Breast
Template:Infobox Anatomy Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
The term breast refers to the upper ventral region of an animal’s torso, particularly that of mammals, including human beings. The breasts of a female primate’s body contain the mammary glands, which secrete milk used to feed infants. This article deals with the human breast; for other animals, see udder and mammary gland.
Breasts are more visible on adult women, but male humans also have breasts which, although usually less prominent, are structurally identical (homologous) to the female, as they develop embryologically from the same tissues.
Anatomy

The breasts are modified sudoriferous (sweat) glands, producing milk in females, and in some rare cases, males.[1] Each breast has one nipple surrounded by the areola. The areola is colored from pink to dark brown and has several sebaceous glands. In females, the larger mammary glands within the breast produce the milk. They are distributed throughout the breast, with two-thirds of the tissue found within 30 mm of the base of the nipple.[2] These are drained to the nipple by between 4 and 18 lactiferous ducts, where each duct has its own opening. The network formed by these ducts is complex, like the tangled roots of a tree. It is not always arranged radially, and branches close to the nipple. The ducts near the nipple do not act as milk reservoirs; Ramsay et al. have shown that conventionally described lactiferous sinuses do not, in fact, exist.
The remainder of the breast is composed of connective tissue (collagen and elastin), adipose tissue (fat), and Cooper's ligaments. The ratio of glands to adipose tissues rises from 1:1 in nonlactating women to 2:1 in lactating women.[2]
The breasts sit over the pectoralis major muscle and usually extend from the level of the 2nd rib to the level of the 6th rib anteriorly. The superior lateral quadrant of the breast extends diagonally upwards towards the axillae and is known as the tail of Spence. A thin layer of mammary tissue extends from the clavicle above to the seventh or eighth ribs below and from the midline to the edge of the latissimus dorsi posteriorly. (For further explanation, see anatomical terms of location.)
The arterial blood supply to the breasts is derived from the internal thoracic artery (formerly called the internal mammary artery), lateral thoracic artery, thoracoacromial artery, and posterior intercostal arteries. The venous drainage of the breast is mainly to the axillary vein, but there is some drainage to the internal thoracic vein and the intercostal veins. Both sexes have a large concentration of blood vessels and nerves in their nipples. The nipples of both females and males can become erect in response to sexual stimuli,[3] and also to cold.
The breast is innervated by the anterior and lateral cutaneous branches of the fourth through sixth intercostal nerves. The nipple is supplied by the T4 dermatome.
Lymphatic drainage
About 75% of lymph from the breast travels to the ipsilateral axillary lymph nodes. The rest travels to parasternal nodes, to the other breast, or abdominal lymph nodes. The axillary nodes include the pectoral, subscapular, and humeral groups of lymph nodes. These drain to the central axillary lymph nodes, then to the apical axillary lymph nodes. The lymphatic drainage of the breasts is particularly relevant to oncology, since breast cancer is a common cancer and cancer cells can break away from a tumour and spread to other parts of the body through the lymph system by metastasis.
Shape and support
Breasts vary in both size and shape, and their external appearance is not predictive of their internal anatomy or lactation potential. The shape of a woman’s breasts is in large part dependent on their support, which primarily comes from the Cooper's ligaments, and the underlying chest on which they rest. The breast is attached at its base to the chest wall by the deep fascia over the pectoral muscles. On its upper surface it is given some support by the covering skin where it continues on to the upper chest wall. It is this support which determines the shape of the breasts. In a small fraction of women, the frontal milk sinuses (ampulla) in the breasts are not flush with the surrounding breast tissue, which causes the sinus area to visibly bulge outward.

In discussing the support of breasts, it is helpful to draw a distinction between breasts which rest on the chest below, and those which do not. High, rounded breasts protrude almost horizontally from the chest wall. All breasts are like this in early stages of development, and such a shape is common in younger women and girls. This protruding or “high” breast is anchored to the chest at its base, and the weight is distributed evenly over the area of the base of the approximately dome- or cone-shaped breasts.
In the “low” breast, a proportion of the breasts’ weight is actually supported by the chest against which the lower breast surface comes to rest, as well as the deep anchorage at the base. The weight is thus distributed over a larger area, which has the effect of reducing the strain. In both males and females, the thoracic cavity slopes progressively outwards from the thoracic inlet (at the top of the breastbone) above to the lowest ribs which mark its lower boundary, allowing it to support the breasts.
The inframammary fold (or line, or crease) is an anatomic structure created by adherence between elements in the skin and underlying connective tissue[4] and represents the inferior extent of breast anatomy. Some teenagers may develop breasts whose skin comes into contact with the chest below the fold at an early age, and some women may never develop such breasts; both situations are perfectly normal. The relationship of the nipple position to the fold is described as ptosis, a term also applied to other body parts and which refers in general to drooping or sagging. Due to breast weight and relaxation of support structures, the nipple-areola complex and breast tissue may eventually hang below the fold, and in some cases the breasts may extend as far as, or even beyond, the navel. The length from the nipple to the sternal notch (central, upper border) in the youthful breast averages 21 cm and is a common anthropometric figure used to assess both breast symmetry and ptosis. Lengthening of both this measurement and the distance between the nipple and the fold are both characteristic of advancing grades of ptosis.
The end of the breast, which includes the nipple, may either be flat (a 180 degree angle) or angled (angles lower than 180 degrees). Breast ends are rarely angled sharper than 60 degrees. Angling of the end of the breast is caused in part by the ligaments that suspend it, such that the breast ends often have a more obtuse angle when a woman is lying on her back. Breasts exist in a range of ratios between length and base diameter, usually ranging from ½ to 1.
Development
The development of a girl's breasts during puberty is triggered by sex hormones, chiefly estrogen. This hormone has been demonstrated to cause the development of woman-like, enlarged breasts in men, a condition called gynecomastia, and is sometimes used deliberately for this effect in transwomen who receive hormone replacement therapy.
In most cases, the breasts fold down over the chest wall during Tanner stage development, as shown in this diagram.[5] It is typical for a woman’s breasts to be unequal in size particularly while the breasts are developing. Statistically it is slightly more common for the left breast to be the larger.[6] In rare cases, the breasts may be significantly different in size, or one breast may fail to develop entirely.
A large number of medical conditions are known to cause abnormal development of the breasts during puberty. Virginal breast hypertrophy is a condition which involves excessive growth of the breasts, and in some cases the continued growth beyond the usual pubescent age. Breast hypoplasia is a condition where one or both breasts fail to develop.
In Cameroon, some girls are subjected to breast ironing to stunt breast growth in order to make them less sexually attractive in the belief that this makes them less likely to become a victim of rape.
Changes

As breasts are mostly composed of adipose tissue, their size can change over time. This occurs for a number of reasons, most obviously when a girl grows during puberty and when a woman becomes pregnant. The breast size may also change if she gains (or loses) weight for any other reason. Any rapid increase in size of the breasts can result in the appearance of stretchmarks.
It is typical for a number of other changes to occur during pregnancy: in addition to becoming larger, the breasts generally become firmer, mainly due to hypertrophy of the mammary gland in response to the hormone prolactin. The size of the nipples may increase noticeably and their pigmentation may become darker. These changes may continue during breastfeeding. The breasts generally revert to approximately their previous size after pregnancy, although there may be some increased sagging and stretchmarks.
The size of a woman’s breasts usually fluctuates during the menstrual cycle, particularly with premenstrual water retention. An increase in breast size is a common side effect of use of the combined oral contraceptive pill.
The breasts naturally sag through aging, as the ligaments become elongated.
Function
Breastfeeding

The primary function of mammary glands is to nurture young by producing breast milk. The production of milk is called lactation. (While the mammary glands that produce milk are present in the male, they normally remain undeveloped.) The orb-like shape of breasts may help limit heat loss, as a fairly high temperature is required for the production of milk. Alternatively, one theory states that the shape of the human breast evolved in order to prevent infants from suffocating while feeding.[7] Since human infants do not have a protruding jaw like human evolutionary ancestors and other primates, the infant’s nose might be blocked by a flat female chest while feeding.[7] According to this theory, as the human jaw receded, the breasts became larger to compensate.[7]
Milk production unrelated to pregnancy can also occur. This galactorrhea may be an adverse effect of some medicinal drugs (such as some antipsychotic medication), extreme physical stress or endocrine disorders. If it occurs in men it is called male lactation. Newborn babies are often capable of lactation because they receive the hormones prolactin and oxytocin via the mother's bloodstream, filtered through the placenta. This neonatal liquid is known colloquially as witch's milk.
Sexual role
Breasts play an important part in human sexual behavior. They are one of most visible or obvious female secondary sex characteristics,[8] and play an important role in sexual attraction of partners, and pleasure of the individual. On sexual arousal breast size increases, venous patterns across the breasts become more visible, and nipples harden. Breasts are sensitive to touch as they have many nerve endings, and it is common practice to press or massage breasts with hands during sexual intercourse. [9] Oral stimulation of nipples and breasts is also common. Some women can achieve breast orgasms. In the ancient Indian work the Kama Sutra, marking breasts with nails and biting with teeth are explained as erotic.[10]
Other suggested functions
Zoologists point out that no female mammal other than the human has breasts of comparable size, relative to the rest of the body, when not lactating and that humans are the only primate that has permanently swollen breasts. This suggests that the external form of the breasts is connected to factors other than lactation alone.
One theory is based around the fact that, unlike nearly all other primates, human females do not display clear, physical signs of ovulation. This could have plausibly resulted in human males evolving to respond to more subtle signs of ovulation. During ovulation, the increased estrogen present in the female body results in a slight swelling of the breasts, which then males could have evolved to find attractive. In response, there would be evolutionary pressures that would favor females with more swollen breasts who would, in a manner of speaking, appear to males to be the most likely to be ovulating.
Some zoologists (notably Desmond Morris) believe that the shape of female breasts evolved as a frontal counterpart to that of the buttocks, the reason being that whilst other primates mate in the rear-entry position, humans, because of their upright posture, are more likely to successfully copulate by mating face to face, the so-called missionary position. A secondary sexual characteristic on a woman’s chest would have encouraged this in more primitive incarnations of the human race, and a face on encounter may have helped found a relationship between partners beyond merely a sexual one.[11]
Cultural status
In art, religion, and legend

Historically, breasts have been regarded as fertility symbols, because they are the source of life-giving milk. Certain prehistoric female statuettes—so-called Venus figurines—often emphasised the breasts, as in the example of the Venus of Willendorf. In historic times, goddesses such as Ishtar were shown with many breasts, alluding to their role as protectors of childbirth and mothering. The legendary tribe of Amazons bared their breasts, and in some accounts removed one breast to allow better combat and archery.
Some religions afford the breast a special status, either in formal teachings or in symbolism. Islam forbids public exposure of the female breasts.[12] In Christian iconography, some works of art depict women with their breasts in their hands or on a platter, signifying that they died as a martyr by having their breasts severed; one example of this is Saint Agatha of Sicily. In Silappatikaram, Kannagi tears off her left breast and flings it on Madurai, cursing it, causing a devastating fire.
In practice
Breasts are secondary sex characteristics and sexually sensitive. Bare female breasts can elicit heightened sexual desires from men and women. Cultures that associate the breast primarily with sex (as opposed to with breastfeeding) tend to designate bare breasts as indecent, and they are not commonly displayed in public, in contrast to male chests. Other cultures view female toplessness as acceptable, and in some countries women have never been forbidden to bare their chests; in some African cultures, for example, the thigh is highly sexualised and never exposed in public, but the breast is not taboo. Opinion on the exposure of breasts often depends on the place and context, and in some Western societies exposure of breasts on a beach may be acceptable, although in town centres, for example, it is usually considered indecent. In some areas the prohibition against the display of a woman’s breasts only restricts exposure of the nipples.

Women in some areas and cultures are approaching the issue of breast exposure as one of sexual equality, since men (and pre-pubescent children) may bare their chests, but women and teenage girls are forbidden. In the United States, the topfree equality movement seeks to redress this imbalance. This movement won a decision in 1992 in the New York State Court of Appeals—“People v. Santorelli”, where the court ruled that the state’s indecent exposure laws do not ban women from being barebreasted. A similar movement succeeded in most parts of Canada in the 1990s. In Australia and much of Europe it is acceptable for women and teenage girls to sunbathe topless on some public beaches and swimming pools, but these are generally the only public areas where exposing breasts is acceptable.
When breastfeeding a baby in public, legal and social rules regarding indecent exposure and dress codes, as well as inhibitions of the woman, tend to be relaxed. Numerous laws around the world have made public breastfeeding legal and disallow companies from prohibiting it in the workplace. Yet the public reaction at the sight of breastfeeding can make the situation uncomfortable for those involved.
See also modesty, nudism and exhibitionism.
Clothing
Since the breasts are flexible, their shape may be affected by clothing, and foundation garments in particular. A brassiere (bra) may be worn to give additional support and to alter the shape of the breasts. There is some debate over whether such support is desirable. A long term clinical study showed that women with large breasts can suffer shoulder pain as a result of bra straps,[13] although a well fitting bra should support most of the breasts’ weight with proper sized cups and back band rather than on the shoulders.
Plastic surgery

Plastic surgical procedures of the breast include those for both cosmetic and reconstructive surgery indications. Some women choose these procedures as a result of the high value placed on symmetry of the human form, and because they identify their femininity and sense of self with their breasts.
After mastectomy (the surgical removal of a breast, usually to treat breast cancer) some women undergo breast reconstruction, either with breast implants or autologous tissue transfer, using fat and tissues from the abdomen (TRAM flap) or back (latissiumus muscle flap).
Breast reduction surgery is a common procedure which involves removing excess breast tissue, fat, and skin with repositioning of the nipple-areolar complex (NAC). Cosmetic procedures include breast lifts (mastopexy), breast augmentation with implants, and procedures that combine both elements. Implants containing either silicone gel or saline are available for augmentation and reconstructive surgeries. Surgery can repair inverted nipples by releasing ductal tissues which are tethering. Breast lift with or without reduction can be part of upper body lift after massive weight loss body contouring.
Any surgery of the breast carries with it the potential for interfering with future breastfeeding,[14][15][16] causing alterations in nipple sensation, and difficulty in interpreting mammography (xrays of the breast). A number of studies have demonstrated a similar ability to breastfeed when breast reduction patients are compared to control groups where the surgery was performed using a modern pedicle surgical technique.[17][18][19][20] Plastic surgery organizations have generally discouraged elective cosmetic breast augmentation surgery for teenage girls as the volume of their breast tissue may continue to grow significantly as they mature and because of concerns about understanding long-term risks and benefits of the procedure. Breast surgery in teens for reduction of significantly enlarged breasts or surgery to correct hypoplasia and severe asymmetry is considered on a case by case basis by most surgeons.
Health
Pre-malignant and malignant diseases

- Carcinoma in situ, a pre-malignant condition which can progress to a malignant cancer
Malignant diseases include:
- Breast cancer
- Paget’s disease of the nipple, also known as Paget’s disease of the breast
Among women worldwide, breast cancer is the most common cause of cancer death.[21] Breast self-examination (BSE) is an easy but unreliable method for finding possible breast cancer,[22] which is recommended once every month.
Infections and inflammations
These may be caused among others by trauma, secretory stasis/milk engorgement, hormonal stimulation, infections or autoimmune reactions. Repeated occurrence unrelated to lactation requires endocrinological examination.

- Mastitis
- bacterial mastitis
- mastitis from milk engorgement or secretory stasis
- mastitis of mumps
- chronic intramammary abscess
- chronic subareolar abscess
- tuberculosis of the breast
- syphilis of the breast
- retromammary abscess
- actinomycosis of the breast
- Mondor’s disease
- Duct ectasia syndrome
- Breast engorgement
Benign conditions
Benign conditions include:
- Congenital disorders
- Inverted nipple
- Supernumerary nipples/supernumerary breasts (polymazia / polymastia) /duplicated nipples
- Aberrations of normal development and involution
- Cyclical nodularity
- Breast cysts
- Fibroadenoma - benign tumor
- Gynecomastia (males)
- Nipple discharge, galactorrhea
- Mammary fistula
- Fibrocystic disease / Fibrocystic changes
- Cysts
- Epithelial hyperplasia
- Epithelial metaplasia
- Papillomas
- Adenosis
- Pregnancy-related
Documentary film
- Breasts, directed by Meema Spadola, 1996.
Breast: Foreign body reaction
{{#ev:youtube|mB2I2inv7Ts}}
Breast: Epithelial hyperplasia
{{#ev:youtube|0PADE4K1XWc}}
See also
- Brassiere
- Breast bondage
- Breast fetishism
- Breast self-examination
- Cleavage (breasts)
- Intimate part
- Mammary intercourse
- Milk line
- Teat
References
- ↑ Introduction to the Human Body, fifth ed. John Wiley & Sons, Inc.: New York, 2001. 560.
- ↑ 2.0 2.1 Anatomy of the lactating human breast redefined with ultrasound imaging, D.T. Ramsay et al., J. Anat. 206:525-34.
- ↑ "www.mckinley.uiuc.edu/Handouts/female_function_dysfunction.html".
- ↑ Boutros S, Kattash M, Wienfeld A, Yuksel E, Baer S, Shenaq S. The intradermal anatomy of the inframammary fold. Plast Reconstr Surg. 1998 Sep; 102(4):1030-3. PMID
- ↑ A.R. Greenbaum, T. Heslop, J. Morris and K.W. Dunn, An investigation of the suitability of bra fit in women referred for reduction mammaplasty, Br J Plast Surg 56 (2003) (3), pp. 230–236
- ↑ C.W. Loughry; et al. (1989). "Breast volume measurement of 598 women using biostereometric analysis". Annals of Plastic Surgery. 22 (5): 380 &ndash, 385.
- ↑ 7.0 7.1 7.2 Bentley, Gillian R. (2001). "The Evolution of the Human Breast". American Journal of Physical Anthropology. 32 (38).
- ↑ secondary sex characteristics
- ↑ "The entire breast is a network of nerve endings" link
- ↑ Sir Richard Burton's English translation of Kama Sutra
- ↑ Morris, Desmond (1967). The Naked Ape: a zoologist's study of the human animal. Canada: Bantam Books. pp. 64–68. N3924.
- ↑ “They shall cover their chests” or “they should draw their khimar (veils) over their bosoms”, depending on the translation, Quran (24:31). Available online
- ↑ Ryan, EL, Pectoral girdle myalgia in women: a five-year study in a clinical setting. Clin J Pain. 2000 Dec; 16(4):298-303.
- ↑ Neifert, M (1990). "The influence of breast surgery, breast appearance and pregnancy-induced changes on lactation sufficiency as measured by infant weight gain". Birth. 17 (1): 31–38. PMID 2288566. Unknown parameter
|coauthors=ignored (help);|access-date=requires|url=(help) - ↑ "FAQ on Previous Breast Surgery and Breastfeeding". La Leche League International. 2006-08-29. Retrieved 2007-02-11.
- ↑ West, Diana. "Breastfeeding After Breast Surgery". Australian Breastfeeding Association. Retrieved 2007-02-11.
- ↑ Cruz-Korchin, N (2004-09-15). "Breast-feeding after vertical mammaplasty with medial pedicle". Plast Reconstr Surg. 15 (114): 890–94. PMID 15468394. Unknown parameter
|coauthors=ignored (help);|access-date=requires|url=(help) - ↑ Brzozowski, D (February 2000). "Breast-feeding after inferior pedicle reduction mammaplasty". Plast Reconstr Surg. 105 (2): 530–34. PMID 10697157. Unknown parameter
|coauthors=ignored (help);|access-date=requires|url=(help) - ↑ Witte, PM (2004-06-26). "Successful breastfeeding after reduction mammaplasty". Ned Tijdschr Geneeskd. 148 (26): 1291–93. PMID 15279213. Unknown parameter
|coauthors=ignored (help);|access-date=requires|url=(help) - ↑ Kakagia, D (2005-10). "Breastfeeding after reduction mammaplasty: a comparison of 3 techniques". Ann Plast Surg. 55 (4): 343–45. PMID 16186694. Unknown parameter
|coauthors=ignored (help); Check date values in:|date=(help);|access-date=requires|url=(help) - ↑ World Health Organization (2006). "Fact sheet No. 297: Cancer". Retrieved 2007-04-26. Unknown parameter
|month=ignored (help) - ↑ Breast Self Examination at The Breast Site
Gallery
-
 Front view of woman's breasts
Front view of woman's breasts -
 Side view of a woman's breasts
Side view of a woman's breasts -
 Normal variation in shape
Normal variation in shape -
 International breastfeeding symbol
International breastfeeding symbol -
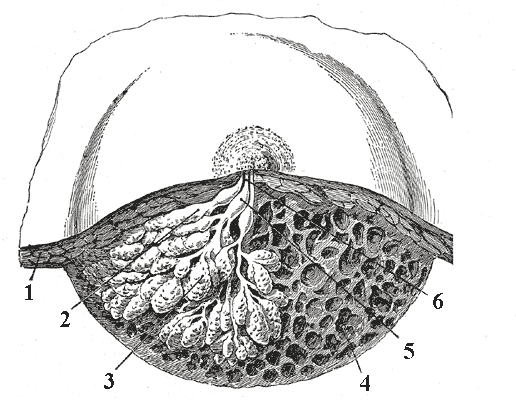 Diagram of dissected lactating breast
Diagram of dissected lactating breast -
 Illustration of saggital section of a human breast
Illustration of saggital section of a human breast -
 Breast with inverted nipple
Breast with inverted nipple -
 Illustration of the early warning signs of breast cancer
Illustration of the early warning signs of breast cancer -
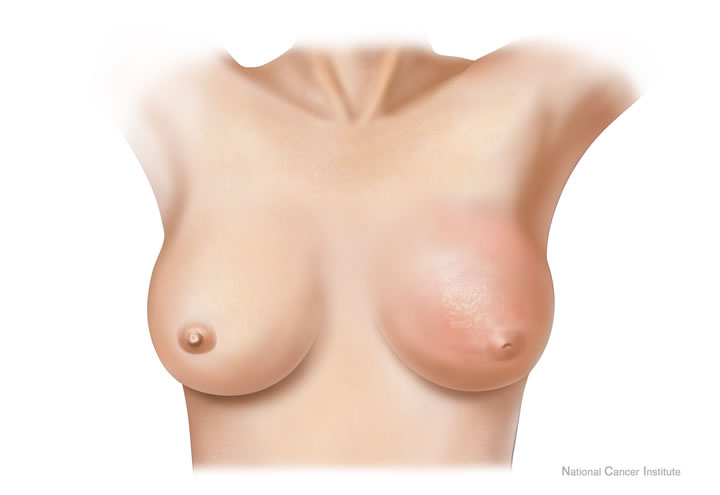 Drawing of inflammatory breast cancer
Drawing of inflammatory breast cancer -
 Patient with advanced local-regional recurrence of breast cancer with an ulcerating axillary mass
Patient with advanced local-regional recurrence of breast cancer with an ulcerating axillary mass -
 Breast self exam
Breast self exam -
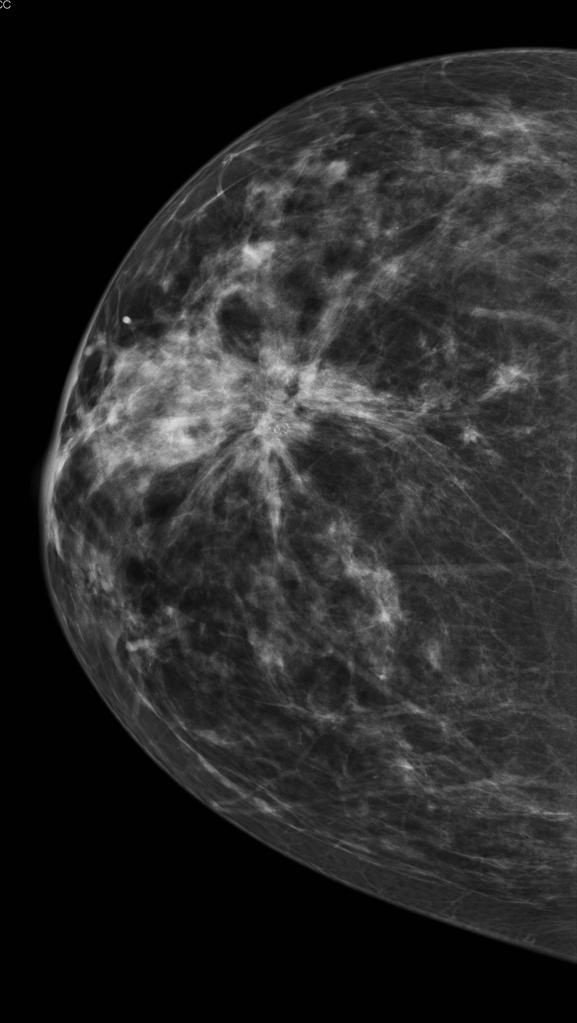 Woman undergoing mammogram
Woman undergoing mammogram -
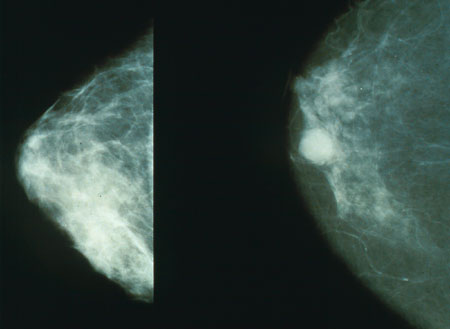 Mammography pictures, normal (left) and cancerous (right)
Mammography pictures, normal (left) and cancerous (right) -
 Mastectomy patient
Mastectomy patient -
 Typical macroscopic (gross) appearance of the cut surface of a mastectomy specimen containing a cancer, in this case, an invasive ductal carcinoma of the breast, pale area at the center
Typical macroscopic (gross) appearance of the cut surface of a mastectomy specimen containing a cancer, in this case, an invasive ductal carcinoma of the breast, pale area at the center -
 Infiltrating ductal carcinoma of the breast
Infiltrating ductal carcinoma of the breast -
 Excised human breast tissue, showing a stellate area of cancer 2cm in diameter. The lesion could be felt clinically as a hard mobile lump, not attached to skin or chest wall.
Excised human breast tissue, showing a stellate area of cancer 2cm in diameter. The lesion could be felt clinically as a hard mobile lump, not attached to skin or chest wall. -
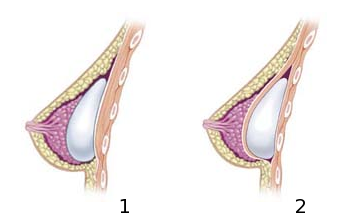 Diagrams of cross sections of breast implants, subglandular (left) and submuscular (right)
Diagrams of cross sections of breast implants, subglandular (left) and submuscular (right) -
 Grade IV capsular contracture in breast implant patient
Grade IV capsular contracture in breast implant patient




.png)













{kind=link}
External links
| Wikimedia Commons has media related to Breasts. |
- Images of female breasts
- Pregnancy and your breasts
- Stages of breast development, from Puberty101
- “Are Women Evolutionary Sex Objects?: Why Women Have Breasts”
- Breast subareolar excision : Operation Script on Wikisurgery.
- Breast subareolar excision daycase : Information for patients on Wikisurgery.
- Fine needle aspiration: Operation Script on Wikisurgery.
- Mastectomy subcutaneous male daycase: Information for patients on Wikisurgery.
- Trucut needle biopsy: Operation Script on Wikisurgery.
Template:Human anatomical features
Template:Female reproductive system
Template:Sex
ar:ثدي ay:Ñuñu bg:Гърда ca:Pit cs:Prs da:Bryst de:Weibliche Brust eo:Mamo eu:Bular hr:Dojka io:Mamo ilo:Suso id:Payudara is:Brjóst it:Mammella he:שד (איבר) pam:Susu ku:Çiçik la:Mamma lt:Krūtis ln:Libɛ́lɛ ml:സ്തനം nl:Borst no:Bryst nn:Bryst qu:Ñuñu scn:Minna (senu dâ fìmmina) simple:Breast sk:Prsník fi:Rinnat sv:Bröstkörtlar th:เต้านม uk:Груди yi:ברוסטען
- CS1 maint: Explicit use of et al.
- Pages with citations using unsupported parameters
- Pages using citations with accessdate and no URL
- CS1 errors: dates
- Pages with script errors
- Commons category link is locally defined
- Breast
- Exocrine system
- Female reproductive system
- Anatomy
- Glands
- Secondary sexual characteristics
- Integumentary system