Norepinephrine
| File:Norepinephrine structure with descriptor.svg | |

| |
| Names | |
|---|---|
| IUPAC name
4-[(1R)-2-amino-1-hydroxyethyl]benzene-1,2-diol
| |
| Other names
Noradrenaline
(R)-(–)-Norepinephrine | |
| Identifiers | |
3D model (JSmol)
|
|
| ChemSpider | |
| ECHA InfoCard | Lua error in Module:Wikidata at line 879: attempt to index field 'wikibase' (a nil value). Lua error in Module:Wikidata at line 879: attempt to index field 'wikibase' (a nil value). |
PubChem CID
|
|
| |
| |
| Properties | |
| C8H11NO3 | |
| Molar mass | 169.18 g/mol |
Except where otherwise noted, data are given for materials in their standard state (at 25 °C [77 °F], 100 kPa). | |
| Infobox references | |
|
WikiDoc Resources for Norepinephrine |
|
Articles |
|---|
|
Most recent articles on Norepinephrine Most cited articles on Norepinephrine |
|
Media |
|
Powerpoint slides on Norepinephrine |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Norepinephrine at Clinical Trials.gov Trial results on Norepinephrine Clinical Trials on Norepinephrine at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Norepinephrine NICE Guidance on Norepinephrine
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Norepinephrine Discussion groups on Norepinephrine Patient Handouts on Norepinephrine Directions to Hospitals Treating Norepinephrine Risk calculators and risk factors for Norepinephrine
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Norepinephrine |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Norepinephrine (INN) (abbreviated norepi or NE) or noradrenaline (BAN) (abbreviated NA or NAd) is a catecholamine with multiple roles including as a hormone and a neurotransmitter.[2]
As a stress hormone, norepinephrine affects parts of the brain where attention and responding actions are controlled. Along with epinephrine, norepinephrine also underlies the fight-or-flight response, directly increasing heart rate, triggering the release of glucose from energy stores, and increasing blood flow to skeletal muscle. Norepinephrine can also suppress neuroinflammation when released diffusely in the brain from the locus ceruleus.[3]
When norepinephrine acts as a drug it increases blood pressure by increasing vascular tone through α-adrenergic receptor activation. The resulting increase in vascular resistance triggers a compensatory reflex that overcomes its direct stimulatory effects on the heart, called the baroreceptor reflex, which results in a drop in heart rate called reflex bradycardia.
Norepinephrine is synthesized from dopamine by dopamine β-hydroxylase.[4] It is released from the adrenal medulla into the blood as a hormone, and is also a neurotransmitter in the central nervous system and sympathetic nervous system where it is released from noradrenergic neurons. The actions of norepinephrine are carried out via the binding to adrenergic receptors.
Chemistry
Norepinephrine is a catecholamine and a phenethylamine. The natural stereoisomer is L-(−)-(R)-norepinephrine. The term "norepinephrine" is derived from the chemical prefix nor-, which indicates that norepinephrine is the next lower homolog of epinephrine. The two structures differ only in that epinephrine has a methyl group attached to its nitrogen, while the methyl group is replaced by a hydrogen atom in norepinephrine. The prefix nor- is likely derived as an abbreviation of the word "normal", used to indicate a demethylated compound.[5][6][7]
Origins
Norepinephrine is released when a host of physiological changes are activated by a stressful event.
In the brain, this is caused in part by activation of an area of the brain stem called the locus ceruleus. This nucleus is the origin of most norepinephrine pathways in the brain. Noradrenergic neurons project bilaterally (send signals to both sides of the brain) from the locus ceruleus along distinct pathways to many locations, including the cerebral cortex, limbic system, and the spinal cord, forming a neurotransmitter system.
Norepinephrine is also released from postganglionic neurons of the sympathetic nervous system, to transmit the fight-or-flight response in each tissue respectively. The adrenal medulla can also be counted to such postganglionic nerve cells, although they release norepinephrine into the blood.
Norepinephrine system
The noradrenergic neurons in the brain form a neurotransmitter system, that, when activated, exerts effects on large areas of the brain. The effects are alertness and arousal, and influences on the reward system.
Anatomically, the noradrenergic neurons originate both in the locus coeruleus and the lateral tegmental field. The axons of the neurons in the locus coeruleus act on adrenergic receptors in:
On the other hand, axons of neurons of the lateral tegmental field act on adrenergic receptors in hypothalamus, for example.
This structure explains some of the clinical uses of norepinephrine, since a modification of the system affects large areas of the brain.
Mechanism
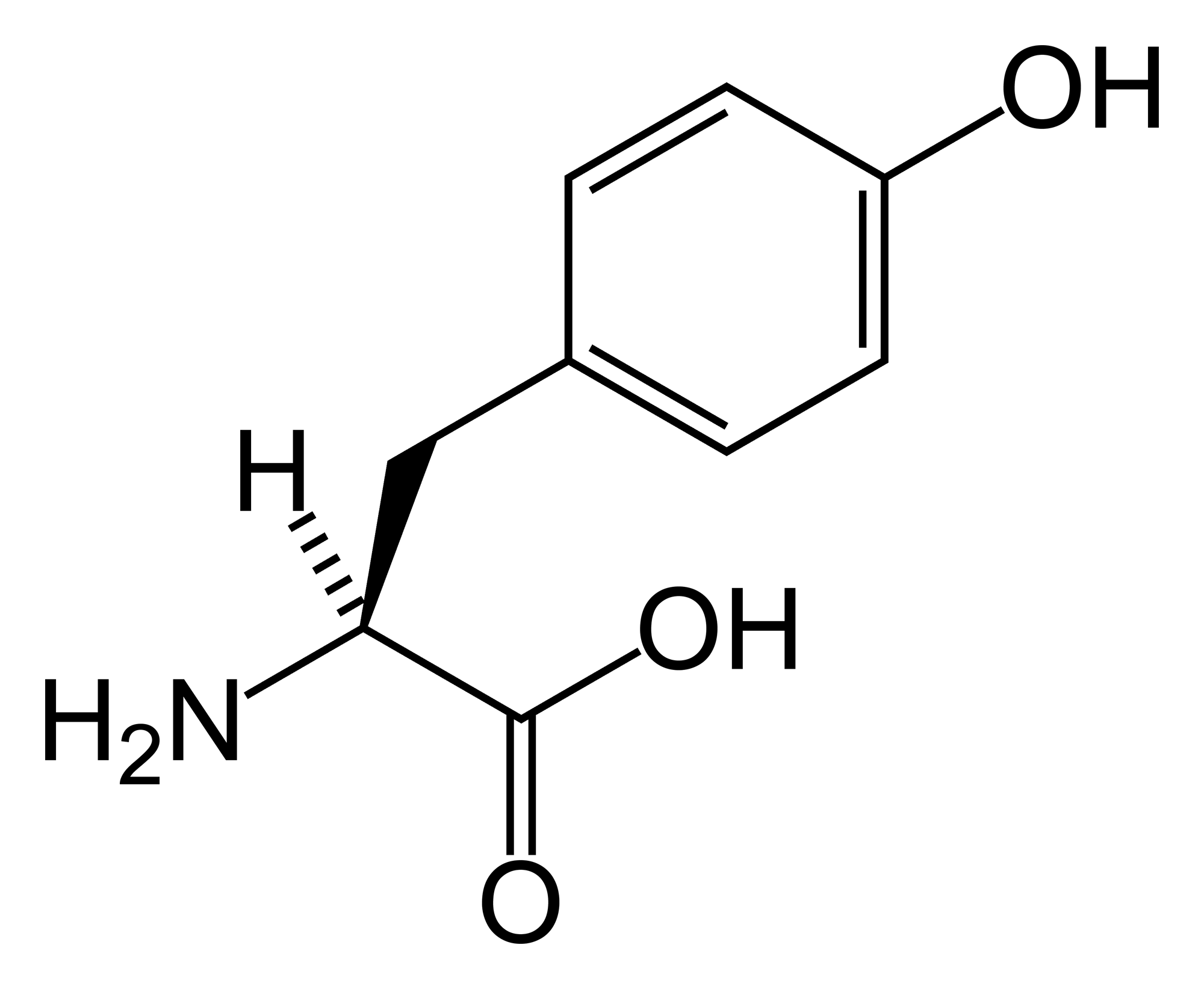
Norepinephrine is synthesized from tyrosine as a precursor, and packed into synaptic vesicles. It performs its action by being released into the synaptic cleft, where it acts on adrenergic receptors, followed by the signal termination, either by degradation of norepinephrine, or by uptake by surrounding cells.
Biosynthesis
Norepinephrine is synthesized by a series of enzymatic steps in the adrenal medulla and postganglionic neurons of the sympathetic nervous system from the amino acid tyrosine:
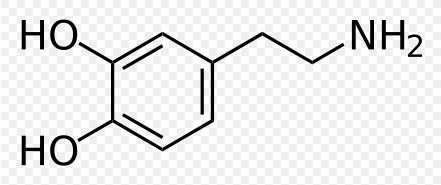
- The first reaction is the hydroxylation into dihydroxyphenylalanine (L-DOPA) (DOPA = 3,4-DiHydroxy-L-Phenylalanine), catalyzed by tyrosine hydroxylase. This is the rate-limiting step.
- This is followed by decarboxylation into the neurotransmitter dopamine, catalyzed by pyridoxal phosphate & DOPA decarboxylase.
- Last is the final β-oxidation into norepinephrine by dopamine beta hydroxylase, requiring ascorbate as a cofactor (electron donor).
-
-
-
Norepinephrine


{kind=link}
.svg){kind=link}
Vesicular transport
Between the decarboxylation and the final β-oxidation, norepinephrine is transported into synaptic vesicles. This is accomplished by vesicular monoamine transporter (VMAT) in the lipid bilayer. This transporter has equal affinity for norepinephrine, epinephrine and isoprenaline.[8]
Release
To perform its functions, norepinephrine needs to be released from synaptic vesicles. Many substances modulate this release, some inhibiting it and some stimulating it.
For instance, there are inhibitory α2 adrenergic receptors presynaptically, that gives negative feedback on release by homotropic modulation.
Receptor binding
Norepinephrine performs its actions on the target cell by binding to and activating adrenergic receptors. The target cell expression of different types of receptors determines the ultimate cellular effect, and thus norepinephrine has different actions on different cell types.
Termination
Signal termination is a result of reuptake and degradation.
Uptake
Extracellular uptake of norepinephrine into the cytosol is either done presynaptically (uptake 1) or by non-neuronal cells in the vicinity (uptake 2). Furthermore, there is a vesicular uptake mechanism from the cytosol into synaptic vesicles.
| Uptake | Transporter | Vmax (nmol/g/min)[9] | KM[9] | Specificity[10] | Location | Other substrates[10] | Inhibitors [11] |
|---|---|---|---|---|---|---|---|
| Uptake 1 | Norepinephrine transporter[11] | 1.2 | 0.3 | norepinephrine > epinephrine > isoprenaline | presynaptic | ||
| Uptake 2 | 100 | 250 | epinephrine > norepinephrine > isoprenaline | cell membrane of non-neuronal cells[8] | |||
| Vesicular | VMAT[11] | -[11] | ~0.2[11] | norepinephrine > epinephrine > isoprenaline[11] | Synaptic vesicle membrane[11] |
Degradation
{kind=link}
In mammals, norepinephrine is rapidly degraded to various metabolites. The principal metabolites are:
- Normetanephrine (via the enzyme catechol-O-methyl transferase, COMT)
- 3,4-Dihydroxymandelic acid (via monoamine oxidase, MAO)
- Vanillylmandelic acid (3-Methoxy-4-hydroxymandelic acid), also referred to as vanilmandelate or VMA (via MAO)
- 3-Methoxy-4-hydroxyphenylethylene glycol, "MHPG" or "MOPEG" (via MAO)
- Epinephrine (via PNMT)[13]
In the periphery, VMA is the major metabolite of catecholamines, and is excreted unconjugated in the urine. A minor metabolite (although the major one in the central nervous sytem) is MHPG, which is partly conjugated to sulfate or glucuronide derivatives and excreted in the urine.[14]
Noradrenergic agents
By indication
Norepinephrine may be used for the indications attention-deficit/hyperactivity disorder, depression and hypotension. Norepinephrine, as with other catecholamines, itself cannot cross the blood-brain barrier, so drugs such as amphetamines are necessary to increase brain levels.
Attention-deficit/hyperactivity disorder
Norepinephrine, along with dopamine, has come to be recognized as playing a large role in attention and focus. For people with ADHD, psychostimulant medications such as methylphenidate (Ritalin/Concerta), dextroamphetamine (Dexedrine), and Adderall (a mixture of dextroamphetamine and racemic amphetamine salts) are prescribed to help increase levels of norepinephrine and dopamine. Atomoxetine (Strattera) is a selective norepinephrine reuptake inhibitor, and is a unique ADHD medication, as it affects only norepinephrine, rather than dopamine. As a result, Strattera has a lower abuse potential. However, it may not be as effective as the psychostimulants are with many people who have ADHD. Consulting with a physician is needed to find the appropriate medication and dosage. (Other SNRIs, currently approved as antidepressants, have also been used off-label for treatment of ADHD.)
Depression
Differences in the norepinephrine system are implicated in depression. Serotonin-norepinephrine reuptake inhibitors are antidepressants that treat depression by increasing the amount of serotonin and norepinephrine available to postsynaptic cells in the brain. There is some recent evidence implying that SNRIs may also increase dopamine transmission.[15] This is because SNRIs work by inhibiting reuptake, i.e. preventing the serotonin and norepinephrine transporters from taking their respective neurotransmitters back to their storage vesicles for later use. If the norepinephrine transporter normally recycles some dopamine too, then SNRIs will also enhance dopaminergic transmission. Therefore, the antidepressant effects associated with increasing norepinephrine levels may also be partly or largely due to the concurrent increase in dopamine (particularly in the prefrontal cortex of the brain).
Tricyclic antidepressants (TCAs) increase norepinephrine activity as well. Most of them also increase serotonin activity, but tend to produce unwanted side effects due to the nonspecific inactivation of histamine, acetylcholine and alpha-1 adrenergic receptors. Common side effects include sedation, dry mouth, constipation, sinus tachycardia, memory impairment, orthostatic hypotension, blurred vision and weight gain.[16] For this reason, they have largely been replaced by newer selective reuptake drugs. These include the SSRIs, e.g. fluoxetine (Prozac), which however have little or no effect on norepinephrine, and the newer SNRIs described above, such as venlafaxine (Effexor) and duloxetine (Cymbalta).
Schizophrenia
A commonly-known side effect associated with schizo-affective patients known as akathisia (commonly mistaken for schizophrenic symptoms) was found to be associated with increased levels of norepinephrine.[17] Data supports the efficacy of novel antipsychotics which deal with agonism of the NMDA glutamate receptors,[18] associated with regulating uptake of norepinephrine,[19] which in turn affects the trafficking of glutamate.[20] This suggests that schizophrenia may in fact have a greater association with abnormal norepinephrine-reuptake kinetics and less with dopamine, which may actually be responsible for a large part of the mechanism of glutamate release.[20]
Hypotension
Norepinephrine is also used as a vasopressor medication (for example, brand name Levophed) for patients with critical hypotension. It is given intravenously and acts on both α1 and α2 adrenergic receptors to cause vasoconstriction. Its effects are often limited to the increasing of blood pressure through agonist activity on α1 and α2 receptors and causing a resultant increase in peripheral vascular resistance. At high doses, and especially when it is combined with other vasopressors, it can lead to limb ischemia and limb death. Norepinephrine is mainly used to treat patients in vasodilatory shock states such as septic shock and neurogenic shock and has shown a survival benefit over dopamine.
By site of action
Different medications affecting norepinephrine function have their targets at different points in the mechanism, from synthesis to signal termination.
Synthesis modulators
α-methyltyrosine is a substance that intervenes in norepinephrine synthesis by substituting tyrosine for tyrosine hydroxylase, and blocking this enzyme.
Vesicular transport modulators
This transportation can be inhibited by reserpine and tetrabenazine.[8]
Release modulators
| Substance[21] | Receptor[21] |
|---|---|
| acetylcholine | muscarinic receptor |
| norepinephrine (itself)/epinephrine | α2 receptor |
| 5-HT | 5-HT receptor |
| adenosine | P1 receptor |
| PGE | EP receptor |
| histamine | H2 receptor |
| enkephalin | δ receptor |
| dopamine | D2 receptor |
| ATP | P2 receptor |
| Substance[21] | Receptor[21] |
|---|---|
| adrenaline | β2 receptor |
| angiotensin II | AT1 receptor |
Receptor binding modulators
Examples include alpha blockers for the α-receptors, and beta blockers for the β-receptors.
Termination modulators
Uptake modulators
Inhibitors[8] of uptake 1 include:
Inhibitors[8] of uptake 2 include:
Anti-Inflammatory agent role in Alzheimer’s Disease
The norepinephrine from locus ceruleus cells in addition to its neurotransmitter role locally defuses from "varicosities". As such it provides an endogenous anti-inflammatory agent in the microenvironment around the neurons, glial cells, and blood vessels in the neocortex and hippocampus.[3] Up to 70% of norepinephrine projecting cells are lost in Alzheimer’s Disease. It has been shown that norepinephrine stimulates mouse microglia to suppress Aβ-induced production of cytokines and their phagocytosis of Aβ suggesting this loss might have a role in causing this disease.[3]
Nutritional sources
{kind=link}
The synthesis of norepinephrine depends on the presence of tyrosine, an amino acid found in proteins such as meat, nuts, and eggs. Dairy products such as cheese also contain high amounts of tyrosine (the amino acid is named for "tyros," the Greek word for cheese). Tyrosine is the precursor to dopamine, which is in itself a precursor of epinephrine and norepinephrine.
Serotonin, a neurotransmitter that is in many ways the opposite of the catecholamines, is also directly synthesized from an amino acid (tryptophan). However, tryptophan has a somewhat different process of degradation. When serotonin is catabolized in the body, it does not break down into useful substrates in the way that dopamine is further degraded into epinephrine and norepinephrine. Instead, it breaks down into 5-hydroxyindoleacetic acid (5-HIA), an organic acid which may be harmful in high amounts. Tryptophan can further be catabolized into kynurenate, quinolinate, and picolinate, harmful substances that are generally regarded as markers of bodily inflammation.
Banana peels contain significant amounts of norepinephrine and dopamine.[22]
See also
External links
- Mental Health: A report of surgeon general. Etiology of Anxiety Disorders
- http://www.biopsychiatry.com/nordop.htm
References
- ↑ Merck Index, 11th Edition, 6612.
- ↑ "Norepinephrine definition". dictionary.reference.com. Retrieved 2008-11-24. Text " Dictionary.com " ignored (help)
- ↑ 3.0 3.1 3.2 Heneka MT, Nadrigny F, Regen T, Martinez-Hernandez A, Dumitrescu-Ozimek L, Terwel D, Jardanhazi-Kurutz D, Walter J, Kirchhoff F, Hanisch UK, Kummer MP. (2010). Locus ceruleus controls Alzheimer's disease pathology by modulating microglial functions through norepinephrine. Proc Natl Acad Sci U S A. 107:6058–6063 doi:10.1073/pnas.0909586107 PMID 20231476
- ↑ "Introduction to Autonomic Pharmacology" (PDF). Elsevier International. Link redirected to commercial site!
- ↑ Sharma B, Satish A, Kumar R (1999). Dictionary of Drugs. Anmol Publications. ISBN 8126118202.
- ↑ Gaddum JH (1956). "The Prefix 'Nor' in Chemical Nomenclature". Nature. 177 (1046): 1046. doi:10.1038/1771046b0. Unknown parameter
|month=ignored (help) - ↑ Matthiessen A, Foster GC (1868). "Researches into the chemical constitution of narcotine and of its products of decomposition". Journal of the Chemical Society. 358.
- ↑ 8.0 8.1 8.2 8.3 8.4 Rang, H. P. (2003). Pharmacology. Edinburgh: Churchill Livingstone. ISBN 0-443-07145-4. Page 167
- ↑ 9.0 9.1 These values are from rat heart. Unless else specified in table, then ref is: Rang, H. P. (2003). Pharmacology. Edinburgh: Churchill Livingstone. ISBN 0-443-07145-4. Page 167
- ↑ 10.0 10.1 Unless else specified in table, then ref is: Rang, H. P. (2003). Pharmacology. Edinburgh: Churchill Livingstone. ISBN 0-443-07145-4. Page 167
- ↑ 11.00 11.01 11.02 11.03 11.04 11.05 11.06 11.07 11.08 11.09 11.10 11.11 Unless else specified in boxes, then ref is: Rod Flower; Humphrey P. Rang; Maureen M. Dale; Ritter, James M. (2007). Rang & Dale's pharmacology. Edinburgh: Churchill Livingstone. ISBN 0-443-06911-5.
- ↑ Figure 11-4 in: Rod Flower; Humphrey P. Rang; Maureen M. Dale; Ritter, James M. (2007). Rang & Dale's pharmacology. Edinburgh: Churchill Livingstone. ISBN 0-443-06911-5.
- ↑ "Endokrynologia Kliniczna" ISBN 83-200-0815-8, page 502
- ↑ Chapter 11 in: Rod Flower; Humphrey P. Rang; Maureen M. Dale; Ritter, James M. (2007). Rang & Dale's pharmacology. Edinburgh: Churchill Livingstone. ISBN 0-443-06911-5.
- ↑ http://stahlonline.cambridge.org/prescribers_drug.jsf?page=0521683505c95_p539-544.html.therapeutics&name=Venlafaxine&title=Therapeutics
- ↑ http://www.preskorn.com/columns/9803.html
- ↑ http://books.google.com/books?id=AQeQa5AtpXoC&pg=PA215&lpg=PA215&source=bl&ots=_AZBdDkZOg&sig=cyrLwQRUUijGlvTRNVpmKoLJmpc&hl=en&ei=C9HMTI3mJ5DSsAPbhNzzDg&sa=X&oi=book_result&ct=result&resnum=2&ved=0CBcQ6AEwAQ#v=onepage&q&f=false
- ↑ http://www.nature.com/npp/journal/v31/n4/abs/1300838a.html
- ↑ http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6WN4-4CCGGN1-9P&_user=10&_coverDate=11%2F30%2F1984&_rdoc=1&_fmt=high&_orig=search&_origin=search&_sort=d&_docanchor=&view=c&_searchStrId=1520587233&_rerunOrigin=scholar.google&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=5e43884bdf1f204eb2356e02096708bc&searchtype=a
- ↑ 20.0 20.1 http://sciencelinks.jp/j-east/article/200707/000020070707A0194475.php
- ↑ 21.0 21.1 21.2 21.3 Unless else specified in table, then ref is: Rang, H. P. (2003). Pharmacology. Edinburgh: Churchill Livingstone. ISBN 0-443-07145-4. Page 129
- ↑ Kanazawa, Kazuki (2000). "High content of Dopamine, a strong antioxidant, in Cavendish banana" (PDF). Journal of Agriculture and Food Chemistry. 48: 844–848. doi:10.1021/jf9909860. Retrieved 8 November 2007. Unknown parameter
|coauthors=ignored (help)
Template:Amino alcohols Template:Adrenergic and dopaminergic agents
- Pages with script errors
- Pages with broken file links
- Pages with citations using unnamed parameters
- CS1 maint: Multiple names: authors list
- Pages with citations using unsupported parameters
- Articles without EBI source
- Articles without KEGG source
- Articles without UNII source
- Chemical articles with unknown parameter in Chembox
- ECHA InfoCard ID from Wikidata
- Articles containing unverified chemical infoboxes
- Chembox image size set
- Catecholamines
- Neurotransmitters
- Cardiovascular Drugs
- Drug