Ankylosing spondylitis: Difference between revisions
| Line 154: | Line 154: | ||
Changes in the upper airway can lead to difficulties in intubating the airway, spinal and epidural anaesthesia may be difficult due to calicification of ligaments, and a small number have aortoc insufficiency. The stiffness of the thoracic ribs results in ventilation being mainly diaphragm-driven, so there may be a decrease in pulmonary function. | Changes in the upper airway can lead to difficulties in intubating the airway, spinal and epidural anaesthesia may be difficult due to calicification of ligaments, and a small number have aortoc insufficiency. The stiffness of the thoracic ribs results in ventilation being mainly diaphragm-driven, so there may be a decrease in pulmonary function. | ||
=== | ===[[Ankylosing Spondylitis physical therapy]]=== | ||
All physical therapies must be approved in advance by a rheumatologist, since movements that normally have great benefits on one's health, may harm a patient with AS: massages and physical manipulations should be practiced by therapists familiar with this disease. | All physical therapies must be approved in advance by a rheumatologist, since movements that normally have great benefits on one's health, may harm a patient with AS: massages and physical manipulations should be practiced by therapists familiar with this disease. | ||
* [[Physical therapy]] has been shown to be of great benefit to AS patients; | * [[Physical therapy]] has been shown to be of great benefit to AS patients; | ||
Revision as of 18:58, 1 March 2012
For patient information click here
Template:DiseaseDisorder infobox
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Synonyms and keywords: Ankylosing spondylitis, AS, Bechterew's disease, Bechterew syndrome, Marie Strümpell disease, Marie Struempell disease, Spondyloarthritis
Overview
Ankylosing spondylitis is a chronic, painful, degenerative inflammatory arthritis primarily affecting spine and sacroiliac joints, causing eventual fusion of the spine; it is a member of the group of the autoimmune spondyloarthropathies with a probable genetic predisposition. Complete fusion results in a complete rigidity of the spine, a condition known as bamboo spine.[1]
Epidemiology
The gender ratio is 3:1 for men:women. In USA, the prevalence is 0.25%, but as it is a chronic condition the incidence (number of new cases) is fairly low.
Pathophysiology
AS is a systemic rheumatic disease, and is one of the seronegative spondyloarthropathies. About 90% of the patients express the HLA-B27 genotype. Tumor necrosis factor-alpha (TNF α) and IL-1 are also implicated in ankylosing spondylitis. Although specific autoantibodies cannot be detected, its response to immunosuppresive medication has prompted its classification as an autoimmune disease.
Hypotheses on its pathogenesis include a cross-reaction with antigens of the Klebsiella bacterial strain (Tiwana et al. 2001).[2] Particular authorities argue that elimination of the prime nutrients of Klebsiella (starches) would decrease antigenemia and improve the musculoskeletal symptoms. On the other hand, Khan (2002) argues that the evidence for a correlation between Klebsiella and AS is circumstantial so far, and that the efficacy of low-starch diets has not yet been scientifically evaluated.[3] Similarly, Toivanen (1999) found no support for the role of klebsiella in the etiology of primary AS.[4]
History

AS was probably first recognized as a disease which was different from Rheumatoid arthritis by Galen as early as the second century AD[5]; however, skeletal evidence of the disease (ossification of joints and entheses primarily of the axial skeleton, known as "bamboo spine") were first discovered in an archaeological dig that unearthed the skeletal remains of a 5000 year–old Egyptian mummy with evidence of "bamboo spine".[6]
The anatomist and surgeon Realdo Colombo described what could have been the disease in 1559,[7] and the first account of pathologic changes to the skeleton possibly associated with AS was published in 1691 by Bernard Connor.[8] In 1818, Benjamin Collins Brodie became the first physician to document that iritis accompanied what is believed to have been a patient with active AS.[9]
In 1858, David Tucker published a small booklet which clearly described a patient by the name of Leonard Trask who suffered from severe spinal deformity subsequent to AS.[10][11]
In 1833 Trask fell from a horse, exacerbating the condition and resulting in severe deformity. Tucker reported that
| “ | It was not until he [Trask] had exercised for some time that he could perform any labor [..., and that] his neck and back have continued to curve drawing his head downward on his breast. | ” |
evidence of inflammatory disease characteristics of AS, and the hallmark of deforming injury in AS. This account became the first documented case of AS in the United States.
It was not until the late nineteenth century (1893-1898), however, when the neurophysiologist Vladimir Bekhterev of Russia in 1893,[12] Adolph Strümpell of Germany in 1897,[13] and Pierre Marie of France in 1898,[14] were the first to give adequate descriptions which permitted an accurate diagnosis of AS prior to severe spinal deformity. For this reason, AS is also known as Bechterew Disease or Marie–Strümpel Disease.
Signs and symptoms
The typical patient is young, of 15 to 30 years of age with chronic pain and stiffness in the lower part of the spine. Men are affected more than women by a ratio in excess of 2:1.[15] In 40% of cases, ankylosing spondylitis is associated with iridocyclitis (anterior uveitis, also known as iritis) causing eye pain and photophobia (increased sensitivity to light). Other common symptoms are recurring mouth ulcers (aphthae) and fatigue. Pain fluctuation from one side to the other.
Typical prodromes (early symptoms) may occur at a very young age (e.g. 3 years old), where the patient may experience recurring painful joints (e.g. knees, elbows), commonly misinterpreted as simple rheumatism.
AS is also associated with ulcerative colitis, Crohn's disease, psoriasis, and Reiter's disease.
Diagnosis

There is no direct test to diagnose AS. A clinical examination and X-ray studies of the spine, which show characteristic spinal changes and sacroiliitis, are the major diagnostic tools. A drawback of X-ray diagnosis is that signs and symptoms of AS have usually been established as long as 8-10 years prior to X-ray evident changes occurring on a plain film X-ray, which means a delay of as long as 10 years before adequate therapies can be introduced. An option for more accurate (and much earlier) diagnosis are tomography and magnetic resonance imaging of the sacroiliac joints. The Schober's test is a useful clinical measure of flexion of the lumbar spine performed during examination.[16]
During acute inflammatory periods, AS patients will usually show an increase in the blood concentration of C-reactive protein (CRP) and an increase in the erythrocyte sedimentation rate (ESR).
Variations of the HLA-B gene increase the risk of developing ankylosing spondylitis, although it is not a diagnostic test. Those with the HLA-B27 variant are at highest risk of developing the disorder. HLA-B27, demonstrated in a blood test, is occasionally used as a diagnostic, but does not distinguish AS from other diseases and is therefore not of real diagnostic value. Over 95% of people with AS are HLA-B27 positive, although this ratio varies from population to population (only 50% of African American patients with AS possess HLA-B27, and it is close to 80% among AS patients from Mediterranean countries).
The Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), developed in Bath (Somerset,UK) is an index designed to detect the inflammatory burden of active disease. The BASDA can help to establish a diagnosis of AS in the presence of other factors such as HLA-B27 positivity, persistent buttock pain which resolves with exercise, and X-ray or MRI evident involvement of the sacroiliac joints. (See: "Diagnostic Tools", below)[17] It can be easily calculated and accurately assesses a patient's need for additional therapy; a score of 4 out of a possible 10 points while on adequate NSAID therapy is usually considered a good candidate for biologic therapy.
The Bath Ankylosing Spondylitis Functional Index (BASFI) is a functional index which can accurately assess a patient's functional impairment due to the disease, as well as improvements following therapy. (See: "Diagnostic Tools", below)[18] The BASFI is not usually used as a diagnostic tool, but as a tool to establish a patient's current baseline and subsequent response to therapy.
Diagnostic Findings
- recognition of minimally displaced fractures is difficult due to osteopenia and deformity
- important to specifically search for disk space widening and discontinuity of the ossified paraspinal ligaments
- with CT, sagittal reformats should be obtained as axial images poorly assess the transverse fracture plane
- MR and radionuclide scintigraphy may be helpful in difficult cases
Radiograph

- indistinct joints
- joints widen before narrow
- subchondral erosions, sclerosis, and proliferation on iliac side of SI joints
- at endstage, sacroiliac joint may be a thin line or not visible
- in the spine, early spondylitis is characterized by small erosions at the corners of vertebral bodies with reactive sclerosis
- squaring of the vertebral body
- syndesmophyte formation, with bridging of the corners of one vertebra to another
- ossification of paravertebral connective tissue fibers, including posterior interspinous ligaments as well as linking of spinous processes leads to an appearance of a solid midline vertical dense line on AP projection
- may see associated pseudoarthroses (discovertebral destruction with adjacent sclerosis) and enthesopathic changes (ill-defined erosions with adjacent sclerosis at sites of ligamentous and tendenous attachments)
- hip involvement is generally bilateral and symmetric, with uniform joint space narrowing, axial migration of the femoral head, and a collar of osteophytes at the femoral head-neck junction
- knees demonstrate uniform joint space narrowing with bony proliferation
- hands are generally involved asymmetrically, with smaller, shallower erosions and marginal periostitis.
- radiographs of the lungs may demonstrate progressive fibrosis and bullous changes at the apices. These lesions may resemble TB infection and bullae may become infected.
CT
- may be useful in selected patients with normal or equivocal findings on sacroiliac joint radiographs
- joint erosions, subchondral sclerosis, and bony ankylosis are better visualized on CT
- some normal variants of the SI joints may mimic features of sacroiliitis
- CT supplements scintigraphy in evaluated areas of increased uptake
- multidetector CT is superior to radiographs and MRI in demonstrating injuries
- MDCT is imaging modality of choice in patients with advanced ankylosing spondylitis for whom there is suspicion of cervical spine fracture
MRI
- May have a role in early diagnosis of sacroiliitis
- Synovial enhancement on MR correlates with disease activity measured by inflammatory mediators
- Superior to CT in detection of cartilage, bone erosions, and subchondral bone changes
- Increased T2 signal correlates with edema or vascularized fibrous tissue
- Useful in following treatment results in patients with active ankylosing spondylitis
Bone scintigraphy
- May be helpful in selected patients with normal or equivocal findings on sacroiliac joint radiographs
- Qualitative assessment of accumulation of radionuclides in the SI joints may be difficult due to normal uptake in this location. Thus quantitative analysis may be more useful.
- Ratios of SI joint to sacral uptake of 1.3:1 or higher is abnormal
(Images courtesy of RadsWiki)
-

AS with dural ectasia
-

AS with dural ectasia
-

AS with dural ectasia



-

Bamboo Spine
-

Bamboo Spine


-

Symmetrical sacroiliac joint fusion
-
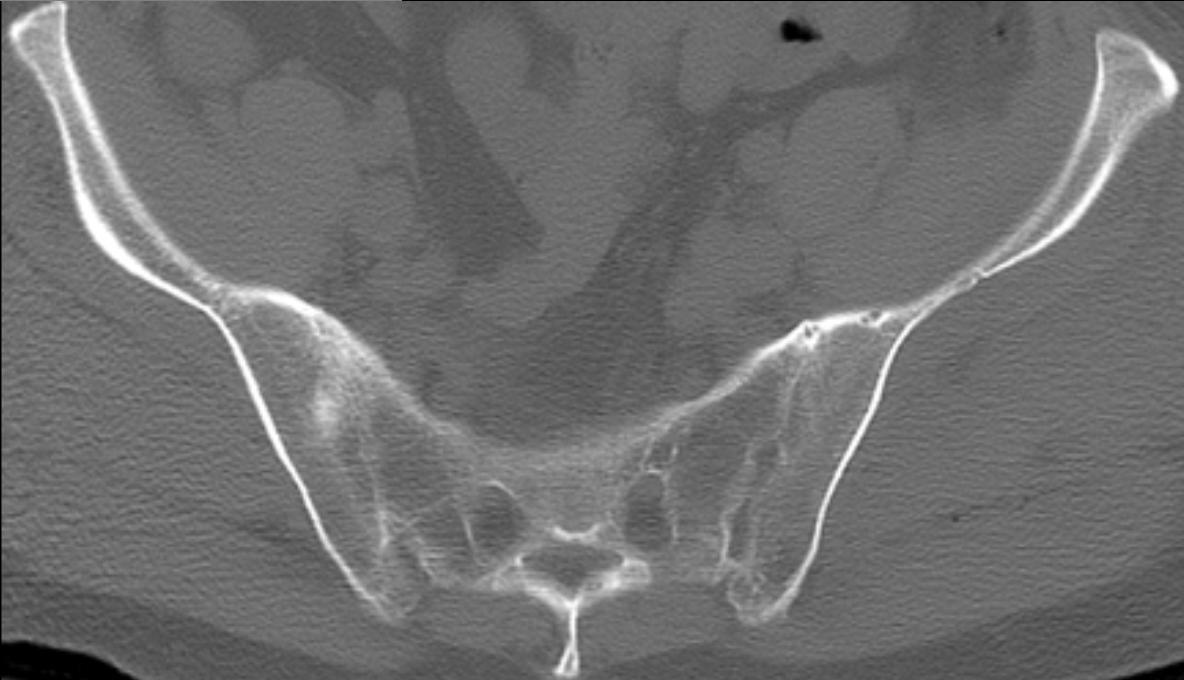
Symmetrical sacroiliac joint fusion


Therapy
No cure is known for AS, although treatments and medications are available to reduce symptoms and pain.
Physical therapy and exercise, along with medication, are at the heart of therapy for ankylosing spondylitis. Physiotherapy and physical exercises are clearly preceded by medical treatment in order to reduce the inflammation and pain, and commonly followed by a physician. This way the movements will help in diminishing pain and stiffness, while exercises in an active inflammatory state will just make the pain worse.
Patients who are able to do so, lie flat on their face or back on the floor for a prescribed cumulative period of time each week, to prevent the chronic stooping which may otherwise result.[19]
Medication
There are three major types of medications used to treat ankylosing spondylitis.
- NSAIDs such as aspirin, ibuprofen, indometacin, naproxen and COX-2 inhibitors, which reduce inflammation and pain. These drugs tend to have a personal response to the pain and inflammation, although commonly used anti-inflammatory drugs like nimesulide are less effective than others;
- DMARDs such as cyclosporin, methotrexate, sulfasalazine, and corticosteroids, used to reduce the immune system response through immunosuppression;
- TNFα blockers (antagonists) such as etanercept, infliximab and adalimumab (also known as biologics), are indicated for the treatment of and are effective immunosuppressants in AS as in other autoimmune diseases;
TNFα blockers have been shown to be the best promising treatment, slowing the progress of AS in the majority of clinical cases. They have also been shown to be highly effective in treating not only the arthritis of the joints but the spinal arthritis associated with AS. A drawback is the fact that these drugs increase the risk of infections. For this reason, the protocol for any of the TNF-α blockers include a test for tubercolosis (like Mantoux or Heaf) before starting treatment. In case of recurrent infections, like even recurrent sore throats, the therapy may be suspended due to the involved immunosuppression.
Surgery
In severe cases of AS, surgery can be an option in the form of joint replacements, particularly in the knees and hips. Surgical correction is also possible for those with severe flexion deformities (severe downward curvature) of the spine, particularly in the neck, although this procedure is considered risky.
In addition, AS can have some manifestations which make anaesthesia more complex.
Changes in the upper airway can lead to difficulties in intubating the airway, spinal and epidural anaesthesia may be difficult due to calicification of ligaments, and a small number have aortoc insufficiency. The stiffness of the thoracic ribs results in ventilation being mainly diaphragm-driven, so there may be a decrease in pulmonary function.
Ankylosing Spondylitis physical therapy
All physical therapies must be approved in advance by a rheumatologist, since movements that normally have great benefits on one's health, may harm a patient with AS: massages and physical manipulations should be practiced by therapists familiar with this disease.
- Physical therapy has been shown to be of great benefit to AS patients;
- Swimming is one of the preferred exercises since it involves all muscles and joints in a low gravity environment;
- Slow movements exercises like stretching, yoga, tai chi;
- Any physical movement like, jogging, Pilates|Pilates method, etc.
Alternative medicine
Although the effectiveness of alternative medicines has not been proved by any clinical trial, some patients find some relief in adding these alternative treatments to the medicaments and physical exercises, like a starch free diet[20] (also known as the No Starch Diet or NSD[21]). Some patients may find relief under acupuncture treatments. This is administered at various points directly on the spine where the pain is located, although efficacy is uncertain. Herbal medicine, may also relieve pain, partly due to placebo effect.[22]
Prognosis
AS can range from mild to progressively debilitating, and from medically controlled to refractive.
Unattended cases of AS normally lead to knee pain, and may be accompanied by dactylitis or enthesitis, which may result in a misdiagnosis of normal rheumatism. In a long-term undiagnosed period, osteopenia or osteoporosis of AP spine may occur, causing eventual compression fractures and a back "hump" if untreated. Typical signs of progressed AS are the visible formation of syndesmophytes on X-rays, an abnormal bone outgrowth similar to osteophytes, affecting the spine. Due to the fusion of the vertrbrae paresthesia is a complication due to the inflammation of the tissue surrounding nerves.
Organs affected by AS, other than the axial spine and other joints, are commonly the heart, lungs, colon, and kidney. Other complications are Aortic regurgitation, Achilles tendinitis, AV node block and Amyloidosis. Due to lung fibrosis, chest X-rays may show apical fibrosis while pulmonary function testing may reveal a restrictive lung defect. Very rare complications involve neurologic conditions such as the cauda equina syndrome.[23]
See also
- NASC, North American AS federation
- NIAMS the National Institute of Arthritis and Musculoskeletal and Skin Diseases
- SAA, Spondylitis Association of America
References
- ↑ Jiménez-Balderas FJ, Mintz G. (1993). "Ankylosing spondylitis: clinical course in women and men". J Rheumatol. 20 (12): 2069–72. PMID 7516975.
- ↑ Tiwana H, Natt R, Benitez-Brito R, Shah S, Wilson C, Bridger S, Harbord M, Sarner M, Ebringer A (2001). "Correlation between the immune responses to collagens type I, III, IV and V and Klebsiella pneumoniae in patients with Crohn's disease and ankylosing spondylitis". Rheumatology (Oxford). 40 (1): 15–23. PMID 11157137.
- ↑ Khan MA. (2002). Ankylosing spondylitis: The facts. Oxford University Press. ISBN 0-19-263282-5.
- ↑ Toivanen P, Hansen D, Mestre F, Lehtonen L, Vaahtovuo J, Vehma M, Möttönen T, Saario R, Luukkainen R, Nissilä M (1999). "Somatic serogroups, capsular types, and species of fecal Klebsiella in patients with ankylosing spondylitis". J Clin Microbiol. 37 (9): 2808–12. PMID 10449457.
- ↑ Dieppe P (1988). "Did Galen describe rheumatoid arthritis?". Annals of the Rheumatic Diseases. 47: 84–87.
- ↑ Calin A. (1985). "Ankylosing spondilitis". Clinics in Rheumatic Diseases. 11: 41–60.
- ↑ Pierre Marie (1995). "Benoist M. - Historical Perspective". Spine. 20: 849–852.
- ↑ Blumberg BS (1958). "?". Arch Rheum. 1: 553.
- ↑ Leden I (1994). "Did Bechterew describe the disease which is named after him? A question raised due to the centennial of his primary report". Scand J Rheumatol. 23 (1): 42–5. PMID 8108667.
- ↑ "Life and sufferings of Leonard Trask" (PDF for registered members)). Ankylosing Spondylitis Information Matrix.
- ↑ "Life and sufferings of Leonard Trask".
- ↑ Bechterew W. (1893). "Steifigkeit der Wirbelsaule und ihre Verkrummung als besondere Erkrankungsform". Neurol Centralbl. 12: 426–434.
- ↑ Strumpell A. (1897). "Bemerkung uber die chronische ankylosirende Entzundung der Wirbelsaule und der Huftgelenke". Dtsch Z Nervenheilkd. 11: 338–342.
- ↑ Marie P. (1898). "Sur la spondylose rhizomelique". Rev Med. 18: 285–315.
- ↑ http://www.spondylitis.org/patient_resources/women.aspx
- ↑ Thomas E, Silman AJ, Papageorgiou AC, Macfarlane GJ, Croft PR. (1998). "Association between measures of spinal mobility and low back pain. An analysis of new attenders in primary care". Spine. 23 (2): 343–7. PMID 9507623.
- ↑ Garrett S, Jenkinson T, Kennedy L, Whitelock H, Gaisford P, Calin A (1994). "A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index". J Rheumatol. 21 (12): 2286–91. PMID 7699630.
- ↑ Calin A, Garrett S, Whitelock H, Kennedy L, O'Hea J, Mallorie P, Jenkinson T (1994). "A new approach to defining functional ability in ankylosing spondylitis: the development of the Bath Ankylosing Spondylitis Functional Index". J Rheumatol. 21 (12): 2281–5. PMID 7699629.
- ↑ "Remicade.com". Living with Ankylosing Spondylitis. Retrieved 2007-01-11.
- ↑ Ebringer A, Wilson C (1996). "The use of a low starch diet in the treatment of patients suffering from ankylosing spondylitis". Clin Rheumatol. 15 Suppl 1: 62–66. PMID 8835506. Unknown parameter
|month=ignored (help) - ↑ http://www.kickas.org/ubbthreads/postlist.php?Board=starch 'No Starch Diet'
- ↑ http://www.nlm.nih.gov/medlineplus/news/fullstory_51426.html National Institute of Health
- ↑ Nicholas U. Ahn, Uri M. Ahn, Elizabeth S. Garrett; et al. (2001). "Cauda Equina Syndrome in AS (The CES-AS Syndrome): Meta-analysis of outcomes after medical and surgical treatments". J of Spinal Disorders. 14 (5): 427–433. PMID 11586143.
Additional Reading
- Baraliakos, X, Landewé, R, Hermann, KG, et al. Inflammation in ankylosing spondylitis: a systematic description of the extent and frequency of acute spinal changes using magnetic resonance imaging. Ann Rheum Dis 2005 May; 64(5): 730-4.
- Bennett, D.L., Ohashi, K., El-Khoury, G.Y. Spondyloarthropathies: ankylosing spondylitis and psoriatic arthritis. Radiol Clin North Am 2004 Jan; 42(1): 121-34.
- Cawley, M.I., Chalmers, T.M., Kellgren, J.H., Ball, J. Destructive lesions of vertebral bodies in ankylosing spondylitis. Ann Rheum Dis 1972 Sep; 31(5): 345-58.
- Dihlmann, W. Current radiodiagnostic concept of ankylosing spondylitis. Skeletal Radiol 1979; 4(4): 179-88.
- Fam, A.G., Rubenstein, J.D., Chin-Sang, H., Leung, F.Y. Computed tomography in the diagnosis of early ankylosing spondylitis. Arthritis Rheum 1985 Aug; 28(8): 930-7.
- Graham, B., Van Peteghem, P.K. Fractures of the spine in ankylosing spondylitis. Diagnosis, treatment, and complications. Spine 1989 Aug; 14(8): 803-7.
- Hanson, J.A., and Mirza, S. Predisposition for spinal fracture in ankylosing spondylitis. AJR 2000; 174:150.
- Karasick, D., Schweitzer, M.E., Abidi, N.A., Cotler, J.M. Fractures of the vertebrae with spinal cord injuries in patients with ankylosing spondylitis: imaging findings. AJR Am J Roentgenol 1995 Nov; 165(5): 1205-8.
External links
National organizations
- The Ankylosing Spondylitis group Australia
- Vlaamse Vereniging voor Bechterew-Patiënten vzw Belgium
- Associazione Italiana per la Lotta alla Spondilite Anchilosante Italy
- National Ankylosing Spondylitis Society UK
- Spondylitis Association of America USA
Diagnostic tools
- Bath Ankylosing Spondylitis Disease Activity Index Calculator BASDAI
- Bath Ankylosing Spondylitis Functional Index Calculator BASFI
Support groups
Current research
Template:Diseases of the musculoskeletal system and connective tissue
cs:Bechtěrevova nemoc
de:Spondylitis ankylosans
he:דלקת חוליות מקשחת
nl:Ziekte van Bechterew
no:Bekhterevs sykdom
fi:Selkärankareuma
sv:Ankyloserande spondylit