Cerebrovascular accident: Difference between revisions
| Line 489: | Line 489: | ||
== Future or Investigational Therapies == --> | == Future or Investigational Therapies == --> | ||
==Case Examples== | |||
==References== | ==References== | ||
Revision as of 13:38, 23 February 2009
| Cerebrovascular accident (Stroke) | |
 | |
|---|---|
| Brain, hemorrhagic stroke Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology | |
| ICD-10 | I61-I64 |
| ICD-9 | 435-436 |
| OMIM | 601367 |
| DiseasesDB | 2247 |
| MedlinePlus | 000726pi |
| eMedicine | neuro/9 emerg/558 emerg/557 pmr/187 |
| MeSH | D020521 |
| Cardiology Network |
 Discuss Cerebrovascular accident further in the WikiDoc Cardiology Network |
| Adult Congenital |
|---|
| Biomarkers |
| Cardiac Rehabilitation |
| Congestive Heart Failure |
| CT Angiography |
| Echocardiography |
| Electrophysiology |
| Cardiology General |
| Genetics |
| Health Economics |
| Hypertension |
| Interventional Cardiology |
| MRI |
| Nuclear Cardiology |
| Peripheral Arterial Disease |
| Prevention |
| Public Policy |
| Pulmonary Embolism |
| Stable Angina |
| Valvular Heart Disease |
| Vascular Medicine |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [3]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [4] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Related Key Words and Synonyms: Stroke, cerebrovascular event, CVA, cerebral emboli
Overview
Cerebrovascular accident (Stroke) is the clinical designation for a rapidly developing loss of brain function due to an interruption in the blood supply to all or part of the brain. This phenomenon can be caused by thrombosis, embolism, or hemorrhage. [1] In medicine the process of being struck down by a stroke, fit or feint is sometimes called an ictus, from the Latin icere (“to strike”), especially prior to the definitive diagnosis being made.
CVA is a medical emergency and can cause permanent neurological damage or even death if not promptly diagnosed and treated. It is the third leading cause of death and the leading cause of adult disability in the United States and industrialized European nations. It is predicted that stroke will soon become the leading cause of death worldwide.
The symptoms of stroke can be quite heterogeneous, and patients with the same cause of stroke can have widely differing handicaps. Conversely, patients with the same clinical handicap can in fact have different underlying causes.
The cause of stroke is an interruption in the blood supply, with a resulting depletion of oxygen and glucose in the affected area. This immediately reduces or abolishes neuronal function, and also initiates an ischemic cascade which causes neurons to die or be seriously damaged, further impairing brain function.
Risk factors for stroke include advanced age, hypertension (high blood pressure), previous stroke or TIA (transient ischaemic attack), diabetes mellitus, high cholesterol, cigarette smoking, atrial fibrillation, migraine[2] with aura, and thrombophilia. In clinical practice, blood pressure is the most important modifiable risk factor of stroke; however many other risk factors, such as cigarette smoking cessation and treatment of atrial fibrillation with anticoagulant drugs, are important.
The traditional definition of stroke, devised by the World Health Organisation in the 1970s[3], is of a 'neurological deficit of cerebrovascular cause that persists beyond 24 hours or is interrupted by death within 24 hours'.
This definition was largely devised for the purpose of research and the time frame of 24 hours appears purely arbitrarily chosen as a cut-off point. It divides stroke from TIA (or 'mini-stroke'), which is the same as above but completely resolves clinically within 24 hours. The division of stroke and TIA into separate clinical entities is considered impractical and even unhelpful in practice by many stroke doctors. The main reason for this is the fact that stroke and TIA are caused by the same disease process, and both persons with a stroke or a TIA are at a higher risk of a subsequent stroke.
In recognition of this, and improved methods for the treatment of stroke, the term "brain attack" is being promoted in the Western World as a substitute for stroke or TIA. The new term makes an analogy with "heart attack" (myocardial infarction), because in both conditions, an interruption of blood supply causes death of tissue that is highly time dependent ('time is brain') and potentially life-threatening. Many hospitals have "brain attack" teams within their neurology departments specifically for swift treatment of stroke.
Types of stroke
Strokes can be classified into two major categories: ischemic and hemorrhagic. Ischemia can be due to thrombosis, embolism, or systemic hypoperfusion. Hemorrhage can be due to intracerebral hemorrhage, subarachnoid hemorrhage, subdural hemorrhage, or epidural hemorrhage. ~80% of strokes are due to ischemia.
Ischemic stroke
In an ischemic stroke (approximately 80% of strokes), a blood vessel becomes occluded and the blood supply to part of the brain is totally or partially blocked. Ischemic stroke is commonly divided into thrombotic stroke, embolic stroke, systemic hypoperfusion (Watershed or Border Zone stroke), or venous thrombosis. Cocaine abuse doubles the risk of ischemic strokes.[4]
-

Autopsy of brain showing middle cerebral artery territory
-
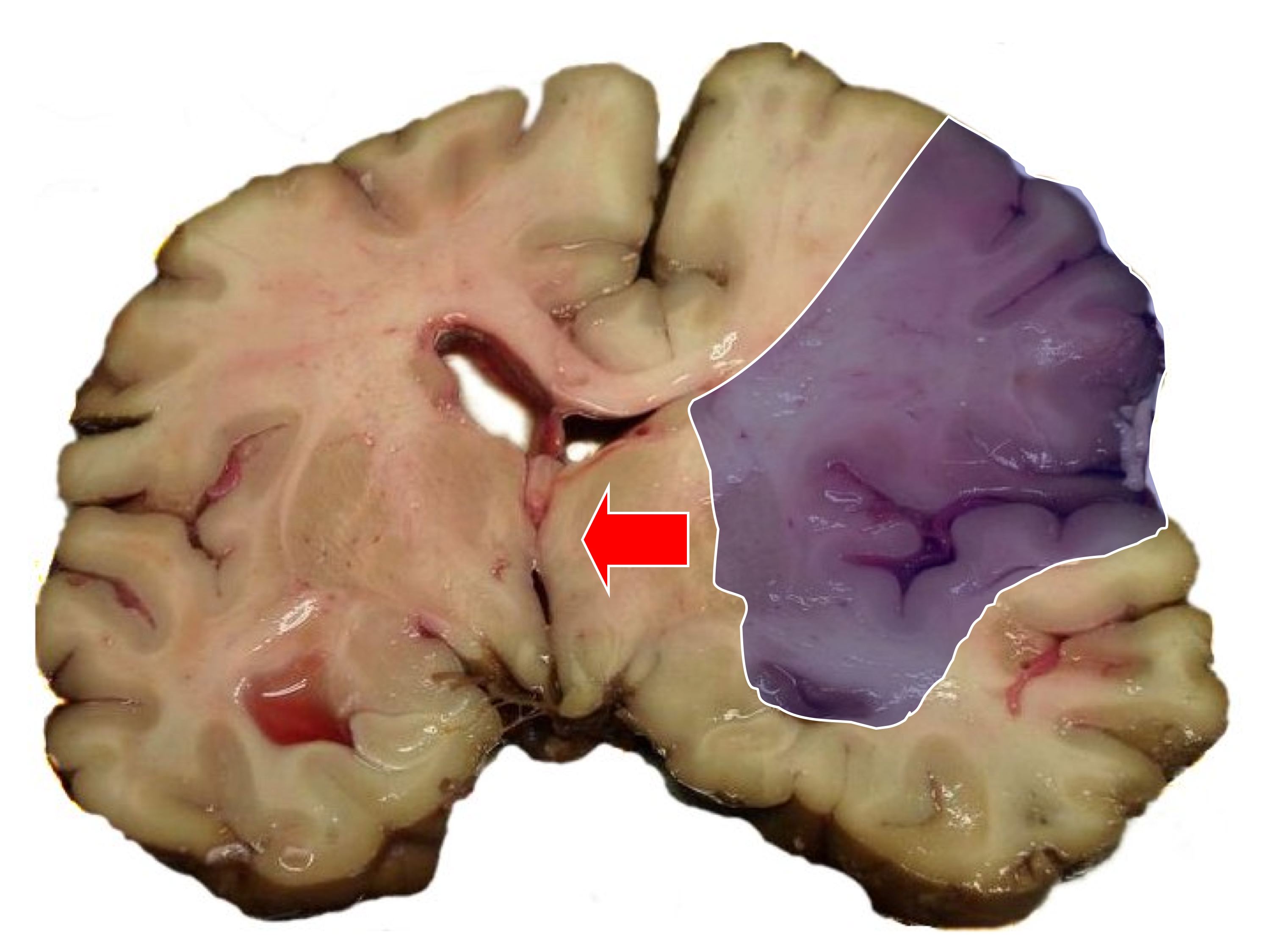
Same image; infarct area (blue shading) and midline shift


Thrombotic stroke
In thrombotic stroke, a thrombus-forming process develops in the affected artery. The thrombus — a built-up clot — gradually narrows the lumen of the artery and impedes blood flow to distal tissue. These clots usually form around atherosclerotic plaques. Since blockage of the artery is gradual, onset of symptomatic thrombotic strokes is slower. A thrombus itself (even if non-occluding) can lead to an embolic stroke (see below) if the thrombus breaks off—at which point it is then called an "embolus." Thrombotic stroke can be divided into two types depending on the type of vessel the thrombus is formed on:
- Large vessel disease involves the common and internal carotids, vertebral, and the Circle of Willis. Diseases that may form thrombi in the large vessels include (in descending incidence):
- Atherosclerosis
- Vasoconstriction
- Dissection
- Takayasu arteritis
- Giant cell arteritis
- Arteritis/vasculitis
- Noninflammatory vasculopathy
- Moyamoya syndrome
- Fibromuscular dysplasia
- Small vessel disease involves the intracerebral arteries, branches of the Circle of Willis, middle cerebral artery, stem, and arteries arising from the distal vertebral and basilar artery. Diseases that may form thrombi in the small vessels include (in descending incidence):
- Lipohyalinosis (lipid hyaline build-up secondary to hypertension and aging) and fibrinoid degeneration (stroke involving these vessels are known as lacunar infarcts)
- Microatheromas from larger arteries that extend into the smaller arteries (atheromatous branch disease)
Embolic stroke
Embolic stroke refers to the blockage of arterial access to a part of the brain by an embolus—a traveling particle or debris in the arterial bloodstream originating from elsewhere. An embolus is most frequently a blood clot, but it can also be a plaque broken off from an atherosclerotic blood vessel or a number of other substances including fat (e.g., from bone marrow in a broken bone), air, and even cancerous cells. Another cause is bacterial emboli released in infectious endocarditis.
Because an embolus arises from elsewhere, local therapy only solves the problem temporarily. Thus, the source of the embolus must be identified. Because the embolic blockage is sudden in onset, symptoms usually are maximal at start. Also, symptoms may be transient as the embolus lyses and moves to a different location or dissipates altogether. Embolic stroke can be divided into four categories:
- those with known cardiac source
- those with potential cardiac or aortic source (from transthoracic or transesophageal echocardiogram)
- those with an arterial source
- those with unknown source
High risk cardiac causes include:[5]
- Atrial fibrillation and paroxysmal atrial fibrillation
- Rheumatic mitral or aortic valve disease
- Bioprosthetic and mechanical heart valves
- Atrial or ventricular thrombus
- Sick sinus syndrome
- Sustained atrial flutter
- Recent myocardial infarction (within one month)
- Chronic myocardial infarction together with ejection fraction <28 percent
- Symptomatic congestive heart failure with ejection fraction <30 percent
- Dilated cardiomyopathy
- Libman-Sacks endocarditis
- Antiphospholipid syndrome
- Marantic endocarditis from cancer
- Infective endocarditis
- Papillary fibroelastoma
- Left atrial myxoma
- Coronary artery bypass graft (CABG) surgery
Potential cardiac causes include:[5]
- Mitral annular calcification
- Patent foramen ovale
- Atrial septal aneurysm
- Atrial septal aneurysm with patent foramen ovale
- Left ventricular aneurysm without thrombus
- Isolated left atrial smoke on echocardiography (no mitral stenosis or atrial fibrillation)
- Complex atheroma in the ascending aorta or proximal arch
Systemic hypoperfusion (Watershed stroke)
Systemic hypoperfusion is the reduction of blood flow to all parts of the body. It is most commonly due to cardiac pump failure from cardiac arrest or arrhythmias, or from reduced cardiac output as a result of myocardial infarction, pulmonary embolism, pericardial effusion, or bleeding. Hypoxemia (low blood oxygen content) may precipitate the hypoperfusion. Because the reduction in blood flow is global, all parts of the brain may be affected, especially "watershed" areas --- border zone regions supplied by the major cerebral arteries. Blood flow to these areas does not necessarily stop, but instead it may lessen to the point where brain damage can occur. This phenomenon is also referred to as "last meadow" to point to the fact that in irrigation the last meadow receives the least amount of water.
Hemorrhagic stroke
A hemorrhagic stroke, or cerebral hemorrhage, is a form of stroke that occurs when a blood vessel in the brain ruptures or bleeds. Like ischemic strokes, hemorrhagic strokes interrupt the brain's blood supply because the bleeding vessel can no longer carry the blood to its target tissue. In addition, blood irritates brain tissue, disrupting the delicate chemical balance, and, if the bleeding continues, it can cause increased intracranial pressure which physically impinges on brain tissue and restricts blood flow into the brain. In this respect, hemorrhagic strokes are more dangerous than their more common counterpart, ischemic strokes. There are two types of hemorrhagic stroke: intracerebral hemorrhage, and subarachnoid hemorrhage. Amphetamine abuse quintuples, and cocaine abuse doubles, the risk of hemorrhagic strokes.
-

Brain, hemorrhagic stroke
-
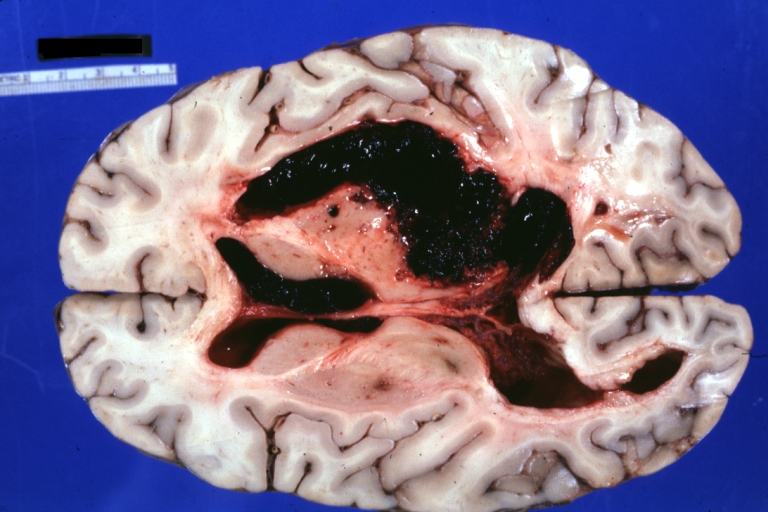
Brain: Hemorrhage: Gross fixed tissue horizontal section cerebral hemispheres with large hemorrhage in right thalamus and upper brainstem excellent example of a typical hypertensive stroke

Risk Factors
- Age >65
- Aortic arch plaque
- Cigarette smoking
- Coronary Artery Disease
- Diabetes mellitus
- Family history of ischemic stroke
- Hypercholesterolemia
- Hypertension
- Hypertriglyceridemia
- Hypothyroidism
- Increased apolipoprotein a
- Obesity
- Oral contraceptives
- African-American and Hispanic race
- Sedentary life style
- Female gender
Epidemiology and Demographics
Hippocrates (460 to 370 BC) was first to describe the phenomenon of sudden paralysis. Apoplexy, from the Greek word meaning "struck down with violence,” first appeared in Hippocratic writings to describe this phenomenon.[6][7]
In 1658, in his Apoplexia, Johann Jacob Wepfer (1620–1695) identified the cause of hemorrhagic stroke when he suggested that people who had died of apoplexy had bleeding in their brains.[6][8] Wepfer also identified the main arteries supplying the brain, the vertebral and carotid arteries, and identified the cause of ischemic stroke when he suggested that apoplexy might be caused by a blockage to those vessels.[8]
The word stroke was used as a synonym for apoplectic seizure as early as 1599[9], and is a fairly literal translation of the Greek term.
Pathophysiology & Etiology
Ischemic stroke occurs due to a loss of blood supply to part of the brain, initiating the Ischemic cascade. Brain tissue ceases to function if deprived of oxygen for more than 60 to 90 seconds and after a few hours will suffer irreversible injury possibly leading to death of the tissue, i.e., infarction. Atherosclerosis may disrupt the blood supply by narrowing the lumen of blood vessels leading to a reduction of blood flow, by causing the formation of blood clots within the vessel, or by releasing showers of small emboli through the disintegration of atherosclerotic plaques. Embolic infarction occurs when emboli formed elsewhere in the circulatory system, typically in the heart as a consequence of atrial fibrillation, or in the carotid arteries. These break off, enter the cerebral circulation, then lodge in and occlude brain blood vessels.
Due to collateral circulation, within the region of brain tissue affected by ischemia there is a spectrum of severity. Thus, part of the tissue may immediately die while other parts may only be injured and could potentially recover. The ischemia area where tissue might recover is referred to as the ischemic penumbra.
As oxygen or glucose becomes depleted in ischemic brain tissue, the production of high energy phosphate compounds such as adenine triphosphate (ATP) fails leading to failure of energy dependent processes (such as ion pumping) necessary for tissue cell survival. This sets off a series of interrelated events that result in cellular injury and death. A major cause of neuronal injury is release of the excitatory neurotransmitter glutamate. The concentration of glutamate outside the cells of the nervous system is normally kept low by so-called uptake carriers, which are powered by the concentration gradients of ions (mainly Na+) across the cell membrane. However, stroke cuts off the supply of oxygen and glucose which powers the ion pumps maintaining these gradients. As a result the transmembrane ion gradients run down, and glutamate transporters reverse their direction, releasing glutamate into the extracellular space. Glutamate acts on receptors in nerve cells (especially NMDA receptors), producing an influx of calcium which activates enzymes that digest the cells' proteins, lipids and nuclear material. Calcium influx can also lead to the failure of mitochondria, which can lead further toward energy depletion and may trigger cell death due to apoptosis.
Ischaemia also induces production of oxygen free radicals and other reactive oxygen species. These react with and damage a number of cellular and extracellular elements. Damage to the blood vessel lining or endothelium is particularly important. In fact, many antioxidant neuroprotectants such as uric acid and NXY-059 work at the level of the endothelium and not in the brain per se. Free radicals also directly initiate elements of the apoptosis cascade by means of redox signaling .[8]
These processes are the same for any type of ischemic tissue and are referred to collectively as the ischemic cascade. However, brain tissue is especially vulnerable to ischemia since it has little respiratory reserve and is completely dependent on aerobic metabolism, unlike most other organs.
Brain tissue survival can be improved to some extent if one or more of these processes is inhibited. Drugs that scavenge Reactive oxygen species, inhibit apoptosis, or inhibit excitotoxic neurotransmitters, for example, have been shown experimentally to reduce tissue injury due to ischemia. Agents that work in this way are referred to as being neuroprotective. Until recently, human clinical trials with neuroprotective agents have failed, with the probable exception of deep barbiturate coma. However, more recently NXY-059, the disulfonyl derivative of the radical-scavenging spintrap phenylbutylnitrone, is reported be neuroprotective in stroke. This agent appears to work at the level of the blood vessel lining or endothelium. Unfortunately, after producing favorable results in one large-scale clinical trial, a second trial failed to show favorable results. [8]
In addition to injurious effects on brain cells, ischemia and infarction can result in loss of structural integrity of brain tissue and blood vessels, partly through the release of matrix metalloproteases, which are zinc- and calcium-dependent enzymes that break down collagen, hyaluronic acid, and other elements of connective tissue. Other proteases also contribute to this process. The loss of vascular structural integrity results in a breakdown of the protective blood brain barrier that contributes to cerebral edema, which can cause secondary progression of the brain injury.
As is the case with any type of brain injury, the immune system is activated by cerebral infarction and may under some circumstances exacerbate the injury caused by the infarction. Inhibition of the inflammatory response has been shown experimentally to reduce tissue injury due to cerebral infarction, but this has not proved out in clinical studies.
Hemorrhagic strokes result in tissue injury by causing compression of tissue from an expanding hematoma or hematomas. This can distort and injure tissue. In addition, the pressure may lead to a loss of blood supply to affected tissue with resulting infarction, and the blood released by brain hemorrhage appears to have direct toxic effects on brain tissue and vasculature.[8]
History and Symptoms
Warning Signs of CVA
- Sudden, severe headache with no known cause
- Sudden trouble seeing in one or both eyes
- Sudden confusion, trouble speaking or understanding
- Sudden numbness or weakness of the face, arm or leg, especially on one side of the body
- Sudden trouble walking, dizziness, loss of balance or coordination
The symptoms of stroke depend on the type of stroke and the area of the brain affected. Ischemic strokes usually only affect regional areas of the brain perfused by the blocked artery. Hemorrhagic strokes can affect local areas, but often can also cause more global symptoms due to bleeding and increased intracranial pressure.
If the area of the brain affected contains one of the three prominent Central nervous system pathways—the spinothalamic tract, corticospinal tract, and dorsal column (medial lemniscus), symptoms may include:
- muscle weakness (hemiplegia)
- numbness
- reduction in sensory or vibratory sensation
In most cases, the symptoms affect only one side of the body. The defect in the brain is usually on the opposite side of the body (depending on which part of the brain is affected). However, the presence of any one of these symptoms does not necessarily suggest a stroke, since these pathways also travel in the spinal cord and any lesion there can also produce these symptoms.
In addition to the above CNS pathways, the brainstem also consists of the 12 cranial nerves. A stroke affecting the brainstem therefore can produce symptoms relating to deficits in these cranial nerves:
- altered smell, taste, hearing, or vision (total or partial)
- drooping of eyelid (ptosis) and weakness of ocular muscles
- decreased reflexes: gag, swallow, pupil reactivity to light
- decreased sensation and muscle weakness of the face
- balance problems and nystagmus
- altered breathing and heart rate
- weakness in sternocleidomastoid muscle (SCM) with inability to turn head to one side
- weakness in tongue (inability to protrude and/or move from side to side)
If the cerebral cortex is involved, the CNS pathways can again be affected, but also can produce the following symptoms:
- aphasia (inability to speak or understand language from involvement of Broca's or Wernicke's area)
- apraxia (altered voluntary movements)
- visual field defect
- memory deficits (involvement of temporal lobe)
- hemineglect (involvement of parietal lobe)
- disorganized thinking, confusion, hypersexual gestures (with involvement of frontal lobe)
If the cerebellum is involved, the patient may have the following:
- trouble walking
- altered movement coordination
- vertigo and or disequilibrium
Loss of consciousness, headache, and vomiting usually occurs more often in hemorrhagic stroke than in thrombosis because of the increased intracranial pressure from the leaking blood compressing on the brain.
If symptoms are maximal at onset, the cause is more likely to be a subarachnoid hemorrhage or an embolic stroke.
Diagnosis
Stroke is diagnosed through several techniques: a neurological examination, blood tests, CT scans (without contrast enhancements) or MRI scans, Doppler ultrasound, and arteriography.
A systematic review by the Rational Clinical Examination found that acute facial paresis, arm drift, or abnormal speech are the best findings [10].
Imaging
For diagnosing ischemic stroke in the emergency setting [11]:
- CT scans (without contrast enhancements)
- sensitivity= 16%
- specificity= 96%
- sensitivity= 83%
- specificity= 98%
For diagnosing hemorrhagic stroke in the emergency setting:
- CT scans (without contrast enhancements)
- sensitivity= 89%
- specificity= 100%
- sensitivity= 81%
- specificity= 100%
For detecting hemorrhages, MRI scan is more sensitive.[12]
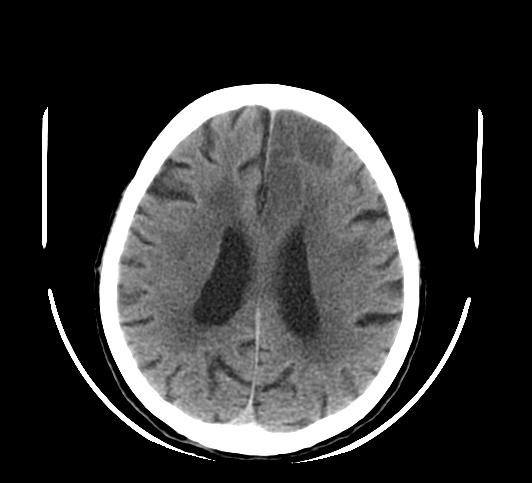
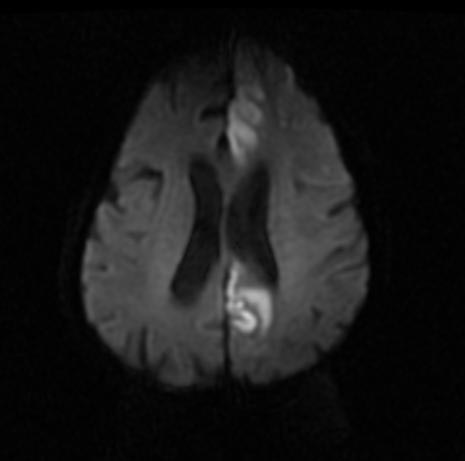
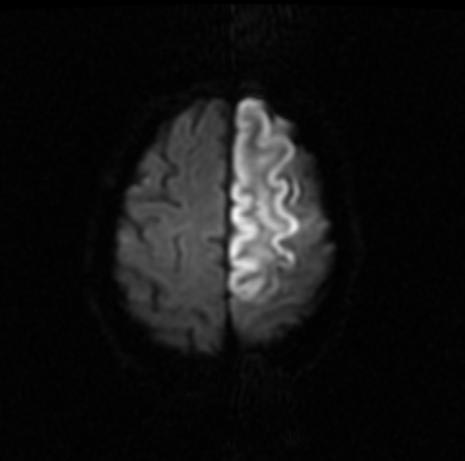
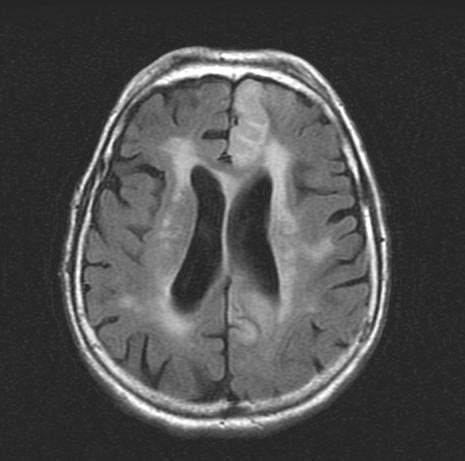
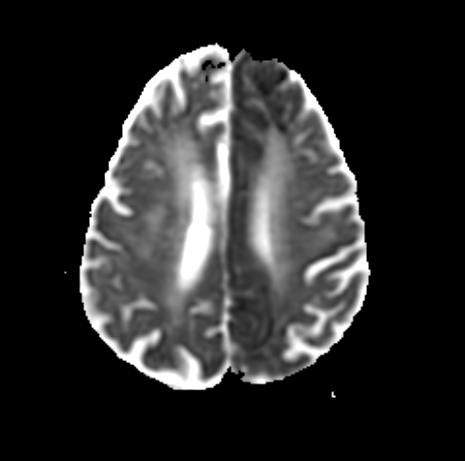
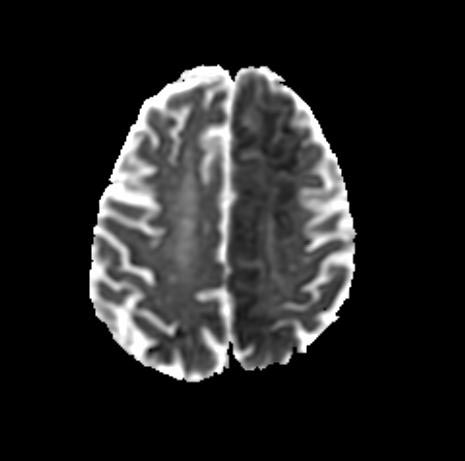
Patient No 1: Change in mental status
-

CT
-
MRI - DWI
-

MRI - FLAIR



-

MRI - T2
-

MRI - T1
-

MRI - ADC



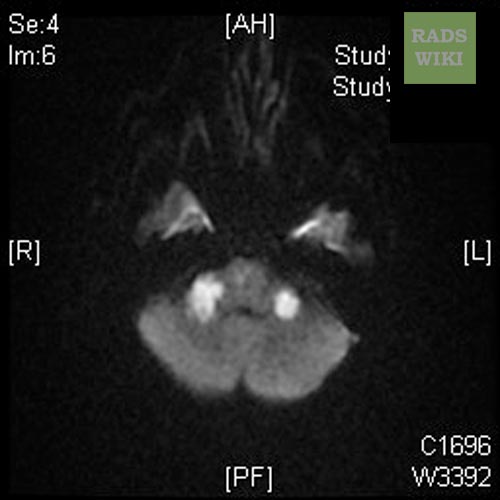
Patient No 2: Left ACA infarction
Images shown below are courtesy of RadsWiki
-
CT
-

CT


-
MRI- DWI
-

MRI- DWI


-

MRI- DWI
-
MRI- DWI


-
MRI- FLAIR
-

MRI- FLAIR


-
MRI- ADC
-
MRI- ADC


Other Diagnostic Studies
If a stroke is confirmed on imaging, various other studies may be performed to determine whether there is a peripheral source of emboli:
- an ultrasound/doppler study of the carotid arteries (to detect carotid stenosis)
- an electrocardiogram (ECG) and echocardiogram (to identify arrhythmias and resultant clots in the heart which may spread to the brain vessels through the bloodstream)
- a Holter monitor study to identify intermittent arrhythmias
- an angiogram of the cerebral vasculature (if a bleed is thought to have originated from an aneurysm or arteriovenous malformation)
Treatment
Early assessment
Early recognition of the signs of stroke is generally regarded as important. Only detailed physical examination and medical imaging provide information on the presence, type, and extent of stroke, and hence hospital attendance — even if the symptoms were brief — is advised.
Studies show that patients treated in hospitals with a dedicated Stroke Team or Stroke Unit and a specialized care program for stroke patients have improved odds of recovery.
Ischemic stroke
As ischemic stroke is due to a thrombus (blood clot) occluding a cerebral artery, a patient is given antiplatelet medication (aspirin, clopidogrel, dipyridamole), or anticoagulant medication (warfarin), dependent on the cause, when this type of stroke has been found. Hemorrhagic stroke must be ruled out with medical imaging, since this therapy would be harmful to patients with that type of stroke.
Whether thrombolysis is performed or not, the following investigations are required:
- Stroke symptoms are documented, often using scoring systems such as the National Institutes of Health Stroke Scale, the Cincinnati Stroke Scale, and the Los Angeles Prehospital Stroke Screen. The Cincinnati Stroke Scale is used by emergency medical technicians (EMTs) to determine whether a patient needs transport to a stroke center.
- A CT scan is performed to rule out hemorrhagic stroke
- Blood tests, such as a full blood count, coagulation studies (PT/INR and APTT), and tests of electrolytes, renal function, liver function tests and glucose levels are carried out.
Other immediate strategies to protect the brain during stroke include ensuring that blood sugar is as normal as possible (such as commencement of an insulin sliding scale in known diabetics), and that the stroke patient is receiving adequate oxygen and intravenous fluids. The patient may be positioned so that his or her head is flat on the stretcher, rather than sitting up, since studies have shown that this increases blood flow to the brain. Additional therapies for ischemic stroke include aspirin (50 to 325 mg daily), clopidogrel (75 mg daily), and combined aspirin and dipyridamole extended release (25/200 mg twice daily).
It is common for the blood pressure to be elevated immediately following a stroke. Studies indicated that while high blood pressure causes stroke, it is actually beneficial in the emergency period to allow better blood flow to the brain.
If studies show carotid stenosis, and the patient has residual function in the affected side, carotid endarterectomy (surgical removal of the stenosis) may decrease the risk of recurrence.
If the stroke has been the result of cardiac arrhythmia with cardiogenic emboli, treatment of the arrhythmia and anticoagulation with warfarin or high-dose aspirin may decrease the risk of recurrence. Stroke prevention treatment for a common arrhythmia, atrial fibrillation, is determined according to the CHADS/CHADS2 system.
Thrombolysis (tPA)
In increasing numbers of primary stroke centers, pharmacologic thrombolysis ("clot busting") with the drug Tissue plasminogen activator, tPA, is used to dissolve the clot and unblock the artery. However, the use of tPA in acute stroke is controversial. On one hand, it is endorsed by the American Heart Association and the American Academy of Neurology as the recommended treatment for acute stroke within three hours of onset of symptoms as long as there are not other contraindications (such as abnormal lab values, high blood pressure, or recent surgery). This position for tPA is based upon the findings of one study [13] which showed that tPA improves the chances for a good neurological outcome. When administered within the first three hours, 39% of all patients who were treated with tPA had a good outcome at three months, only 26% of placebo controlled patients had a good functional outcome. However, in the NINDS trial 6.4% of patients with large strokes developed substantial brain hemorrhage as a complication from being given tPA. tPA is often misconstrued as a "magic bullet" and it is important for patients to be aware that despite the study that supports its use, some of the data were flawed and the safety and efficacy of tPA is controversial. A recent study found the mortality to be higher among patients receiving tPA versus those who did not.[14] Additionally, it is the position of the American Academy of Emergency Medicine that objective evidence regarding the efficacy, safety, and applicability of tPA for acute ischemic stroke is insufficient to warrant its classification as standard of care. [15] Until additional evidence clarifies such controversies, physicians are advised to use their discretion when considering its use. Given the cited absence of definitive evidence, AAEM believes it is inappropriate to claim that either use or non-use of intravenous thrombolytic therapy constitutes a standard of care issue in the treatment of stroke.
Mechanical Thrombectomy
Another intervention for acute ischemic stroke is removal of the offending thrombus directly. This is accomplished by inserting a catheter into the femoral artery, directing it up into the cerebral circulation, and deploying a corkscrew-like device to ensnare the clot, which is then withdrawn from the body. In August 2004, based on data from the MERCI (Mechanical Embolus Removal in Cerebral Ischemia) Trial, the FDA cleared several of these devices, called the Merci X5 and X6 Retrievers.[16][17] The newer generation Merci L5 Retriever was cleared for thrombus removal in acute stroke based on data from the Multi MERCI trial.[18][19] Both the MERCI and Multi MERCI trials evaluated the use of mechanical thrombectomy up to 8 hours after onset of symptoms.
Embolic stroke
Anticoagulation can prevent recurrent stroke. Among patients with nonvalvular atrial fibrillation, anticoagulation can reduce stroke by 60% while antiplatelet agents can reduce stroke by 20%. [20]. However, a recent meta-analysis suggests harm from anti-coagulation started early after an embolic stroke.[21]
Hemorrhagic stroke

Patients with bleeding into (intracerebral hemorrhage) or around the brain (subarachnoid hemorrhage), require neurosurgical evaluation to detect and treat the cause of the bleeding. Anticoagulants and antithrombotics, key in treating ischemic stroke, can make bleeding worse and cannot be used in intracerebral hemorrhage. Patients are monitored and their blood pressure, blood sugar, and oxygenation are kept at optimum levels.
Care and rehabilitation
Stroke rehabilitation is the process by which patients with disabling strokes undergo treatment to help them return to normal life as much as possible by regaining and relearning the skills of everyday living. It also aims to help the survivor understand and adapt to difficulties, prevent secondary complications and educate family members to play a supporting role.
A rehabilitation team is usually multidisciplinary as it involves staff with different skills working together to help the patient. These include nursing staff, physiotherapy, occupational therapy, speech and language therapy, and usually a physician trained in rehabilitation medicine. Some teams may also include psychologists, social workers, and pharmacists since at least one third of the patients manifest post stroke depression.
Good nursing care is fundamental in maintaining skin care, feeding, hydration, positioning, and monitoring vital signs such as temperature, pulse, and blood pressure. Stroke rehabilitation begins almost immediately.
For most stroke patients, physical therapy (PT) and occupational therapy (OT) are the cornerstones of the rehabilitation process. Often, assistive technology such as a wheelchair, walkers, canes, and orthosis may be beneficial. PT and OT have overlapping areas of working but their main attention fields are; PT involves re-learning functions as transferring, walking and other gross motor functions. OT focusses on exercises and training to help relearn everyday activities known as the Activities of daily living (ADLs) such as eating, drinking, dressing, bathing, cooking, reading and writing, and toileting. Speech and language therapy is appropriate for patients with problems understanding speech or written words, problems forming speech and problems with eating (swallowing).
Patients may have particular problems, such as complete or partial inability to swallow, which can cause swallowed material to pass into the lungs and cause aspiration pneumonia. The condition may improve with time, but in the interim, a nasogastric tube may be inserted, enabling liquid food to be given directly into the stomach. If swallowing is still unsafe after a week, then a percutaneous endoscopic gastrostomy (PEG) tube is passed and this can remain indefinitely.
Stroke rehabilitation should be started as immediately as possible and can last anywhere from a few days to several months. Most return of function is seen in the first few days and weeks, and then improvement falls off with the "window" considered officially by U.S. state rehabilitation units and others to be closed after six months, with little chance of further improvement. However, patients have been known to continue to improve for years, regaining and strengthening abilities like writing, walking, running, and talking. Daily rehabilitation exercises should continue to be part of the stroke patient's routine. Complete recovery is unusual but not impossible and most patients will improve to some extent : a correct diet and exercise are known to help the brain to self-recover.
Prognosis
Disability affects 75% of stroke survivors enough to decrease their employability.[22] Stroke can affect patients physically, mentally, emotionally, or a combination of the three. The results of stroke vary widely depending on size and location of the lesion.[23] Dysfunctions correspond to areas in the brain that have been damaged.
Some of the physical disabilities that can result from stroke include paralysis, numbness, pressure sores, pneumonia, incontinence, apraxia (inability to perform learned movements), difficulties carrying out daily activities, appetite loss, vision loss, and pain. If the stroke is severe enough, or in a certain location such as parts of the brainstem, coma or death can result.
Emotional problems resulting from stroke can result from direct damage to emotional centers in the brain or from frustration and difficulty adapting to new limitations. Post-stroke emotional difficulties include anxiety, panic attacks, flat affect (failure to express emotions), mania, apathy, and psychosis.
30 to 50% of stroke survivors suffer post stroke depression, which is characterized by lethargy, irritability, sleep disturbances, lowered self esteem, and withdrawal.[24] Depression can reduce motivation and worsen outcome, but can be treated with antidepressants.
Emotional lability, another consequence of stroke, causes the patient to switch quickly between emotional highs and lows and to express emotions inappropriately, for instance with an excess of laughing or crying with little or no provocation. While these expressions of emotion usually correspond to the patient's actual emotions, a more severe form of emotional lability causes patients to laugh and cry pathologically, without regard to context or emotion.[22] Some patients show the opposite of what they feel, for example crying when they are happy.[25] Emotional lability occurs in about 20% of stroke patients.
Cognitive deficits resulting from stroke include perceptual disorders, speech problems, dementia, and problems with attention and memory. A stroke sufferer may be unaware of his or her own disabilities, a condition called anosognosia. In a condition called hemispatial neglect, a patient is unable to attend to anything on the side of space opposite to the damaged hemisphere.
Up to 10% of all stroke patients develop seizures, most commonly in the week subsequent to the event; the severity of the stroke increases the likelihood of a seizure[26][27].
Prevention
Risk factors and prevention
Prevention of stroke can work at various levels including:
- primary prevention - the reduction of risk factors across the board, by public health measures such as reducing smoking and the other behaviours that increase risk;
- secondary prevention - actions taken to reduce the risk in those who already have disease or risk factors that may have been identified through screening; and
- tertiary prevention - actions taken to reduce the risk of complications (including further strokes) in people who have already had a stroke.
The most important modifiable risk factors for stroke are hypertension, heart disease, diabetes, and cigarette smoking. Other risks include heavy alcohol consumption (see Alcohol consumption and health), high blood cholesterol levels, illicit drug use, and genetic or congenital conditions. Family members may have a genetic tendency for stroke or share a lifestyle that contributes to stroke. Higher levels of Von Willebrand factor are more common amongst people who have had ischemic stroke for the first time.[28] The results of this study found that the only significant genetic factor was the person's blood type. Having had a stroke in the past greatly increases one's risk of future strokes.
One of the most significant stroke risk factors is advanced age. 95% of strokes occur in people age 45 and older, and two-thirds of strokes occur in those over the age of 65.[24][8] A person's risk of dying if he or she does have a stroke also increases with age. However, stroke can occur at any age, including in fetuses.
Sickle cell anemia, which can cause blood cells to clump up and block blood vessels, also increases stroke risk. Stroke is the second leading killer of people under 20 who suffer from sickle-cell anemia.[8]
Men are 1.25 times more likely to suffer Cerebral Vascular Accidents than women,[8] yet 60% of deaths from stroke occur in women.[25] Since women live longer, they are older on average when they have their strokes and thus more often killed (NIMH 2002).[8] Some risk factors for stroke apply only to women. Primary among these are pregnancy, childbirth, menopause and the treatment thereof (HRT). Stroke seems to run in some families.
Prevention is an important public health concern. Identification of patients with treatable risk factors for stroke is paramount. Treatment of risk factors in patients who have already had strokes (secondary prevention) is also very important as they are at high risk of subsequent events compared with those who have never had a stroke. Medication or drug therapy is the most common method of stroke prevention. Aspirin (usually at a low dose of 75 mg) is recommended for the primary and secondary prevention of stroke. Also see Antiplatelet drug treatment. Treating hypertension, diabetes mellitus, smoking cessation, control of hypercholesterolemia, physical exercise, and avoidance of illicit drugs and excessive alcohol consumption are all recommended ways of reducing the risk of stroke.[29]
In patients who have strokes due to abnormalities of the heart, such as atrial fibrillation, anticoagulation with medications such as warfarin is often necessary for stroke prevention.[30]
Procedures such as carotid endarterectomy or carotid angioplasty can be used to remove significant atherosclerotic narrowing (stenosis) of the carotid artery, which supplies blood to the brain. These procedures have been shown to prevent stroke in certain patients, especially where carotid stenosis leads to ischemic events such as transient ischemic attack. (The value and role of carotid artery ultrasound scanning in screening has yet to be established.)
Case Examples
References
- ↑ Robbins and Cotran's Pathological Basis of Disease, 7th edition (2005), p.1361.
- ↑ headaches.about.com
- ↑ Cerebrovascular disorders: a clinical and research classification, WHO Offset Publication No. 43, 1978
- ↑ MedlinePlus: Stroke a risk for cocaine, amphetamine abusers
- ↑ 5.0 5.1 Ay H; Furie KL; Singhal A; Smith WS; Sorensen AG; Koroshetz WJ (2005). "An evidence-based causative classification system for acute ischemic stroke". Ann Neurol. 58 (5): 688–97. PMID 16240340.
- ↑ 6.0 6.1 Thompson JE (1996). "The evolution of surgery for the treatment and prevention of stroke. The Willis Lecture". Stroke. 27 (8): 1427–34. PMID 8711815.
- ↑ Kopito, Jeff (2001). "A Stroke in Time". MERGINET.com (Number 9). Unknown parameter
|Volume=ignored (|volume=suggested) (help); Unknown parameter|month=ignored (help) - ↑ 8.0 8.1 8.2 8.3 8.4 8.5 8.6 8.7 8.8 National Institute of Neurological Disorders and Stroke (NINDS) (1999). "Stroke: Hope Through Research". National Institutes of Health.
- ↑ R. Barnhart, ed. The Barnhart Concise Dictionary of Etymology (1995)
- ↑ Goldstein L, Simel D (2005). "Is this patient having a stroke?". JAMA. 293 (19): 2391–402. doi:10.1001/jama.296.16.2012. PMID 15900010.
- ↑ Chalela J, Kidwell C, Nentwich L, Luby M, Butman J, Demchuk A, Hill M, Patronas N, Latour L, Warach S (2007). "Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison". Lancet. 369 (9558): 293–8. PMID 17258669.
- ↑ Kidwell C, Chalela J, Saver J, Starkman S, Hill M, Demchuk A, Butman J, Patronas N, Alger J, Latour L, Luby M, Baird A, Leary M, Tremwel M, Ovbiagele B, Fredieu A, Suzuki S, Villablanca J, Davis S, Dunn B, Todd J, Ezzeddine M, Haymore J, Lynch J, Davis L, Warach S (2004). "Comparison of MRI and CT for detection of acute intracerebral hemorrhage". JAMA. 292 (15): 1823–30. PMID 15494579.
- ↑ (NINDS; N Engl J Med 1995;333:1581–1587.[1])
- ↑ Dubinsky, R (2006). "Mortality of stroke patients treated with thrombolysis: analysis of nationwide inpatient sample". Neurology. 66 (11): 1742–1744. PMID 16769953. Unknown parameter
|coauthors=ignored (help);|access-date=requires|url=(help) - ↑ (http://www.aaem.org/positionstatements/thrombolytictherapy.shtml)
- ↑ Smith WS, Sung G, Starkman S, Saver JL, Kidwell CS, Gobin YP, Lutsep HL, Nesbit GM, Grobelny T, Rymer MM, Silverman IE, Higashida RT, Budzik RF, Marks MP; MERCI Trial Investigators (2005). "Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial". Stroke. 2005 Jul;36(7):1432–8.
- ↑ Celia Witten (2004). "Concentric Merci Retriever product licence" (PDF). FDA.
- ↑ W. Smith (2006). "Safety of mechanical thrombectomy and intravenous tissue plasminogen activator in acute ischemic stroke. Results of the multi Mechanical Embolus Removal in Cerebral Ischemia (MERCI) trial, part I". AJNR Am J Neuroradiol. 2006 Jun-Jul;27(6):1177–82.
- ↑ W. Smith (2006). "Mechanical Intervention for Ischemic Stroke". Touch Briefings.
- ↑ Hart RG, Pearce LA, Aguilar MI (2007). "Meta-analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation". Ann. Intern. Med. 146 (12): 857–67. PMID 17577005.
- ↑ Paciaroni M, Agnelli G, Micheli S, Caso V (2007). "Efficacy and safety of anticoagulant treatment in acute cardioembolic stroke: a meta-analysis of randomized controlled trials". Stroke. 38 (2): 423–30. doi:10.1161/01.STR.0000254600.92975.1f. PMID 17204681. ACP JC synopsis
- ↑ 22.0 22.1 Coffey C. Edward, Cummings Jeffrey L, Starkstein Sergio, Robinson Robert (2000). Stroke - The American Psychiatric Press Textbook of Geriatric Neuropsychiatry (Second Edition ed.). Washington DC: American Psychiatric Press. pp. 601–617.
- ↑ Stanford Hospital & Clinics. "Cardiovascular Diseases: Effects of Stroke". Unknown parameter
|accessyear=ignored (|access-date=suggested) (help) - ↑ 24.0 24.1 Senelick Richard C., Rossi, Peter W., Dougherty, Karla (1994). Living with Stroke: A Guide For Families. Contemporary Books, Chicago.
- ↑ 25.0 25.1 Villarosa, Linda, Ed., Singleton, LaFayette, MD, Johnson, Kirk A. (1993). Black Health Library Guide to Stroke. Henry Holt and Company, New York.
- ↑ Reith J, Jorgensen HS, Nakayama H, Raaschou HO, Olsen TS. Seizures in acute stroke: predictors and prognostic significance. The Copenhagen Stroke Study. Stroke 1997;28:1585–9. PMID 9259753.
- ↑ Burn J, Dennis M, Bamford J, Sandercock P, Wade D, Warlow C. Epileptic seizures after a first stroke: the Oxfordshire Community Stroke Project. BMJ 1997;315:1582–7. PMID 9437276.
- ↑ Bongers T, de Maat M, van Goor M, et. al (2006). "High von Willebrand factor levels increase the risk of first ischemic stroke: influence of ADAMTS13, inflammation, and genetic variability". Stroke. 37 (11): 2672–7. PMID 16990571.
- ↑ American Heart Association. (2007). Stroke Risk Factors Americanheart.org. Retrieved on January 22, 2007.
- ↑ American Heart Association. (2007). Atrial Fibrillation Americanheart.org. Retrieved on January 22, 2007.
Suggested Revisions to the Current Guidelines
- Update to the AHA/ASA Recommendations for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack. DOI: 10.1161/STROKEAHA.107.189063 Stroke. 2008; 39:000-000 (Published online on 05.March.2008)
Acknowledgements
The content on this page was first contributed by
List of contributors:
Suggested Reading and Key General References
- J. P. Mohr, Dennis Choi, James Grotta, Philip Wolf (2004). Stroke: Pathophysiology, Diagnosis, and Management. New York: Churchill Livingstone. ISBN 0-443-06600-0.
- Perry, Thomas and Miller Frank (1961). 'Pathology: A Dynamic Introduction to Medicine and Surgery. Boston: Little, Brown and Company.
Suggested Links and Web Resources
- The original text of this article is taken from National Institute of Neurological Disorders and Stroke
- Canadian Stroke Network
- Registry of the Canadian Stroke Network
- StrokEngine McGill University, Montreal, Quebec, Canada. Focuses on stroke rehabilitation and interventions
- Cerebrovascular disease and risk of stroke
- What Happens During a Stroke?
- American Stroke Association
- National Stroke Association
- Heart and Stroke Foundation of Canada
- The Stroke Association
- "Heart Attack, Stroke and Cardiac Arrest Warning Signs," from the American Heart Association
- StrokeMD.net
- National Stroke Association of Malaysia
- Study of Outcome of Childhood Stroke
- Update to the AHA/ASA Recommendations for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack March 2008