*Histoloigically, well-differentiated [[neuroendocrine tumor]] have characteristic "[[organoid]]" arrangements of [[Tumor cell|tumor]] [[cells]], with solid/nesting, trabecular, [[gyriform]], or sometimes, [[glandular]] patterns.
*Histoloigically, well-differentiated [[neuroendocrine tumor]] have characteristic "[[organoid]]" arrangements of [[Tumor cell|tumor]] [[cells]], with solid/nesting, trabecular, [[gyriform]], or sometimes, [[glandular]] patterns.
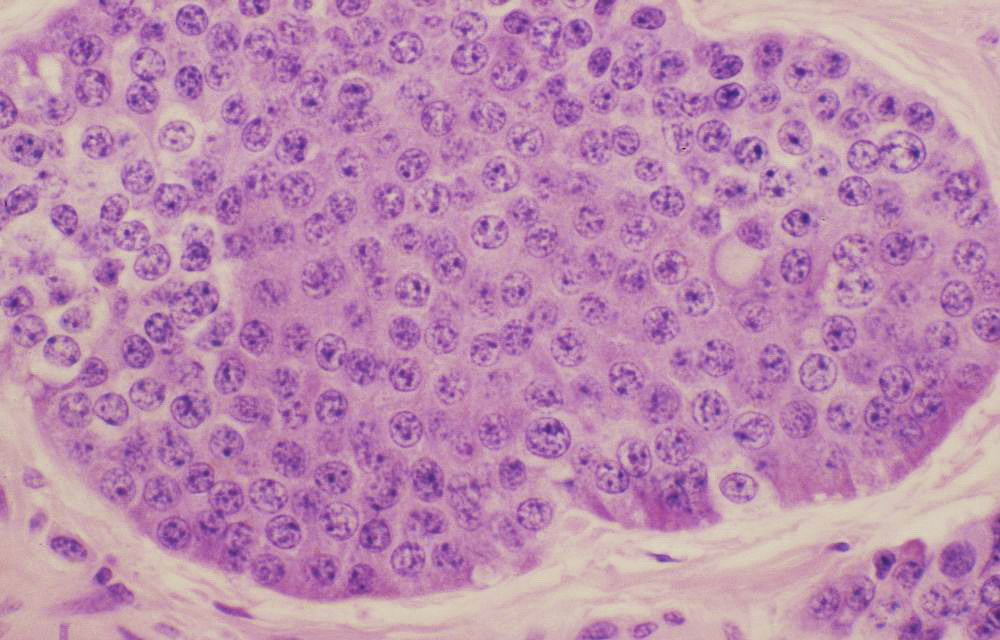
*The [[cells]] are relatively uniform, and they have round to oval nuclei, coarsely stippled [[Chromatin|chromatin,]] and finely [[Granularity|granular]] [[Cytoplasmic|cytoplasm]].
*The [[cells]] are relatively uniform, and they have round to oval nuclei, coarsely stippled [[Chromatin|chromatin,]] and finely [[Granularity|granular]] [[Cytoplasmic|cytoplasm]].
*The [[cells]] produce abundant [[Neurosecretory|neurosecretory granules]], as reflected in the strong and diffuse [[immunohistochemical]] expression of [[Neuroendocrine cells|neuroendocrine markers]] such as [[synaptophysin]], [[neuron-specific enolase]] and [[chromogranin]].<ref name="pmid15104570">{{cite journal |vauthors=Nehar D, Lombard-Bohas C, Olivieri S, Claustrat B, Chayvialle JA, Penes MC, Sassolas G, Borson-Chazot F |title=Interest of Chromogranin A for diagnosis and follow-up of endocrine tumours |journal=Clin. Endocrinol. (Oxf) |volume=60 |issue=5 |pages=644–52 |date=May 2004 |pmid=15104570 |doi=10.1111/j.1365-2265.2004.02030.x |url=}}</ref>
*The [[cells]] produce abundant [[Neurosecretory|neurosecretory granules]], as reflected in the strong and diffuse [[immunohistochemical]] expression of [[Neuroendocrine cells|neuroendocrine markers]] such as [[synaptophysin]], [[neuron-specific enolase]] and [[chromogranin]].<ref name="pmid15104570">{{cite journal |vauthors=Nehar D, Lombard-Bohas C, Olivieri S, Claustrat B, Chayvialle JA, Penes MC, Sassolas G, Borson-Chazot F |title=Interest of Chromogranin A for diagnosis and follow-up of endocrine tumours |journal=Clin. Endocrinol. (Oxf) |volume=60 |issue=5 |pages=644–52 |date=May 2004 |pmid=15104570 |doi=10.1111/j.1365-2265.2004.02030.x |url=}}</ref><ref name="pmid20217257">{{cite journal |vauthors=Modlin IM, Gustafsson BI, Moss SF, Pavel M, Tsolakis AV, Kidd M |title=Chromogranin A--biological function and clinical utility in neuro endocrine tumor disease |journal=Ann. Surg. Oncol. |volume=17 |issue=9 |pages=2427–43 |date=September 2010 |pmid=20217257 |doi=10.1245/s10434-010-1006-3 |url=}}</ref>
*Well-differentiated [[neuroendocrine tumor]] of the [[midgut]] [[Ileum|(ileum]] in particular) also have a very characteristic pattern of [[solid]] or cribriform nests punctuated by sharply outlined luminal spaces with peripheral [[nuclear]] [[palisading]] and [[Granular cell|granular]] [[eosinophilic]] [[Cytoplasmic|cytoplasm]].
*Well-differentiated [[neuroendocrine tumor]] of the [[midgut]] [[Ileum|(ileum]] in particular) also have a very characteristic pattern of [[solid]] or cribriform nests punctuated by sharply outlined luminal spaces with peripheral [[nuclear]] [[palisading]] and [[Granular cell|granular]] [[eosinophilic]] [[Cytoplasmic|cytoplasm]].
*Poorly differentiated [[Neuroendocrine tumor|neuroendocrine carcinomas]] (NECs) less closely resemble [[nonneoplastic]] [[neuroendocrine cells]] and have a more sheet-like or diffuse architecture, irregular [[nuclei]], and less [[cytoplasmic]] [[granularity]]. [[Immunohistochemical|Immunohistochemica]]<nowiki/>l expression of [[Neuroendocrine cells|neuroendocrine]] markers is generally more limited in extent and intensity.
*Poorly differentiated [[Neuroendocrine tumor|neuroendocrine carcinomas]] (NECs) less closely resemble [[nonneoplastic]] [[neuroendocrine cells]] and have a more sheet-like or diffuse architecture, irregular [[nuclei]], and less [[cytoplasmic]] [[granularity]]. [[Immunohistochemical|Immunohistochemica]]<nowiki/>l expression of [[Neuroendocrine cells|neuroendocrine]] markers is generally more limited in extent and intensity.
Carcinoid syndrome is encountered uncommonly and most often with tumors of large size (>5 cm).
Left upper lobe": A lung lobe 185x110x55mm with bronchovascular remnants up to 25mm. Arising in the hilum and involving the bronchus is a rubbery tan-pink tumor 21x20x19mm. The tumor is 6mm from the bronchovascular margins and 3mm from the hilar margin. 26mm from the tumor and 1mm from the pleura there is a firm white nodule 6mm. Peripheral to the tumor is an area where the lung shows dilated bronchi up to 12mm in diameter which lie 2mm from the pleura.Source: Radiopedia
↑Kvols LK, Moertel CG, O'Connell MJ, Schutt AJ, Rubin J, Hahn RG (September 1986). "Treatment of the malignant carcinoid syndrome. Evaluation of a long-acting somatostatin analogue". N. Engl. J. Med. 315 (11): 663–6. doi:10.1056/NEJM198609113151102. PMID2427948.
↑Grozinsky-Glasberg S, Grossman AB, Gross DJ (2015). "Carcinoid Heart Disease: From Pathophysiology to Treatment--'Something in the Way It Moves'". Neuroendocrinology. 101 (4): 263–73. doi:10.1159/000381930. PMID25871411.
↑Launay JM, Birraux G, Bondoux D, Callebert J, Choi DS, Loric S, Maroteaux L (February 1996). "Ras involvement in signal transduction by the serotonin 5-HT2B receptor". J. Biol. Chem. 271 (6): 3141–7. PMID8621713.
↑Xu J, Jian B, Chu R, Lu Z, Li Q, Dunlop J, Rosenzweig-Lipson S, McGonigle P, Levy RJ, Liang B (December 2002). "Serotonin mechanisms in heart valve disease II: the 5-HT2 receptor and its signaling pathway in aortic valve interstitial cells". Am. J. Pathol. 161 (6): 2209–18. doi:10.1016/S0002-9440(10)64497-5. PMID12466135.
↑Luis SA, Pellikka PA (January 2016). "Carcinoid heart disease: Diagnosis and management". Best Pract. Res. Clin. Endocrinol. Metab. 30 (1): 149–58. doi:10.1016/j.beem.2015.09.005. PMID26971851.
↑Druce MR, Bharwani N, Akker SA, Drake WM, Rockall A, Grossman AB (March 2010). "Intra-abdominal fibrosis in a recent cohort of patients with neuroendocrine ('carcinoid') tumours of the small bowel". QJM. 103 (3): 177–85. doi:10.1093/qjmed/hcp191. PMID20123681.
↑Pantongrag-Brown L, Buetow PC, Carr NJ, Lichtenstein JE, Buck JL (February 1995). "Calcification and fibrosis in mesenteric carcinoid tumor: CT findings and pathologic correlation". AJR Am J Roentgenol. 164 (2): 387–91. doi:10.2214/ajr.164.2.7839976. PMID7839976.
↑Daskalakis K, Karakatsanis A, Stålberg P, Norlén O, Hellman P (January 2017). "Clinical signs of fibrosis in small intestinal neuroendocrine tumours". Br J Surg. 104 (1): 69–75. doi:10.1002/bjs.10333. PMID27861745.
↑General Information About Gastrointestinal (GI) Carcinoid Tumors.<ref name="pmid2886072">Duh QY, Hybarger CP, Geist R, Gamsu G, Goodman PC, Gooding GA, Clark OH (July 1987). "Carcinoids associated with multiple endocrine neoplasia syndromes". Am. J. Surg. 154 (1): 142–8. PMID2886072.
↑Karatzas G, Kouraklis G, Karayiannakis A, Patapis P, Givalos N, Kaperonis E (June 2000). "Ampullary carcinoid and jejunal stromal tumour associated with von Recklinghausen's disease presenting as gastrointestinal bleeding and jaundice". Eur J Surg Oncol. 26 (4): 428–9. doi:10.1053/ejso.1999.0911. PMID10873367.
↑Fujimori M, Ikeda S, Shimizu Y, Okajima M, Asahara T (September 2001). "Accumulation of beta-catenin protein and mutations in exon 3 of beta-catenin gene in gastrointestinal carcinoid tumor". Cancer Res. 61 (18): 6656–9. PMID11559529.
↑Nehar D, Lombard-Bohas C, Olivieri S, Claustrat B, Chayvialle JA, Penes MC, Sassolas G, Borson-Chazot F (May 2004). "Interest of Chromogranin A for diagnosis and follow-up of endocrine tumours". Clin. Endocrinol. (Oxf). 60 (5): 644–52. doi:10.1111/j.1365-2265.2004.02030.x. PMID15104570.
↑Modlin IM, Gustafsson BI, Moss SF, Pavel M, Tsolakis AV, Kidd M (September 2010). "Chromogranin A--biological function and clinical utility in neuro endocrine tumor disease". Ann. Surg. Oncol. 17 (9): 2427–43. doi:10.1245/s10434-010-1006-3. PMID20217257.
.JPG)


.jpg){kind=link}