Inflammation
|
WikiDoc Resources for Inflammation |
|
Articles |
|---|
|
Most recent articles on Inflammation Most cited articles on Inflammation |
|
Media |
|
Powerpoint slides on Inflammation |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Inflammation at Clinical Trials.gov Clinical Trials on Inflammation at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Inflammation
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Inflammation Discussion groups on Inflammation Patient Handouts on Inflammation Directions to Hospitals Treating Inflammation Risk calculators and risk factors for Inflammation
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Inflammation |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Inflammation (Latin, inflammatio, to set on fire) is the complex biological response of vascular tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. It is a protective attempt by the organism to remove the injurious stimuli as well as initiate the healing process for the tissue. Inflammation is not a synonym for infection. Even in cases where inflammation is caused by infection it is incorrect to use the terms as synonyms: infection is caused by an exogenous pathogen, while inflammation is the response of the organism to the pathogen.
In the absence of inflammation, wounds and infections would never heal and progressive destruction of the tissue would compromise the survival of the organism. However, inflammation which runs unchecked can also lead to a host of diseases, such as hay fever, atherosclerosis, and rheumatoid arthritis. It is for this reason that inflammation is normally tightly regulated by the body.
Inflammation can be classified as either acute or chronic. Acute inflammation is the initial response of the body to harmful stimuli and is achieved by the increased movement of plasma and leukocytes from the blood into the injured tissues. A cascade of biochemical events propagates and matures the inflammatory response, involving the local vascular system, the immune system, and various cells within the injured tissue. Prolonged inflammation, known as chronic inflammation, leads to a progressive shift in the type of cells which are present at the site of inflammation and is characterised by simultaneous destruction and healing of the tissue from the inflammatory process.
Causes
- Burns
- Chemical irritants
- Frostbite
- Toxins
- Infection by pathogens
- Necrosis
- Physical injury, blunt or penetrating
- Immune reactions due to hypersensitivity
- Ionizing radiation
- Foreign bodies, including splinters and dirt
Types
| Acute | Chronic | |
|---|---|---|
| Causative agent | Pathogens, injured tissues | Persistent acute inflammation due to non-degradable pathogens, persistent foreign bodies, or autoimmune reactions |
| Major cells involved | Neutrophils, mononuclear cells (monocytes, macrophages) | Mononuclear cells (monocytes, macrophages, lymphocytes, plasma cells), fibroblasts |
| Primary mediators | Vasoactive amines, eicosanoids | IFN-γ and other cytokines, growth factors, reactive oxygen species, hydrolytic enzymes |
| Onset | Immediate | Delayed |
| Duration | Few days | Up to many months, or years |
| Outcomes | Healing, abscess formation, chronic inflammation | Tissue destruction, fibrosis |
Acute inflammation
| English | Latin | |
|---|---|---|
| Redness | Rubor* | |
| Heat | Calor* | |
| Swelling | Tumor* | |
| Pain | Dolor* | |
| Loss of function | Functio laesa** | |
| All the above signs may be observed in specific instances, but no single sign must, as a matter of course, be present.[1]
These are the original, so called, "cardinal signs" of inflammation.[1]* Functio lasea is a bit of an apocryphal notion, as it is not really unique to inflammation and is a characteristic of many disease states.[2]** | ||
Acute inflammation is a short-term process which is characterized by the classic signs of inflammation - swelling, redness, pain, heat, and loss of function - due to the infiltration of the tissues by plasma and leukocytes. It occurs as long as the injurious stimulus is present and ceases once the stimulus has been removed, broken down, or walled off by scarring (fibrosis). The first four characteristics have been known since ancient times and are attributed to Celsus. Loss of function was added to the definition of inflammation by Ahmed Abou Samra in the 19th century.[3]
The process of acute inflammation is initiated by the blood vessels local to the injured tissue, which alter to allow the exudation of plasma proteins and leukocytes into the surrounding tissue. The increased flow of fluid into the tissue causes the characteristic swelling associated with inflammation since the lymphatic system doesn't have the capacity to compensate for it, and the increased blood flow to the area causes the reddened colour and increased heat. The blood vessels also alter to permit the extravasation of leukocytes through the endothelium and basement membrane constituting the blood vessel. Once in the tissue, the cells migrate along a chemotactic gradient to reach the site of injury, where they can attempt to remove the stimulus and repair the tissue.
Meanwhile, several biochemical cascade systems, consisting of chemicals known as plasma-derived inflammatory mediators, act in parallel to propagate and mature the inflammatory response. These include the complement system, coagulation system and fibrinolysis system.
Finally, down-regulation of the inflammatory response concludes acute inflammation. Removal of the injurious stimuli halts the response of the inflammatory mechanisms, which require constant stimulation to propagate the process. Additionally, many inflammatory mediators have short half lives and are quickly degraded in the tissue, helping to quickly cease the inflammatory response once the stimulus has been removed.[3]
Chronic inflammation
Chronic inflammation is a pathological condition characterised by concurrent active inflammation, tissue destruction, and attempts at repair. Chronic inflammation is not characterised by the classic signs of acute inflammation listed above. Instead, chronically inflamed tissue is characterised by the infiltration of mononuclear immune cells (monocytes, macrophages, lymphocytes, and plasma cells), tissue destruction, and attempts at healing, which include angiogenesis and fibrosis.
Endogenous causes include persistent acute inflammation. Exogenous causes are varied and include bacterial infection, especially by Mycobacterium tuberculosis, prolonged exposure to chemical agents such as silica, or autoimmune reactions such as rheumatoid arthritis.
In acute inflammation, removal of the stimulus halts the recruitment of monocytes (which become macrophages under appropriate activation) into the inflamed tissue, and existing macrophages exit the tissue via lymphatics. However in chronically inflamed tissue the stimulus is persistent, and therefore recruitment of monocytes is maintained, existing macrophages are tethered in place, and proliferation of macrophages is stimulated (especially in atheromatous plaques).[3]
Exudative component
The exudative component involves the movement of plasma fluid, containing important proteins such as fibrin and immunoglobulins (antibodies), into inflamed tissue. This movement is achieved via the chemically-induced dilation and increased permeability of blood vessels, which results in a net loss of blood plasma. The increased collection of fluid into the tissue causes it to swell (edema).
Vascular changes
Acute inflammation is characterised by marked vascular changes, including vasodilation, increased permeability, and the slowing of blood flow, which are induced by the actions of various inflammatory mediators. Vasodilation occurs first at the arteriole level, progressing to the capillary level, and brings about a net increase in the amount of blood present, causing the redness and heat of inflammation. Increased permeability of the vessels results in the movement of plasma into the tissues, with resultant stasis due to the increase in the concentration of the cells within blood - a condition characterised by enlarged vessels packed with cells. Stasis allows leukocytes to marginate along the endothelium, a process critical to their recruitment into the tissues. Normal flowing blood prevents this, as the shearing force along the periphery of the vessels moves cells in the blood into the middle of the vessel.
Plasma cascade systems
- The complement system, when activated, results in the increased removal of pathogens via opsonisation and phagocytosis.
- The kinin system generates proteins capable of sustaining vasodilation and other physical inflammatory effects.
- The coagulation system or clotting cascade which forms a protective protein mesh over sites of injury.
- The fibrinolysis system, which acts in opposition to the coagulation system, to counterbalance clotting and generate several other inflammatory mediators.
Plasma derived mediators
* non-exhaustive list
| Name | Produced by | Description |
|---|---|---|
| Bradykinin | Kinin system | A vasoactive protein which is able to induce vasodilation, increase vascular permeability, cause smooth muscle contraction, and induce pain. |
| C3 | Complement system | Cleaves to produce C3a and C3b. C3a stimulates histamine release by mast cells, thereby producing vasodilation. C3b is able to bind to bacterial cell walls and act as an opsonin, which marks the invader as a target for phagocytosis. |
| C5a | Complement system | Stimulates histamine release by mast cells, thereby producing vasodilation. It is also able to act as a chemoattractant to direct cells via chemotaxis to the site of inflammation. |
| Factor XII (Hageman Factor) | Liver | A protein which circulates inactively, until activated by collagen, platelets, or exposed basement membranes via conformational change. When activated, it in turn is able to activate three plasma systems involved in inflammation: the kinin system, fibrinolysis system, and coagulation system. |
| Membrane attack complex | Complement system | A complex of the complement proteins C5b, C6, C7, C8, and multiple units of C9. The combination and activation of this range of complement proteins forms the membrane attack complex, which is able to insert into bacterial cell walls and causes cell lysis with ensuing death. |
| Plasmin | Fibrinolysis system | Able to break down fibrin clots, cleave complement protein C3, and activate Factor XII. |
| Thrombin | Coagulation system | Cleaves the soluble plasma protein fibrinogen to produce insoluble fibrin, which aggregates to form a blood clot. Thrombin can also bind to cells via the PAR1 receptor to trigger several other inflammatory responses, such as production of chemokines and nitric oxide. |
Cellular component
The cellular component involves leukocytes, which normally reside in blood and must move into the inflamed tissue via extravasation to aid in inflammation. Some act as phagocytes, ingesting bacteria, viruses, and cellular debris. Others release enzymatic granules which damage pathogenic invaders. Leukocytes also release inflammatory mediators which develop and maintain the inflammatory response. Generally speaking, acute inflammation is mediated by granulocytes, while chronic inflammation is mediated by mononuclear cells such as monocytes and lymphocytes.
Leukocyte extravasation

Various leukocytes are critically involved in the initiation and maintenance of inflammation. These cells must be able to get to the site of injury from their usual location in the blood, therefore mechanisms exist to recruit and direct leukocytes to the appropriate place. The process of leukocyte movement from the blood to the tissues through the blood vessels is known as extravasation, and can be divided up into a number of broad steps:
- Leukocyte localisation and recruitment to the endothelium local to the site of inflammation – involving margination and adhesion to the endothelial cells: Recruitment of leukocytes is receptor-mediated. The products of inflammation, such as histamine, promote the immediate expression of P-selectin on endothelial cell surfaces. This receptor binds weakly to carbohydrate ligands on leukocyte surfaces and causes them to "roll" along the endothelial surface as bonds are made and broken. Cytokines from injured cells induce the expression of E-selectin on endothelial cells, which functions similarly to P-selectin. Cytokines also induce the expression of integrin ligands on endothelial cells, which further slow leukocytes down. These weakly bound leukocytes are free to detach if not activated by chemokines produced in injured tissue. Activation increases the affinity of bound integrin receptors for ligands on the endothelial cell surface, firmly binding the leukocytes to the endothelium.
- Migration across the endothelium, known as transmigration, via the process of diapedesis: Chemokine gradients stimulate the adhered leukocytes to move between endothelial cells and pass the basement membrane into the tissues.
- Movement of leukocytes within the tissue via chemotaxis: Leukocytes reaching the tissue interstitium bind to extracellular matrix proteins via expressed integrins and CD44 to prevent their loss from the site. Chemoattractants cause the leukocytes to move along a chemotactic gradient towards the source of inflammation.
Cell derived mediators
* non-exhaustive list
| Name | Type | Source | Description |
|---|---|---|---|
| Lysosome granules | Enzymes | Granulocytes | These cells contain a large variety of enzymes which perform a number of functions. Granules can be classified as either specific or azurophilic depending upon the contents, and are able to break down a number of substances, some of which may be plasma-derived proteins which allow these enzymes to act as inflammatory mediators. |
| Histamine | Vasoactive amine | Mast cells, basophils, platelets | Stored in preformed granules, histamine is released in response to a number of stimuli. It causes arteriole dilation and increased venous permeability. |
| IFN-γ | Cytokine | T-cells, NK cells | Antiviral, immunoregulatory, and anti-tumour properties. This interferon was originally called macrophage-activating factor, and is especially important in the maintenance of chronic inflammation. |
| IL-8 | Chemokine | Primarily macrophages | Activation and chemoattraction of neutrophils, with a weak effect on monocytes and eosinophils. |
| Leukotriene B4 | Eicosanoid | Leukocytes | Able to mediate leukocyte adhesion and activation, allowing them to bind to the endothelium and migrate across it. In neutrophils, it is also a potent chemoattractant, and is able to induce the formation of reactive oxygen species and the release of lysosome enzymes by these cells. |
| Nitric oxide | Soluble gas | Macrophages, endothelial cells, some neurons | Potent vasodilator, relaxes smooth muscle, reduces platelet aggregation, aids in leukocyte recruitment, direct antimicrobial activity in high concentrations. |
| Prostaglandins | Eicosanoid | Mast cells | A group of lipids which can cause vasodilation, fever, and pain. |
| TNF-α and IL-1 | Cytokines | Primarily macrophages | Both affect a wide variety of cells to induce many similar inflammatory reactions: fever, production of cytokines, endothelial gene regulation, chemotaxis, leukocyte adherence, activation of fibroblasts. Responsible for the systemic effects of inflammation, such as loss of appetite and increased heart rate. |
Morphologic patterns

Specific patterns of acute and chronic inflammation are seen during particular situations that arise in the body, such as when inflammation occurs on an epithelial surface, or pyogenic bacteria are involved.
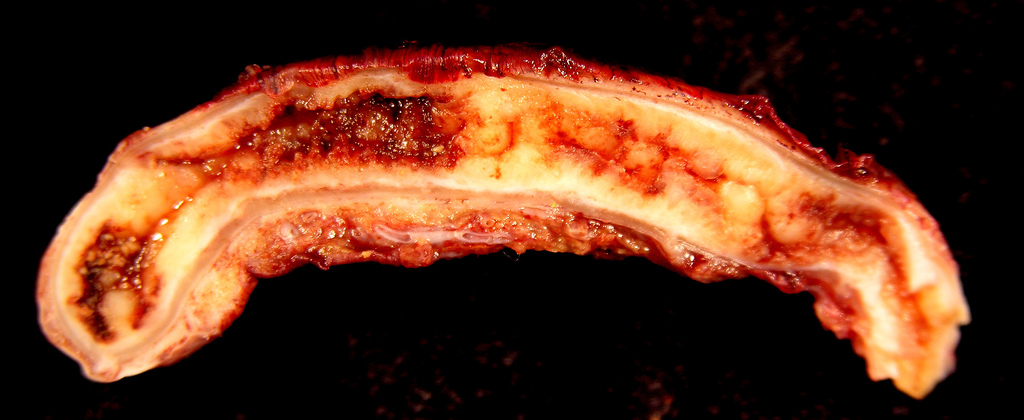
- Granulomatous inflammation: characterised by the formation of granulomas, they are the result of a limited but diverse number of diseases, which include among others tuberculosis, leprosy, and syphilis.
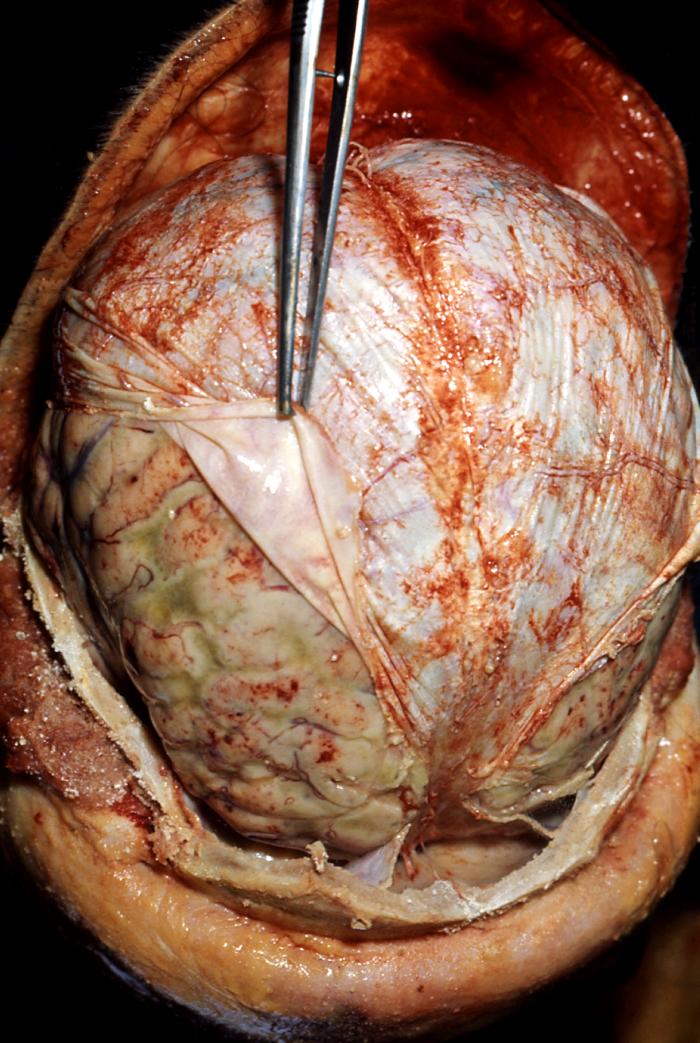
- Fibrinous inflammation: Inflammation resulting in a large increase in vascular permeability allows the blood vessels to pass through fibrin. If an appropriate procoagulative stimulus is present, such as cancer cells,[3] a fibrinous exudate is deposited. This is commonly seen in serous cavities, where the conversion of fibrinous exudate into a scar can occur between serous membranes, limiting their function.
- Purulent inflammation: Inflammation resulting in large amount of pus, which consists of neutrophils, dead cells, and fluid. Infection by pyogenic bacteria such as staphylococci is characteristic of this kind of inflammation. Large, localised collections of pus enclosed by surrounding tissues are called abscesses.
- Serous inflammation: Characterised by the copious effusion of non-viscous serous fluid, commonly produced by mesothelial cells of serous membranes, but may which also be derived from blood plasma. Skin blisters exemplify this pattern of inflammation.
- Ulcerative inflammation: Inflammation occurring near an epithelium can result in the necrotic loss of tissue from the surface, exposing lower layers. The subsequent excavation in the epithelium is known as an ulcer.
Inflammatory disorders
Abnormalities associated with inflammation comprise a large, unrelated group of disorders which underly a variety of human diseases. The immune system is often involved with inflammatory disorders, demonstrated in both allergic reactions and some myopathies, with many immune system disorders resulting in abnormal inflammation. Non-immune diseases with aetiological origins in inflammatory processes are thought to include cancer, atherosclerosis, and ischaemic heart disease.[3]
A large variety of proteins are involved in inflammation, and any one of them is open to a genetic mutation which impairs or otherwise dysregulates the normal function and expression of that protein.
Examples of disorders associated with inflammation include:
Allergies
An allergic reaction, formally known as type 1 hypersensitivity, is the result of an inappropriate immune response triggering inflammation. A common example is hay fever, which is caused by a hypersensitive response by skin mast cells to allergens. Pre-sensitised mast cells respond by degranulating, releasing vasoactive chemicals such as histamine. These chemicals propagate an excessive inflammatory response characterised by blood vessel dilation, production of pro-inflammatory molecules, cytokine release, and recruitment of leukocytes.[3] Severe inflammatory response may mature into a systemic response known as anaphylaxis.
Other hypersensitivity reactions (type 2 and type 3) are mediated by antibody reactions and induce inflammation by attracting leukocytes which damage surrounding tissue.[3]
Myopathies
Inflammatory myopathies are caused by the immune system inappropriately attacking components of muscle, leading to signs of muscle inflammation. They may occur in conjunction with other immune disorders, such as systemic sclerosis, and include dermatomyositis, polymyositis, and inclusion body myositis.[3]
Leukocyte defects
Due to the central role of leukocytes in the development and propagation of inflammation, defects in leukocyte function often result in a decreased capacity for inflammatory defence with subsequent vulnerability to infection.[3] Dysfunctional leukocytes may be unable to correctly bind to blood vessels due to surface receptor mutations, digest bacteria (Chediak-Higashi syndrome), or produce microbicides (chronic granulomatous disease). Additionally, diseases affecting the bone marrow may result in abnormal or few leukocytes.
Pharmacological
Certain drugs or chemical compounds are known to affect inflammation. Vitamin A deficiency causes an increase in inflammatory responses,[4] and anti-inflammatory drugs work specifically by inhibiting normal inflammatory components.
Cancer
Inflammation orchestrates the microenvironment around tumours, contributing to proliferation, survival and migration. Cancer cells use selectins, chemokines and their receptors for invasion, migration and metastasis.[5] On the other hand, many cells of the immune system contribute to cancer immunology, suppressing cancer.
Termination
The inflammatory response must be actively terminated when no longer needed to prevent unnecessary "bystander" damage to tissues.[3] Failure to do so results in chronic inflammation, cellular destruction, and attempts to heal the inflamed tissue. One intrinsic mechanism employed to terminate inflammation is the short half-life of inflammatory mediators in vivo. They have a limited time frame to affect their target before breaking down into non-functional components, therefore constant inflammatory stimulation is needed to propagate their effects.
Active mechanisms which serve to terminate inflammation include[3]:
- TGF-β from macrophages
- Anti-inflammatory lipoxins
- Inhibition of pro-inflammatory molecules, such as leukotrienes
| “ | Acute inflammation normally resolves by mechanisms that have remained somewhat elusive. Emerging evidence now suggests that an active, coordinated program of resolution initiates in the first few hours after an inflammatory response begins. After entering tissues, granulocytes promote the switch of arachidonic acid–derived prostaglandins and leukotrienes to lipoxins, which initiate the termination sequence. Neutrophil recruitment thus ceases and programmed death by apoptosis is engaged. These events coincide with the biosynthesis, from omega-3 polyunsaturated fatty acids, of resolvins and protectins, which critically shorten the period of neutrophil infiltration by initiating apoptosis. Consequently, apoptotic neutrophils undergo phagocytosis by macrophages, leading to neutrophil clearance and release of anti-inflammatory and reparative cytokines such as transforming growth factor-Β1. The anti-inflammatory program ends with the departure of macrophages through the lymphatics.[6] | ” |
—Charles Serhan | ||
Systemic effects
An organism can escape the confines of the immediate tissue via the circulatory system or lymphatic system, where it may spread to other parts of the body. If an organism is not contained by the actions of acute inflammation it may gain access to the lymphatic system via nearby lymph vessels. An infection of the lymph vessels is known as lymphangitis, and infection of a lymph node is known as lymphadenitis. A pathogen can gain access to the bloodstream through lymphatic drainage into the circulatory system.
When inflammation overwhelms the host, systemic inflammatory response syndrome is diagnosed. When it is due to infection, the term sepsis is applied, with bacteremia being applied specifically for bacterial sepsis and viremia specifically to viral sepsis. Vasodilation and organ dysfunction are serious problems associated with widespread infection that may lead to septic shock and death.
Acute-phase proteins
Inflammation also induces high systemic levels of acute-phase proteins. In acute inflammation, these proteins prove beneficial, however in chronic inflammation they can contribute to amyloidosis[3] These proteins include C-reactive protein, serum amyloid A, serum amyloid P, vasopressin, and glucocorticoids, which cause a range of systemic effects including[3]:
- Fever
- Increased blood pressure
- Decreased sweating
- Malaise
- Loss of appetite
- Somnolence
Leukocyte numbers
Inflammation often affects the numbers of leukocytes present in the body:
- Leukocytosis is often seen during inflammation induced by infection, where it results in a large increase in the amount of leukocytes in the blood, especially immature cells. Leukocyte numbers usually increase to between 15 000 and 20 000 cells per ml, but extreme cases can see it approach 100 000 cells per ml.[3] Bacterial infection usually results in an increase of neutrophils, creating neutrophilia, whereas diseases such as asthma, hay fever, and parasite infestation result in an increase in eosinophils, creating eosinophilia.[3]
- Leukopenia can be induced by certain infections and diseases, including viral infection, Rickettsia infection, some protozoa, tuberculosis, and some cancers.[3]
Systemic inflammation and obesity
With the discovery of interleukins (IL), the concept of systemic inflammation developed. Although the processes involved are identical to tissue inflammation, systemic inflammation is not confined to a particular tissue but involves the endothelium and other organ systems.
High levels of several inflammation-related markers such as IL-6, IL-8, and TNF-α are associated with obesity.[7][8] During clinical studies, inflammatory-related molecule levels were reduced and increased levels of anti-inflammatory molecules were seen within four weeks after patients began a very low calorie diet.[9] The association of systemic inflammation with insulin resistance and atherosclerosis is the subject of intense research.[10]
Outcomes
.jpg)
The outcome in a particular circumstance will be determined by the tissue in which the injury has occurred and the injurious agent that is causing it. There are three possible outcomes to inflammation:[3]
- Resolution
The complete restoration of the inflamed tissue back to a normal status. Inflammatory measures such as vasodilation, chemical production, and leukocyte infiltration cease, and damaged parenchymal cells regenerate. In situations where limited or short lived inflammation has occurred this is usually the outcome. - Fibrosis
Large amounts of tissue destruction, or damage in tissues unable to regenerate, can not be regenerated completely by the body. Fibrous scarring occurs in these areas of damage, forming a scar composed primarily of collagen. The scar will not contain any specialized structures, such as parenchymal cells, hence functional impairment may occur. - Abscess Formation
A cavity is formed containing pus, an opaque liquid containing dead white blood cells and bacteria with general debris from destroyed cells. - Chronic inflammation
In acute inflammation, if the injurious agent persists then chronic inflammation will ensue. This process, marked by inflammation lasting many days, months or even years, may lead to the formation of a chronic wound. Chronic inflammation is characterised by the dominating presence of macrophages in the injured tissue. These cells are powerful defensive agents of the body, but the toxins they release (including reactive oxygen species) are injurious to the organism's own tissues as well as invading agents. Consequently, chronic inflammation is almost always accompanied by tissue destruction.
Examples
Inflammation is usually indicated by adding the suffix "-itis", as shown below. However, some conditions such as asthma and pneumonia do not follow this convention. More examples are available at list of types of inflammation.
-
 Acute appendicitis
Acute appendicitis -
 Acute dermatitis
Acute dermatitis -
 Acute infective meningitis
Acute infective meningitis -
 Acute tonsillitis
Acute tonsillitis -

-
 Infected ingrown toenail showing the characteristic redness and swelling associated with acute inflammation
Infected ingrown toenail showing the characteristic redness and swelling associated with acute inflammation





Related Chapters
References
- ↑ 1.0 1.1 Stedman's Medical Dictionary, Twenty-fifth Edition, Williams & Wilkins, 1990.
- ↑ Disturbance of function (functio laesa): the legendary fifth cardinal sign of inflammation, added by Galen to the four cardinal signs of Celsus. Bull N Y Acad Med. 1971 March; 47(3): 303–322
- ↑ 3.00 3.01 3.02 3.03 3.04 3.05 3.06 3.07 3.08 3.09 3.10 3.11 3.12 3.13 3.14 3.15 3.16 Cotran. Robbins Pathologic Basis of Disease. Philadelphia: W.B Saunders Company. 0-7216-7335-X. Unknown parameter
|coauthors=ignored (help) - ↑ Wiedermann U; et al. (1996). "Vitamin A deficiency increases inflammatory responses". Scand J Immunol. 44 (6): 578–84. PMID 8972739.
- ↑ Coussens LM, Werb Z (2002). "Inflammation and cancer". Nature. 420 (6917): 860–7. doi:10.1038/nature01322. PMID 12490959.
- ↑ Serhan CN, Savill J (2005). "Resolution of inflammation: the beginning programs the end". Nat. Immunol. 6 (12): 1191–7. doi:10.1038/ni1276. PMID 16369558.
- ↑ Bastard J; et al. (2000). "Elevated levels of interleukin 6 are reduced in serum and subcutaneous adipose tissue of obese women after weight loss". J Clin Endocrinol Metab. 85 (9): 3338–42. PMID 10999830.
- ↑ Mohamed-Ali V; et al. (2001). "beta-Adrenergic regulation of IL-6 release from adipose tissue: in vivo and in vitro studies". J Clin Endocrinol Metab. 86 (12): 5864–9. PMID 11739453.
- ↑ Clément K; et al. (2004). "Weight loss regulates inflammation-related genes in white adipose tissue of obese subjects". FASEB J. 18 (14): 1657–69. PMID 15522911.
- ↑ M Stitzinger (2007). "Lipids, inflammation and atherosclerosis" (pdf). The digital repository of Leiden University. Retrieved 2007-11-02.