The EKG of cardiac transplantation
(Redirected from The EKG of Cardiac Transplantation)
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
General Specifications
- The recipient retains the posterior walls of his own atria.
- The recipient's atria are vascularized by bronchial collateral vessels.
- The transplanted heart is denervated and lacks autonomic neural control.
- The EKG changes in these patients are mainly due to the remnant activity of the recipients atria, injury to the donor heart during the transplant procedure, and increased PVR in the recipient.
- Atrial arrhythmias and ventricular conduction defects are common.
- Role of the ECG in acute rejection is controversial.
- MI may occur as a result of accelerated atherogenesis.
EKG Findings
- Two sets of P waves
- the recipients native P waves are of a small amplitude
- donor P waves have normal amplitude and configuration
- the suture line between the donor and the recipient atria blocks any interchange of the electrical impulses from the two sources. Atrial dissociation is present.
- the donor P wave is conducted and stimulates the ventricles. The recipients atrial impulses are not conducted.
- the rate of the denervated donor's heart is faster than that of the recipient's atrial remnant rate.
- in one series, two sets of P waves were identified in 86% of patients.
- P waves of the recipient atrial remnants may not be seen because of their small amplitude or the presence of sinus node dysfunction or atrial fibrillation prior to the transplantation. May also lose the sinus node artery during surgery.
- a. fib/flutter may be present in one set of atria while NSR is present in the other pair making interpretation difficult.
- RBBB (complete or incomplete)
- occurs in 83% of patients in Chou's experience, in 45% in another series.
- LAHB
- occurs in about 25% of patients
- Bradyarrhythmias due to sinus node dysfunction
- cause not explained by rejection or ischemic time during transplant
- subsidiary pacemakers may be unreliable in providing an escape rhythm and sudden death may occur.
- permanent pacemaker may be required.
- PACs, PSVTs, afib and aflutter are seen postoperatively. Some investigators have felt that these episodes are associated with rejection episodes.
- Presence of complex VEA is associated with accelerated atherosclerosis and early death.
- ST-segment and T-wave changes
- some patients may develop diffuse ST-segment elevation followed by evolutionary changes of the ST segment and T wave changes consistent with acute pericarditis in the early post-operative period.
- as a rule these changes are transient
- some patients develop ischemic appearing ST T wave changes and these are not associated with evidence of acute rejection and their angiograms are normal.
ECG Evidence of Rejection
- Originally though that low voltage was indicative of rejection, but this has been called into question.
Accelerated Atherogenesis
- 40% of patients have this after three years.
- Equally frequent in those who did and did not have ischemic heart disease at the time of transplantation.
- Immunologic damage to the coronary endothelium is thought to be the mechanism of injury.
- Is a mixture of ordinary proximal lesions and diffuse obliterative disease.
- Usually silent because of denervation.
-
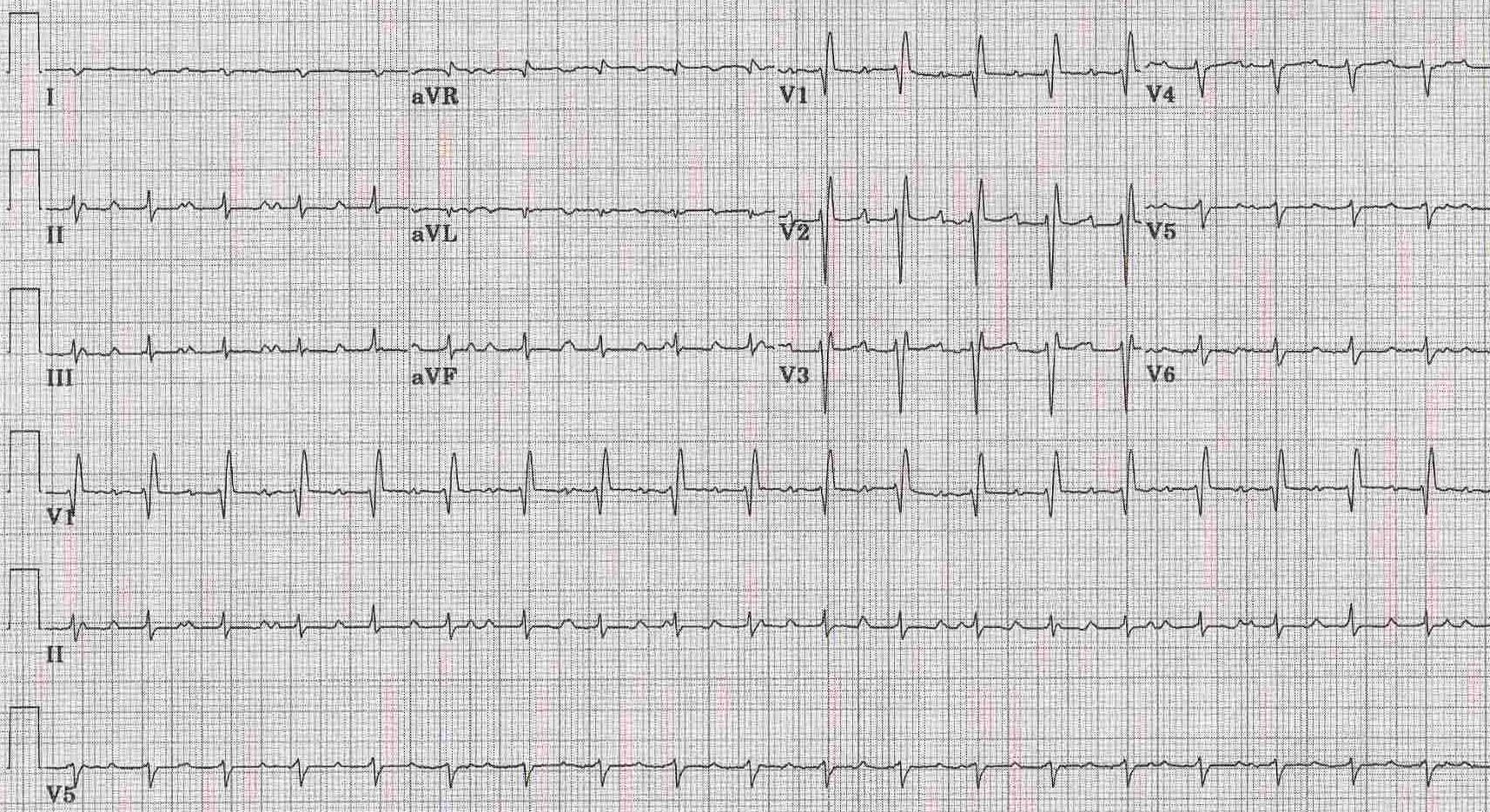 12 lead EKG shows accessory atrial activity (better seen in lead II at the end of the first complex in the middle between the second and third complex and after the third complex) due to some of the original sinus node still remains in addition to the donor sinus node after a cardiac transplant. Because of a suture line in the right atrium the ectopic atrial rhythm rarely conducts to the AV node. Right axis deviation and a rSR' which might suggest volume overload RVH also shown.
12 lead EKG shows accessory atrial activity (better seen in lead II at the end of the first complex in the middle between the second and third complex and after the third complex) due to some of the original sinus node still remains in addition to the donor sinus node after a cardiac transplant. Because of a suture line in the right atrium the ectopic atrial rhythm rarely conducts to the AV node. Right axis deviation and a rSR' which might suggest volume overload RVH also shown.
