Right bundle branch block
| Right bundle branch block | |
 | |
|---|---|
| ECG characteristics of a typical RBBB showing wide QRS complexes with a terminal R wave in lead V1 and slurred S wave in lead V6. | |
| ICD-10 | I45.1 |
| DiseasesDB | 11620 |
| eMedicine | ped/2500 |
| Cardiology Network |
 Discuss Right bundle branch block further in the WikiDoc Cardiology Network |
| Adult Congenital |
|---|
| Biomarkers |
| Cardiac Rehabilitation |
| Congestive Heart Failure |
| CT Angiography |
| Echocardiography |
| Electrophysiology |
| Cardiology General |
| Genetics |
| Health Economics |
| Hypertension |
| Interventional Cardiology |
| MRI |
| Nuclear Cardiology |
| Peripheral Arterial Disease |
| Prevention |
| Public Policy |
| Pulmonary Embolism |
| Stable Angina |
| Valvular Heart Disease |
| Vascular Medicine |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Please Join in Editing This Page and Apply to be an Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [3] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Right bundle branch block (RBBB) results from a defect in the heart's electrical conduction system. There is a delay in failure of transmission of electrical impulses down the right bundle of the heart. As a result, the right ventricle depolarizes by an alternate mechanism. This is by means of cell-to-cell conduction. These cell to cell conduction impulses spread more slowly than usual from the interventricular septum to the left ventricle and to the right ventricle. This delay in conduction results in the characteristic ECG pattern which is a wide and notched QRS. Although conduction down the right bundle is delayed, conduction down the left bundle is normal. As result, the interventricular septum and left ventricle depolarize in the normal fashion.
ECG diagnosis
- The heart rhythm must be supraventricular in origin
- The QRS axis can be either normal, or right or left axis deviation may be present.
- The QRS duration must be = or > 120 ms
- For complete RBBB, the patient's age must be taken into account to determine if the duration of the QRS complex is prolonged for the patient's age.
- Maximum QRS durations are 0.07 s for newborns <6 days, 0.08 s for patients aged 1 week to 7 years, and 0.09 s for patients aged 7-15 years.
- For complete RBBB, the patient's age must be taken into account to determine if the duration of the QRS complex is prolonged for the patient's age.
- There should be a terminal R wave in lead V1-V3R (e.g., R, rR', rsR', rSR' or qR')
- This pattern is present because the initial R wave represents septal activation, the S wave represents left ventricular activation, and the R' represents activation of the right ventricle from the septum and left ventricle.
- There should be a slurred S wave in leads I and V6. This represent left ventricular activation.
- Because transmission of the electrical impulse through the left bundle is normal, this results in normal depolarization of the septum and the left ventricle. As a result, there is an initial R wave in lead I and V1 and the Q wave in V6.
The T wave should be deflected opposite the terminal deflection of the QRS complex. This is known as appropriate T wave discordance with bundle branch block. A concordant T wave may suggest ischemia or myocardial infarction.
The prevalence of RBBB increases with age.
Three Anatomic Locations of Right Bundle Branch Block
In each of the three types of RBBB, the surface ECG pattern remains the same.
Three types of RBBB have been identified based upon electrophysiologic studies.
1. Proximal, or central, RBBB: This type of conduction defect occurs when the conduction block is located just distal to the bundle of His in the superior aspect of the right bundle branch. This type of block occurs when the proximal bundle is injured during surgery for an inlet or membranous ventricular septal defect (VSD).
2. Interruption between the proximal and distal aspects of the right bundle branch: This type of right bundle branch block occurs when the impulse is interrupted between the proximal and distal aspects of the right bundle branch. This type of bright bundle branch block is most commonly observed after surgical division of the moderator band.
3. Distal RBBB: This form is observed when distal ramifications of the right bundle are disrupted during right ventriculotomy or resection of muscle bundles in the right ventricular outflow tract.
Genetics
There can be familial cases of right bundle branch block such as that observed in 4 Lebanese families and the abnormality was mapped to chromosome 19.
There is a subset of patients with Brugada syndrome who have mutations in SCN5A, the gene encoding for the voltage-gated cardiac sodium channel.
Differential Diagnosis
- Acute pulmonary embolism
- Atrial septal defect
- Cardiomyopathy
- Cor Pulmonale
- Coronary Heart Disease
- Lenegre's Disease
- Lev's Disease
- Myocardial Infarction
- Myocarditis
Causes of Right Bundle Branch Block
- Surgery for correction of congenital heart disease is the most common cause of RBBB among children any United States. This includes surgery for repair of an isolated VSD or another congenital heart disease that includes a VSD (eg, double-chambered right ventricle, AV canal defect, or tetralogy of Fallot). The incidence of RBBB varies and ranges from 25-81% after repair of a VSD to 60-100% after repair of tetralogy of Fallot. The risk of RBBB after surgery varies depending upon the proximity of the VSD to the His-Purkinje system.
- Blunt trauma
- Polymyositis
- Premature atrial contractions or supraventricular tachycardia may cause a transient form up right bundle branch block. This occurs when a premature impulse is conducted from the AV node to the His bundle while the right bundle branch remains in its refractory period, but the left bundle is not. As a result, conduction down the right bundle branch is delayed or blocked.
- Prenatal exposure to each one HIV type 1 may cause right anterior hemiblock.
- Familial
Associated syndromes
- Myotonic dystrophy Other ECG findings include first-degree AV block, left anterior fascicular block, and intraventricular conduction delay. Patients may have arrhythmias and/or Stokes-Adams attacks.
- Brugada syndrome: This syndrome is due to a channelopathy mediated by the SCN5A gene. It is important to note that the RBBB pattern seen in patients with this syndrome is not actually RBBB but is instead due to a repolarization abnormality. In this syndrome, the ECG shows ST-segment elevation in leads V1-V3. Cocaine consumption and / or the use of the antiarrhythmic propafenone may unmask the ECG findings of Brugada syndrome.
Natural history of right bundle branch block
In general, the natural history of right bundle branch block benign. There are three scenarios in which right bundle branch block can be associated with poor prognosis:
- Brugada syndrome: if right bundle branch block is present, then sudden death may occur.
- Kearns Sayre syndrome: again, if right bundle branch block is present than sudden death may occur.
- Tetralogy of Fallot: if right bundle branch block is present with a markedly prolonged QRS (< 180 ms), then the patient may be at risk for ventricular arrhythmias and sudden death.
If right bundle branch block is due to surgery then there are generally no acute hemodynamic consequences. The subsequent courses also quite benign. An exception is if there is substantial injury to the His-Purkinje system in which case left anterior hemiblock or first-degree AV block may be present.
There are familial cases of right bundle branch block, which are benign.
Physical examination
Right bundle branch block is associated with a persistently split second heart sound with normal respiratory variation in the splitting interval.
Laboratory Evaluation
If there is a history of blunt trauma or any symptoms to suggest polymyositis then troponin, creatine kinase (CK) and an echocardiogram should be obtained.
Treatment
In general treatment for right bundle branch block is not necessary. These patients need not limit their activity. However, if the RBBB progresses to heart block, the patient may be at risk for adverse clinical outcomes. In these patients further electrophysiologic testing may be necessary. Those patients who develop right bundle branch block after surgery should undergo EKG testing each year to evaluate for interval changes. In particular, care should be taken to observe for the development of sinus bradycardia supraventricular or ventricular ectopy.
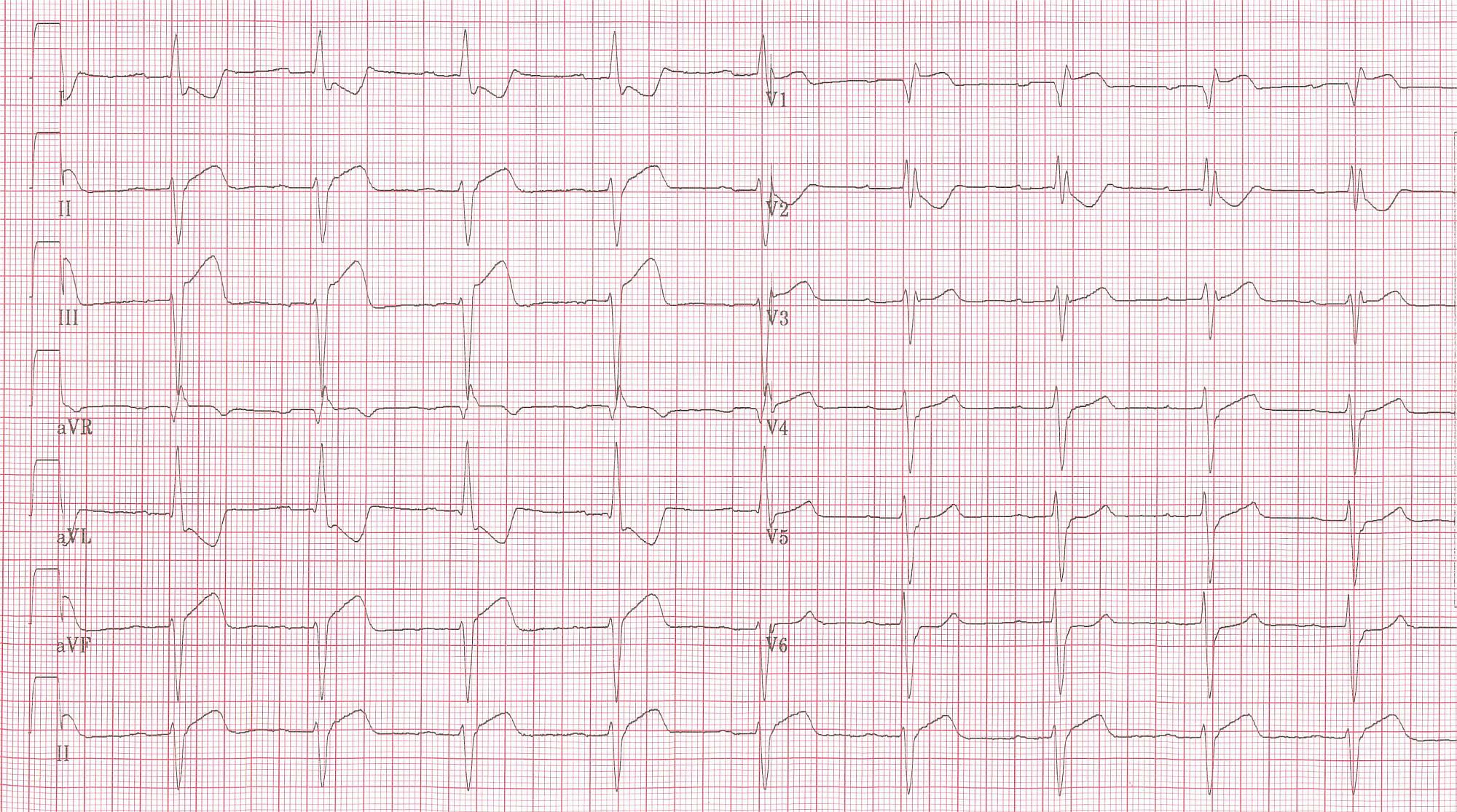
EKG Examples
-
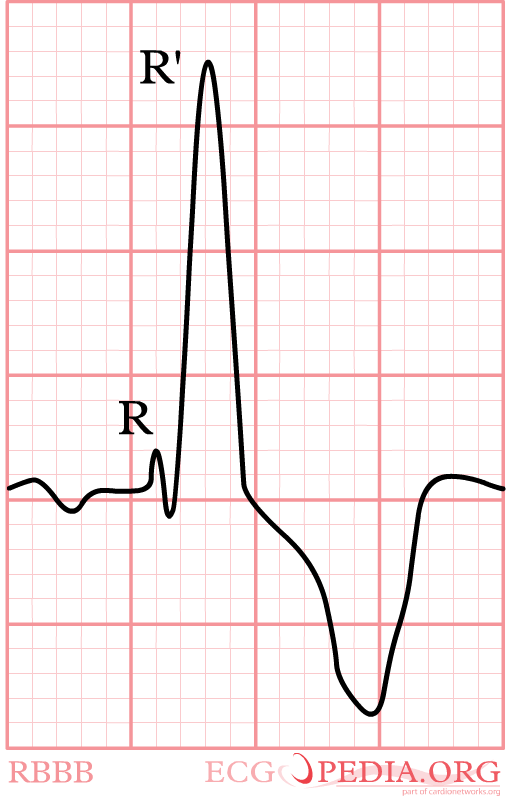
The main characteristics of Right Bundle Branch Block in V1







-

-

Right Bundle Branch Block with RA hypertrophy. Image courtesy of Dr Jose Ganseman


-
Patient with RBBB and inferior MI. Note to left axis deviation.
-

The same patient. Lead V4R. ST elevation shown.


-

The same patient before acute MI developed. Horizontal axis shown.
-



-

-
![Anterior MI] with RBBB and LAFB. Image courtesy of Dr Jose Ganseman](/images/c/c5/Right_bundle_branch_block_18.jpg)
Anterior MI] with RBBB and LAFB. Image courtesy of Dr Jose Ganseman

![Anterior MI] with RBBB and LAFB. Image courtesy of Dr Jose Ganseman](/index.php/File:Right_bundle_branch_block_18.jpg)





{kind=link}
Animation of RBBB
<youtube v=EJUQKaDeAXg/>