmonary Embolism |
| Stable Angina |
| Valvular Heart Disease |
| Vascular Medicine |
Editors-In-Chief: Josh Hare, M.D.; C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Please Join in Editing This Page and Apply to be an Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [3] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
Epidemiology
Signs and symptoms
Diagnosis
Myocardial inflammation can be suspected on the basis of electrocardiographic results (ECG), elevated CRP and/or ESR and increased IgM (serology) against viruses known to affect the myocardium. Markers of myocardial damage (troponin or creatine kinase cardiac isoenzymes) are elevated.[1]
Electrocardiographic Findings
The ECG findings most commonly seen in myocarditis are sinus tachycardia, diffuse T wave inversions; ST segment elevation may also be present (these are also seen in pericarditis).[1]
Endomyocardial Biopsy
The gold standard is still biopsy of the myocardium, generally done in the setting of angiography. A small tissue sample of the endocardium and myocardium is taken, and investigated by a pathologist by and if necessaryimmunochemistry and special staining methods. Histopathological features are: myocardial interstitium with abundant edema and inflammatory infiltrate, rich in lymphocytes and macrophages. Focal destruction of myocytes explains the myocardial pump failure.[1]
Cardiac Magnetic Resonance Imaging
Recently, cardiac magnetic resonance imaging (cMRI or CMR) has been shown to be very useful in diagnosing myocarditis by visualizing markers for inflammation of the myocardium.[2]
Differential Diagnosis of Underlying Causes
A large number of different causes have been identified as leading to myocarditis:[1]
Infectious
Immunological
Toxic
Physical agents
Bacterial myocarditis is rare in patients without immunodeficiency.
The Heart in Toxoplasma Gondii Myocarditis
<youtube v=2s9OuW9XlUw/>
The Heart in Coxsackie B2 Myocarditis
<youtube v=R_7AXF61QGg/>
Treatment
Bacterial infections are treated with antibiotics, dependent on the nature of the pathogen and its sensitivity to antibiotics. As most viral infections cannot be treated with directed therapy, symptomatic treatment is the only form of therapy for those forms of myocarditis, e.g. NSAIDs for the inflammatory component and diuretics and/or inotropes for ventricular failure. ACE inhibitor therapy may aid in left ventricular remodeling after the inflammation has begun to resolve.
Pathologic Findings
Autopsy Study
Clinical Summary
A 21-year-old male with sickle cell anemia had recurrent attacks of acute rheumatic fever beginning at age 14.
Mitral insufficiency and stenosis were present by age 16.
On prophylactic antibiotics, the patient had no evidence of recurrence until three weeks before his final admission, when an upper respiratory infection developed. A few weeks later he developed acute migratory polyarthritis. This was associated with rapid deterioration of cardiac function and death.
Autopsy Findings
At autopsy, the heart was enlarged (weighing 675 grams) especially the left atrium. Both the aortic and mitral valves showed fibrosis as well as the fresh, tiny verrucae characteristic of acute rheumatic fever.
Images
-

This is a gross photograph of mitral valve demonstrating marked thickening and fibrosis of the valve leaflet. There are also numerous foci of fibrinoid necrosis within the cusps and friable vegetations (verrucae) along the lines of closure (arrows). These irregular, warty projections are found at sites of erosion on the inflamed endocardial surface. The verrucae probably result from the precipitation of fibrin where the leaflets impinge on each other.
-

This is a low-power photomicrograph of heart tissue. Little can be seen at this magnification, except that the tissue looks relatively normal.


-
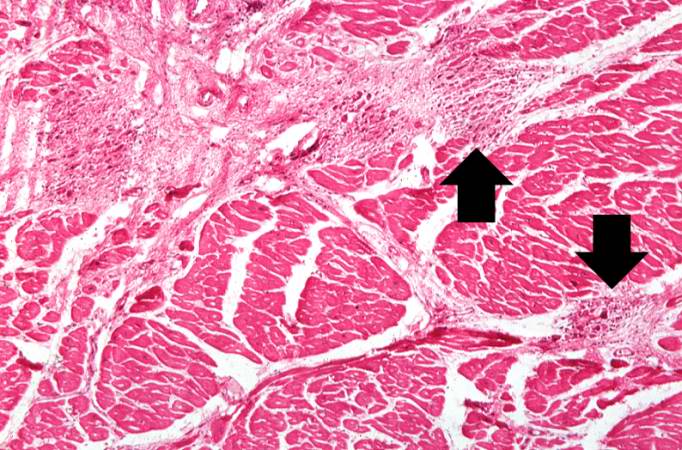
This is a higher-power photomicrograph of myocardium showing cellular accumulations--Aschoff bodies (arrows)--within the interstitium of the myocardium. These are found especially around blood vessels.
-
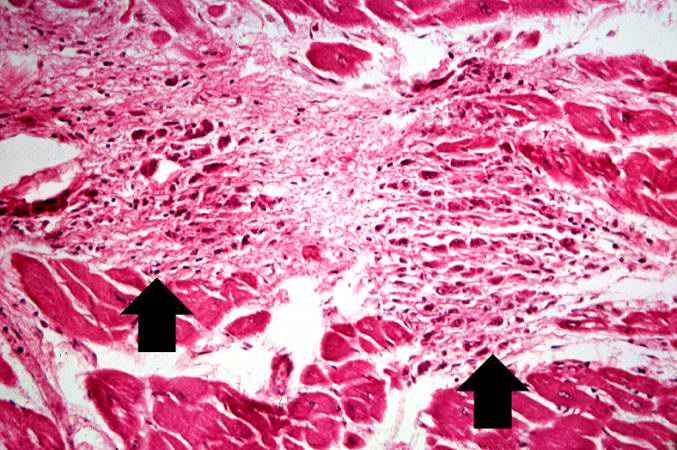
This is a higher-power photomicrograph of myocardium containing Aschoff bodies (arrows) within the interstitium.


-
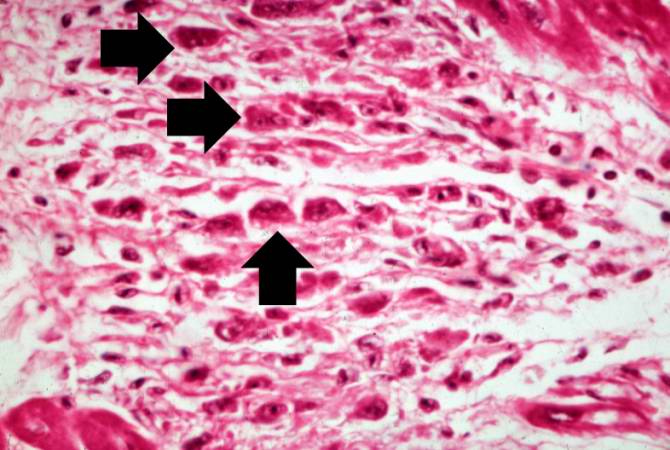
This high-power photomicrograph of myocardium shows the cellular detail of an Aschoff body. Aschoff bodies are foci of fibrinoid necrosis surrounded by lymphocytes, macrophages, an occasional plasma cell, and plump “activated” histiocytes called Anitschkow cells or Aschoff cells (arrows). These distinctive cells have abundant amphophilic cytoplasm and central round-to-ovoid nuclei in which the chromatin is disposed in a central, slender, wavy ribbon resembling a caterpillar (hence the designation “caterpillar cells”).
-
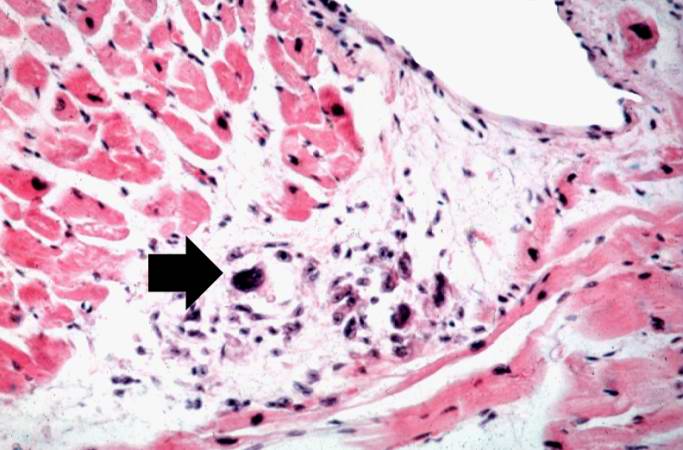
This high-power photomicrograph of myocardium shows the cellular detail of another Aschoff body. In this case there appears to be a multinucleated Aschoff giant cell (arrow).


References
External links
de:Myokarditis it:Miocardite fi:Sydänlihastulehdus sv:Hjärtmuskelinflammation