Rheumatic fever: Difference between revisions
| Line 27: | Line 27: | ||
==General information== | ==General information== | ||
'''Rheumatic fever''', and therefore Streptococus pyogenes infections, are endemic in most countries of the world. In countries | '''Rheumatic fever''', and therefore Streptococus pyogenes infections, are endemic in most countries of the world. In countries affected by the industrial revolution, living conditons became less crowded and generally more hygienic and so Streptococcus pyogenes infections became less common and less severe. The introduction of antibiotics, first sulfonamide in the 1930's, further caused Streptococcus pyogenes infections to become less common although they never disappeared. | ||
The development of a rheumatic fever episode depends on | The development of a rheumatic fever episode, depends on the involved host being highly autoimmunologically sensitized to autoantigens exhibited to the host during prior Streptococcus pyogenes during infections, so a decrease in the frequency of infections, and the virulence of infections, in a society can cause rheumatic fever, as a disease entity, to be remarkably reduced. | ||
Rheumatic fever affects individuals who are thought to be "young and healthy", for instance, individuals between four years and fifty, but in most eras it was most common in children between the six and | Rheumatic fever affects individuals who are thought to be "young and healthy", for instance, individuals between four years and fifty years of age, but in most eras it was most common in children between the six and thirty. The reason children younger than four years, or so, do not ''usually'' develop rheumatic fever is that an individual must have sufficient, prior stimulation by Streptococcus pyogens autoantigens, which is, typically, caused by multiple infections by Streptococcus pyogenes, over time, and that situation is ''less likely'' to occur in younger children(although it does happen!). Older individuals are expected, somewhat, to develop diseases of aging and so it is often not surprising when they become sick; it is surprising when individuals in their teens, twenties, thirties, forties and even fifties, for instance, become very sick so those cases attract more "medical" attention. Individuals of all ages, however, can develop rheumatic fever. | ||
Scarlet fever and rheumatic fever are, primarily, the same disease. The somewhat typical rash of scarlet fever develops if an individual contracts an infecton from a strain of Streptococcus pyogenes that secretes erythrotoxin A, B, and C, and if the individual involved has not had an infection by that particular strain previously, since during a previous infection antibodies will have been developed against the erythrotoxin of interest. Repeated infections by strains of Streptococcus pyogenes that have, and do not have, erythrotoxin A, B, and C can reinforce each other in the development of autoimmunological reactions by a host, since they all have certain autoantigens and secreted toxic products, other than erythrotoxin A, B, and C, in common. Children are less likely to have experienced repeated autoimmunological stimulation by various strains of Streptococcus pyogenes and therefore they are less autoimmunologically sensitized, in general, to its autoantigens. If a young child, usually, develops an infection from Streptococcus pyogenes that secretes A, B, or C erythrotixin they will develop a mild infectious/autoimmunological disease and the classic, mild rash of scarletina, the diminuative term for scarlet fever, will often develop. | Scarlet fever and rheumatic fever are, primarily, the same disease. The somewhat typical rash of scarlet fever develops if an individual contracts an infecton from a strain of Streptococcus pyogenes that secretes erythrotoxin A, B, and C, and if the individual involved has not had an infection by that particular strain previously, since during a previous infection antibodies will have been developed against the erythrotoxin of interest. Repeated infections by strains of Streptococcus pyogenes that have, and do not have, erythrotoxin A, B, and C can reinforce each other in the development of autoimmunological reactions by a host, since they all have certain autoantigens and secreted toxic products, other than erythrotoxin A, B, and C, in common. Children are less likely to have experienced repeated autoimmunological stimulation by various strains of Streptococcus pyogenes and therefore they are less autoimmunologically sensitized, in general, to its autoantigens. If a young child, usually, develops an infection from Streptococcus pyogenes that secretes A, B, or C erythrotixin they will develop a mild infectious/autoimmunological disease and the classic, mild rash of scarletina, the diminuative term for scarlet fever, will often develop. | ||
Since the development of rheumatic fever depends | Since the development of rheumatic fever depends upon a prior, high-level of autoimmunological stimulation, which itself depends upon an individual, in the past, experiencing many infectious episodes by Streptococcus pyogenes, and since Streptococcus pyogenes are endemic in human and domestic animal populations (information from the Russian Encyclopedia (Nasonova,Talahaev), it must be understood that all individuals experience pathological, autoimmunological stimulation during Streptococcus pyogenes infections. | ||
The rate of development of rheumatic fever, in a somewhat homogeneous population, will depend upon the environmental conditions mentioned above, wherein crowding and unhygienic living conditions are two of the most important. Information in the text ''Streptococcal | The rate of development of rheumatic fever, in a somewhat homogeneous population, will depend upon the environmental conditions mentioned above, wherein crowding and unhygienic living conditions are two of the most important. Information in the text ''Streptococcal Infections'' (Stevens, D., Kaplan, E., Oxford University Press, 2000) indicate that 1% to 70% of individuals in any given population are carriers of Streptococcus pyogenes and many of them are asymptomatic carriers. Perhaps, 2% to 4% of individuals who contract Streptoccus pyogenes infections develop recognizable rheumatic fever (but most mild cases go unrecognized) and of those, a low percentage, about 1% to 3% die from rheumatic fever. The frequency of rheumatic fever depends, to a great degree, upon the general level of Streptococcal pyogenic, autoimmunological stimulation that exists within members of a given population. | ||
Contrary to the immunological protection developed during most other infections, wherein individuals develop immunity to | Contrary to the immunological protection developed during most other infections, wherein individuals develop immunity to the microorganism that causes a certain infection, infections by Streptococcus pyogenes cause both a protective immunological and a pathological autoimmunological stimulation and so repeated infections by Streptococcus pyogenes will cause both a heightened protective immune and pathological autoimmune response. The immune response causes Streptococcus pyogenes to be controlled, but the concomitant, autoimmunological response causes an inflammatory, systemic, disease process to be developed within the affected individual. The systemic, autoimmunological disease process is termed '''rheumatic fever''' and it is a sequela to the triggering Streptococcus pyogenes infection. | ||
When an individual develops | When an individual develops rheumatic fever, they experience further sensitization to Streptococcus pyogenes autoantigens. An infection by a virulent strain of Streptococcus pyogenes, at a later date, will likely cause an elevated autoimmunological response and a recurrent case, probably a more severe case, of rheumatic fever will develop. | ||
If an individual does not contract a Streptococcus pyogenes infection for a long period, for | If an individual does not contract a Streptococcus pyogenes infection for a long period, perhaps for five years or longer, the individual's immunological/autoimmunological responsivness will naturally decrease and, perhaps, there will be a less chance of developing rheumatic fever if the individual contracts a future Streptococcus pyogenes infection. | ||
The above natural phenomenon is the basis for the use of prophylactic penicillin therapy for individuals, and populations of individuals, who are at risk for rheumatic fever. Providing individuals who have had rheumatic fever with monthly (or maybe every three weeks) injections of Benzathine Penicillin G,1,200,000 units, or oral penicillin VK or G, 250mg twice daily, decreases the frequency of recurrent Streptococcus pyogenes infections and therefore recurrent rheumatic fever episodes. It is estimated that the recurrence rate of rheumatic fever is decreased about 85% by providing prophylactic penicillin therapy. | The above natural phenomenon is the basis for the use of prophylactic penicillin therapy for individuals, and populations of individuals, who are at risk for rheumatic fever. Providing individuals who have had rheumatic fever with monthly (or maybe every three weeks) injections of Benzathine Penicillin G, 1,200,000 units, or oral penicillin VK or G, 250mg twice daily (I think 500 mg twice daily is more efficacious), decreases the frequency of recurrent Streptococcus pyogenes infections and therefore recurrent rheumatic fever episodes. It is estimated that the recurrence rate of rheumatic fever is decreased about 85% by providing prophylactic penicillin therapy. | ||
Streptococcus pyogenes is a complex microorganism and it causes many disease entities both from the suppurative aspect of Streptococcus pyogenes infections and from nonsuppurative, systemic, autoimmunological sequelae to the infections. The nonsuppurative, systemic, autoimmunological sequelae are inflammatory in nature and therefore all tissues and organs are affected, but certain organs are noted to be affected in an important and acute fashion: the heart and kidneys. | Streptococcus pyogenes is a complex microorganism and it causes many disease entities both from the suppurative aspect of Streptococcus pyogenes infections and from nonsuppurative, systemic, autoimmunological sequelae to the infections. The nonsuppurative, systemic, autoimmunological sequelae are inflammatory in nature and therefore all tissues and organs are affected, but certain organs are noted to be affected in an important and acute fashion: the heart and kidneys. | ||
Revision as of 23:06, 25 February 2010
| Rheumatic fever | |
 | |
|---|---|
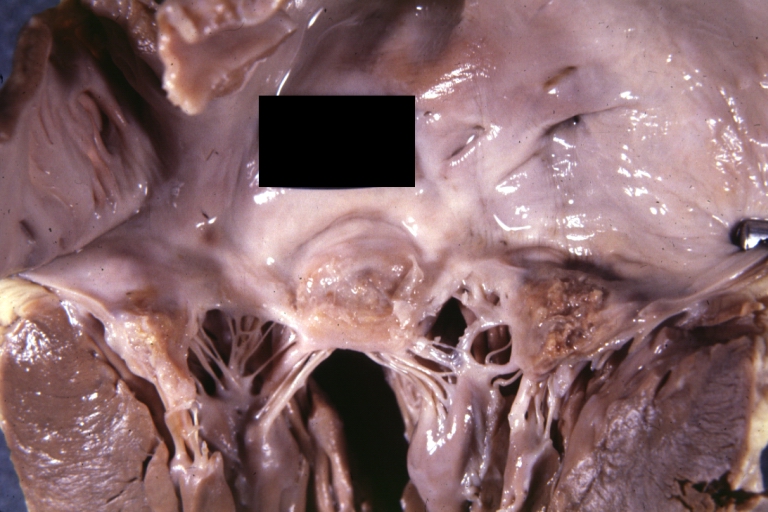
| Rheumatic Mitral Valvulitis: Gross; an excellent example of acute rheumatic fever lesion along line of closure of mitral valve Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology | |
| ICD-10 | I00-I02 |
| ICD-9 | 390–392 |
| DiseasesDB | 11487 |
| MedlinePlus | 003940 |
| eMedicine | med/3435 med/2922 emerg/509 ped/2006 |
| MeSH | D012213 |
|
WikiDoc Resources for Rheumatic fever |
|
Articles |
|---|
|
Most recent articles on Rheumatic fever Most cited articles on Rheumatic fever |
|
Media |
|
Powerpoint slides on Rheumatic fever |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Rheumatic fever at Clinical Trials.gov Trial results on Rheumatic fever Clinical Trials on Rheumatic fever at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Rheumatic fever NICE Guidance on Rheumatic fever
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Rheumatic fever Discussion groups on Rheumatic fever Patient Handouts on Rheumatic fever Directions to Hospitals Treating Rheumatic fever Risk calculators and risk factors for Rheumatic fever
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Rheumatic fever |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
| Cardiology Network |
 Discuss Rheumatic fever further in the WikiDoc Cardiology Network |
| Adult Congenital |
|---|
| Biomarkers |
| Cardiac Rehabilitation |
| Congestive Heart Failure |
| CT Angiography |
| Echocardiography |
| Electrophysiology |
| Cardiology General |
| Genetics |
| Health Economics |
| Hypertension |
| Interventional Cardiology |
| MRI |
| Nuclear Cardiology |
| Peripheral Arterial Disease |
| Prevention |
| Public Policy |
| Pulmonary Embolism |
| Stable Angina |
| Valvular Heart Disease |
| Vascular Medicine |
Editor-in-Chief: Lance Christiansen, D.O.
Associate Editor: Cafer Zorkun, M.D., Ph.D. [1]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [2] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
The systemic signs and symptoms of rheumatic fever are caused primarily by an attack on a host's tissues by autoantibodies, and other autoimmunological elements, that are self-developed by a host, who has had prior, adequate, autoimmunological stimulation to Streptococcus pyogenes autoantibodies and secreted toxic products. A rheumatic fever episode is primarily an autoimmunological sequela of a Streptococcus pyogenes infection and not a function of direct pathological damage from the bacteria itself.
General information
Rheumatic fever, and therefore Streptococus pyogenes infections, are endemic in most countries of the world. In countries affected by the industrial revolution, living conditons became less crowded and generally more hygienic and so Streptococcus pyogenes infections became less common and less severe. The introduction of antibiotics, first sulfonamide in the 1930's, further caused Streptococcus pyogenes infections to become less common although they never disappeared.
The development of a rheumatic fever episode, depends on the involved host being highly autoimmunologically sensitized to autoantigens exhibited to the host during prior Streptococcus pyogenes during infections, so a decrease in the frequency of infections, and the virulence of infections, in a society can cause rheumatic fever, as a disease entity, to be remarkably reduced.
Rheumatic fever affects individuals who are thought to be "young and healthy", for instance, individuals between four years and fifty years of age, but in most eras it was most common in children between the six and thirty. The reason children younger than four years, or so, do not usually develop rheumatic fever is that an individual must have sufficient, prior stimulation by Streptococcus pyogens autoantigens, which is, typically, caused by multiple infections by Streptococcus pyogenes, over time, and that situation is less likely to occur in younger children(although it does happen!). Older individuals are expected, somewhat, to develop diseases of aging and so it is often not surprising when they become sick; it is surprising when individuals in their teens, twenties, thirties, forties and even fifties, for instance, become very sick so those cases attract more "medical" attention. Individuals of all ages, however, can develop rheumatic fever.
Scarlet fever and rheumatic fever are, primarily, the same disease. The somewhat typical rash of scarlet fever develops if an individual contracts an infecton from a strain of Streptococcus pyogenes that secretes erythrotoxin A, B, and C, and if the individual involved has not had an infection by that particular strain previously, since during a previous infection antibodies will have been developed against the erythrotoxin of interest. Repeated infections by strains of Streptococcus pyogenes that have, and do not have, erythrotoxin A, B, and C can reinforce each other in the development of autoimmunological reactions by a host, since they all have certain autoantigens and secreted toxic products, other than erythrotoxin A, B, and C, in common. Children are less likely to have experienced repeated autoimmunological stimulation by various strains of Streptococcus pyogenes and therefore they are less autoimmunologically sensitized, in general, to its autoantigens. If a young child, usually, develops an infection from Streptococcus pyogenes that secretes A, B, or C erythrotixin they will develop a mild infectious/autoimmunological disease and the classic, mild rash of scarletina, the diminuative term for scarlet fever, will often develop.
Since the development of rheumatic fever depends upon a prior, high-level of autoimmunological stimulation, which itself depends upon an individual, in the past, experiencing many infectious episodes by Streptococcus pyogenes, and since Streptococcus pyogenes are endemic in human and domestic animal populations (information from the Russian Encyclopedia (Nasonova,Talahaev), it must be understood that all individuals experience pathological, autoimmunological stimulation during Streptococcus pyogenes infections.
The rate of development of rheumatic fever, in a somewhat homogeneous population, will depend upon the environmental conditions mentioned above, wherein crowding and unhygienic living conditions are two of the most important. Information in the text Streptococcal Infections (Stevens, D., Kaplan, E., Oxford University Press, 2000) indicate that 1% to 70% of individuals in any given population are carriers of Streptococcus pyogenes and many of them are asymptomatic carriers. Perhaps, 2% to 4% of individuals who contract Streptoccus pyogenes infections develop recognizable rheumatic fever (but most mild cases go unrecognized) and of those, a low percentage, about 1% to 3% die from rheumatic fever. The frequency of rheumatic fever depends, to a great degree, upon the general level of Streptococcal pyogenic, autoimmunological stimulation that exists within members of a given population.
Contrary to the immunological protection developed during most other infections, wherein individuals develop immunity to the microorganism that causes a certain infection, infections by Streptococcus pyogenes cause both a protective immunological and a pathological autoimmunological stimulation and so repeated infections by Streptococcus pyogenes will cause both a heightened protective immune and pathological autoimmune response. The immune response causes Streptococcus pyogenes to be controlled, but the concomitant, autoimmunological response causes an inflammatory, systemic, disease process to be developed within the affected individual. The systemic, autoimmunological disease process is termed rheumatic fever and it is a sequela to the triggering Streptococcus pyogenes infection.
When an individual develops rheumatic fever, they experience further sensitization to Streptococcus pyogenes autoantigens. An infection by a virulent strain of Streptococcus pyogenes, at a later date, will likely cause an elevated autoimmunological response and a recurrent case, probably a more severe case, of rheumatic fever will develop.
If an individual does not contract a Streptococcus pyogenes infection for a long period, perhaps for five years or longer, the individual's immunological/autoimmunological responsivness will naturally decrease and, perhaps, there will be a less chance of developing rheumatic fever if the individual contracts a future Streptococcus pyogenes infection.
The above natural phenomenon is the basis for the use of prophylactic penicillin therapy for individuals, and populations of individuals, who are at risk for rheumatic fever. Providing individuals who have had rheumatic fever with monthly (or maybe every three weeks) injections of Benzathine Penicillin G, 1,200,000 units, or oral penicillin VK or G, 250mg twice daily (I think 500 mg twice daily is more efficacious), decreases the frequency of recurrent Streptococcus pyogenes infections and therefore recurrent rheumatic fever episodes. It is estimated that the recurrence rate of rheumatic fever is decreased about 85% by providing prophylactic penicillin therapy.
Streptococcus pyogenes is a complex microorganism and it causes many disease entities both from the suppurative aspect of Streptococcus pyogenes infections and from nonsuppurative, systemic, autoimmunological sequelae to the infections. The nonsuppurative, systemic, autoimmunological sequelae are inflammatory in nature and therefore all tissues and organs are affected, but certain organs are noted to be affected in an important and acute fashion: the heart and kidneys.
Since the heart and kidneys are vital organs, and their functional failure causes the death of individuals, acute, rheumatic abnormalities to the heart and kidnesy that individuals experience are medically-noted more frequently than acute rheumatic damage to other organs. The symptoms and signs of acute rheumatic fever, however, indicates that virtually all tissues, and therefore organs, of the body are affected: connective tissue (arthritis); lethargy, stupor, seizures, coma, post-disease fatigue, tics, chronic mental disturbances such as obsessive-compulsive behavior and PANDAS (the brain); chorea (rheumatic encephalomyelitis); acute,congestive heart failure and pulmonary edema (the heart); autoimmune pneumonitis (the lungs); erythema marginatum, papulatum, miliary rash, and scarlet fever rash (the skin); autoimmune hepatitis (the liver); anemia of various types including aplastic anemia (bone marrow); acute, peripheral, painful neuropathies (peripheral nerves); nausea, vomiting, diarrhea, crampy abdominal pain (gastrointestinal organs); other organs such as the pancreas, endocrine organs, and elements of the circulatory system are also affected.
More important, perhaps, are the more chronic, inflammatory, autoimmunologial disease states, which have not been well appreciated in modern times, but which were understood, at least to some degree, during prior eras. Rheumatic fever, an acute, inflammatory, autoimmune disease state, was, from the 1600's, at least, until the early 1900's termed, often, acute rheumatism or acute articular rheumatism, and the chronic disease state of rheumatic, inflammatory autoimmunity was termed chronic rheumatism or simply, rheumatism. Galen, during the second century A.D. coined the word, rheumatismos and it was first used in post-renaissance times by Guillaume Bailou (1538-1616).
The chronic non-suppurative sequela of rheumatic fever, rheumatic heart-valve disease, is not caused by acute rheumatic fever, but it is due to a high-grade rheumatic, inflammatory, autoimmune state, which is caused by repeated, or at times chronic, infections by virulent strains of Streptococcus pyogenes. Rheumatic heart-valve disease is common in American society, but there is no outcry from treating cardiologists, and cardiac surgeons, concerning the ongoing development of the high-grade, chronic, rheumatic state within individuals in the American population.
Diagnosis of Rheumatic Fever The diagnosis of rheumatic fever has been historically difficult, but physicians since the 1500's understood, at least in part, the complex of signs and symptoms that indicated its existence. Thomas Sydenham discribed a case of severe rheumatic fever in the late 1600's and a similar discription is provided in the Encyclopedia Britanica, first edition, of 1771: "The rheumatism chiefly attacks persons in the flower of their age, after violent exercise, or a great heat of the body from anoy other cause, adn then being too suddenly cooled; but spares neither men nor women, old nor young...It begins with chilness and shivering, followed by inquietude and thirst. Which is preceded with spontaneous lassitude, a heaviness of the joints, and coldness of the extreme parts. When the fever appears, there is an inward heat, chiefly about the -praecordia, attended with anxiety. The pulse is quick and strait, the appetite is lost, and the body is coftive. In a day or two, sometimes sooner, the patient feels a racking pain, sometimes in one joint, sometimes in another, but more frequently in the wrists, shoulders and knees; frequently shifting from place to place, and leaving redness and swelling in the part visited last. The pain is exasperated upon the least motion; it sometimes attacks the loins and the coxendix. When it seizes the loins, it is called the lumbago; and there is a most violent pain in the small of the back,which sometimes extends to the os sacrum, and is like fit of the gravel...it may continue for months or years, but not always with the same violence, but by fits. If it continues and increases, it may cause a stiff joint, which will scarce yield to any remedy. Its proximate cause seems to be the inflammation of the lymphatic arteries...The chronic rheumatism is either the remains of a rheumatic fever, or a continuationof pains that proceeded at first from lesser but neglected colds."
As rheumatic fever, progressively, became less common as the advances of the industrial revolution were instituted into society, high-grade cases became less common. Fewer physicians took care of patients with severe rheumatic fever so it became a probematic diagnosis. During WW II conditions of over-crowding developed in military training sites, and at sites of war-making activities, so rheumatic fever, as a disease entity, became more common. Leaders in the U.S. Navy Medical Corps hired T. Duckett Jones, MD, an investigator in the area of rheumatic fever, to study rheumatic fever's epidemiology and clinical development and he devised certain sign and symptom criteria to provide an aid in diagnosing overt, severe, rheumatic fever. Those diagnostic criteria, published in 1944[1] have become known as the "Jones Criteria" and they are still currently used, in a modified form, to diagnose rheumatic fever. They have been periodically revised by the American Heart Association in collaboration with other groups.[2] Two major criteria, or one major and two minor criteria, when there is also evidence of a previous strep infection, support the diagnosis of rheumatic fever.[3][4]
Major criteria
- Carditis: inflammation of the heart muscle which can manifest as congestive heart failure with shortness of breath, pericarditis with a rub, or a new heart murmur.
- Migratory polyarthritis: a temporary migrating inflammation of the large joints, usually starting in the legs and migrating upwards.
- Sydenham's chorea (St. Vitus' dance): a characteristic series of rapid movements without purpose of the face and arms. This can occur very late in the disease.
- Erythema marginatum: a long lasting rash that begins on the trunk or arms as macules and spread outward to form a snakelike ring while clearing in the middle. This rash never starts on the face and is made worse with heat.
- Subcutaneous nodules (a form of Aschoff bodies): painless, firm collections of collagen fibers on the back of the wrist, the outside elbow, and the front of the knees. These now occur infrequently.
Minor criteria
- Fever: temperature elevation
- Arthralgia: Joint pain without swelling
- Laboratory abnormalities: increased Erythrocyte sedimentation rate, increased C reactive protein, leukocytosis
- Electrocardiogram abnormalities: a prolonged PR interval
- Evidence of Group A Strep infection: positive culture for Group A Strep, elevated or rising Antistreptolysin O titre
- Previous rheumatic fever or inactive heart disease
Other signs and symptoms
Unfortunately, since the 1930's, most physicians dealing with rheumatic fever have knowingly treated only a few cases and this causes only the very most high-grade cases to be recognized and the symptoms and signs of those cases are what compose the "Jones Criteria".
Sir William Osler indicates in his text, Osler's Principles and Practices of Medicine, Twelfth Edition (McCrea, T., D. Appleton-Century Company, 1935) presents many clinical and epidemiological factors concerning rheumatic fever. All physicians dealing with patient sicknesses should read it in its entirity. It does indicate that rheumatic fever is often a disease that exists commonly within family members (Streptococcus pyogenese is highly contagious), he indicates that it is due to a "hypersensitiveness" to...streptococci. "There is an initial lesion with more serious manifestations occuring elsewhere in the body...The initial lesion may be in the tonsils with resulting sensitization and subsequent attacks may be due to fresh infection or to areas of chronic infection (tonsils, sinuses)...A hypersensitive state once established, a chronic infection or a repeated slight infection may serve to prolong it and an acute infection may precipitate another attack."
Further, he indicates, "As a rule, the disease sets in abruptly, but it may be preceded by irregular pains in the joints, slight malaise, sore throat, and particularly by tonsillitis...A definite rigor is uncommon; more often there is a slight chilliness. The fever rises quickly, and one or more of the joints may become painful. Within twenty-four hours from the onset the disease is fully manifest. The temperature range is from 102 deg. to 104 deg. The pulse is frequent, soft, and usually above 100. The tongue is moist and covered wiht white fur. There are...loss of appetite, thirst, constipation, and scanty, highly acid urine. In the majority of cases there are profuse, acid sweats, of a paeculiar sour odor. Sudaminal and miliary vesicles are abundant, the latter being surrounded by a minute ring of hyperemia."
In addition Dr. Osler Indicates, "The affected joints become are painful to move, soon become swollen and hot, and present a reddish flush. The order of frequency of involvement of the joints in our series was knee, ankle, shoulder, wrist, elbow, hip, hand, foot. The joints are not attacked together, but successively. The amount of swelling is variable. Extensive effusion into a joint is ratre, and much of the enlargement is due to the infiltration of the periarticular tissues with serum."
Importantly, Dr. Osler indicates, "Perhaps no disease is more painful; the inability to change posture without agonizing pain, the drenching sweats, the prostration and helplessness, combine to make it a most distressing affection...In children there may be no arthritis whatever or if present only in a mild form...The blood is profoundly altered and there is no acute febrile disease in which an anemia occurs with greater rapidity...The average leucocyte count in our cases was about 12,000 per c. mm. Epistaxis is not uncommon...With a high fever a murmur may often be heard at the apex region...Febrile albuminuria is not uncommon. Hematuria occurs occassionally."
Rheumatic fever is highly variable, enough so that a rigid set of criteria, such as the Jones Criteria, is somewhat superficial and only meaninful in high-grade cases of rheumatic fever. Dr. Osler continues with the following most important information: "Subacute rheumatic fever represents a milder form of the disease, in which all the symptoms are less pronounced. The fever rarely rises above 101 deg. F.; fewer joints are involved; and the arthritis is less intense. The cases may drag on for weeks or months. It should not be forgotten that mild or subacute forms may be associated with endocarditis or pericarditis.
The influence of age on the manifestations is marked. While the usual description applies to the disease as seen in adults, in young children there may not be any pronounced arthritis or any arthritis at all, and the discovery of endocarditis often suggests the diagnosis. Endocarditis and myocarditis are the prominant features in children in whom the picture may be very variable. The onset may be so insidious that it can hardly be termed even subacute. Ill health without any evident cause, loss of weight, anorexia, fatigue, complaint of slight pains and fever with no apparent cause should suggest the possibility. Acute arthritis is the exception in the child; cardiac involvement of some kind is the rule."
It is very difficult to record the symptoms and signs of a disease with so much variation, depending on the age of the sik individual, depending on the level of prior rheumatic sensitization, depending on the strain of Streptococcus pyogenes involved in the acute infection, depending on the pattern of infection and its secondary autoimmunological response, and on prior autoimmunological damage that has taken place during prior rheumatic, autoimmunological episodes. Then there is random chance that is enhanced in complex systemic diseases.
Pathophysiology
Rheumatic fever is a systemic disease affecting the peri-arteriolar connective tissue and can occur after an untreated Group A streptococcal pharyngeal infection. It is believed to be caused by antibody cross-reactivity. This cross-reactivity is a Type II hypersensitivity reaction and is termed molecular mimicry.
Usually, self reactive B cells remain anergic in the periphery without T cell co-stimulation. During a Strep. infection activated antigen presenting cells such as macrophages present the bacterial antigen to helper T cells. Helper T cells subsequently activate B cells and induce the production of antibodies against the cell wall of Streptococcus. However the antibodies may also react against the myocardium and joints[5], producing the symptoms of Rheumatic fever.
Group A streptococcus pyogenes has a cell wall composed of branched polymers which sometimes contain "M proteins" that are highly antigenic. The antibodies which the immune system generates against the "M proteins" may cross react with cardiac myofiber sarcolemma and smooth muscle cells of arteries, inducing cytokine release and tissue destruction. This inflammation occurs through direct attachment of complement and Fc receptor-mediated recruitment of neutrophils and macrophages. Characteristic Aschoff bodies, composed of swollen eosinophilic collagen surrounded by lymphocytes and macrophages can be seen on light microscopy. The larger macrophages may become Aschoff giant cells. Acute rheumatic valvular lesions may also involve a cell-mediated immunity reaction as these lesions predominantly contain T-helper cells and macrophages.[6]
In acute RF, these lesions can be found in any layer of the heart and is hence called pancarditis. The inflammation may cause a serofibrinous pericardial exudates described as “bread-and-butter” pericarditis, which usually resolves without sequelae. Involvement of the endocardium typically results in fibrinoid necrosis and verrucae formation along the lines of closure of the left-sided heart valves. Warty projections arise from the deposition, while subendothelial lesions may induce irregular thickenings called MacCallum plaques.
Chronic rheumatic heart disease is characterized by repeated inflammation with fibrinous resolution. The cardinal anatomic changes of the valve include leaflet thickening, commissural fusion and shortening and thickening of the tendinous cords. RHD cause 99% of mitral stenosis often resulting in a “fish mouth” gross appearance.[7]
Treatment
The management of acute rheumatic fever is geared toward the reduction of inflammation with anti-inflammatory medications such as aspirin or corticosteroids. Individuals with positive cultures for strep throat should also be treated with antibiotics. Another important cornerstone in treating rheumatic fever includes the continuous use of low dose antibiotics (such as penicillin, sulfadiazine, or erythromycin) to prevent recurrence.
Infection
Patients with positive cultures for streptococcus pyogenes should be treated with penicillin as long as allergy is not present. This treatment will not alter the course of the acute disease.
Inflammation
Patients with significant symptoms may require corticosteroids. Salicylates are useful for pain.
Heart failure
Some patients develop significant carditis which manifests as congestive heart failure. This requires the usual treatment for heart failure: diuretics and digoxin. Unlike normal heart failure, rheumatic heart failure responds well to corticosteroids.
Prevention
Prevention of recurrence is achieved by eradicating the acute infection and prophylaxis with antibiotics. The American Heart Association recommends daily or monthly prophylaxis continue long-term, perhaps for life.[8]
Primary care physicians, nurses also have a role in prevention, primarily in screening school-aged children for sore throats that may be caused by Group A streptococci(especially Group A β Hemolytic Streptococcus pyogenes).
Pathological Findings
-

Aortic Stenosis (Tricuspid aorta): Gross, good example of aortic stenosis due to rheumatic fever
-
Gross, an excellent example of mitral scarring due to rheumatic fever (healing phase of an infectious lesion).
-
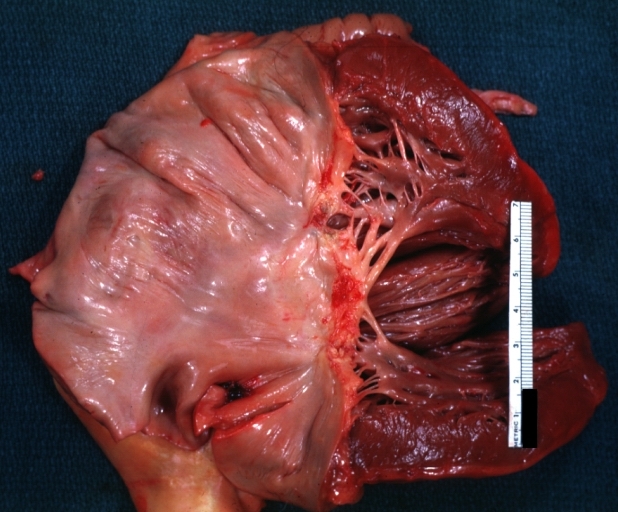
Rheumatic mitral valvulitis: Gross, an excellent example of fibrosis, chorda thickening and shortening has thrombus around the large left atrium



-
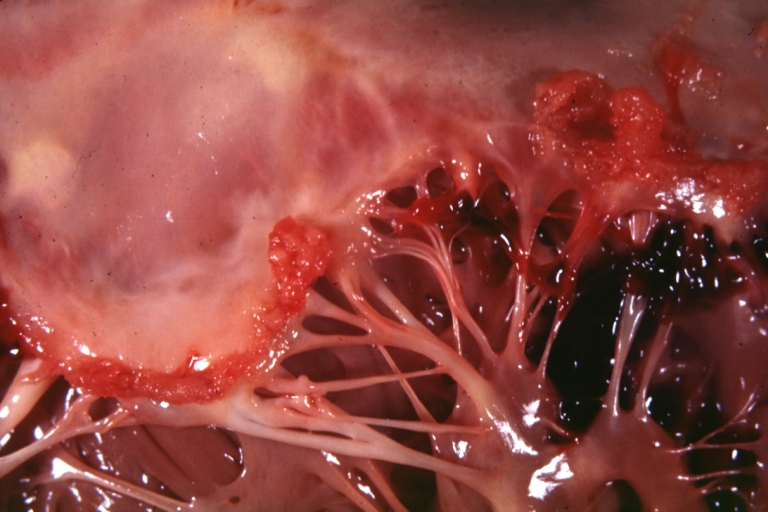
Mitral valve: acute rheumatic fever
-
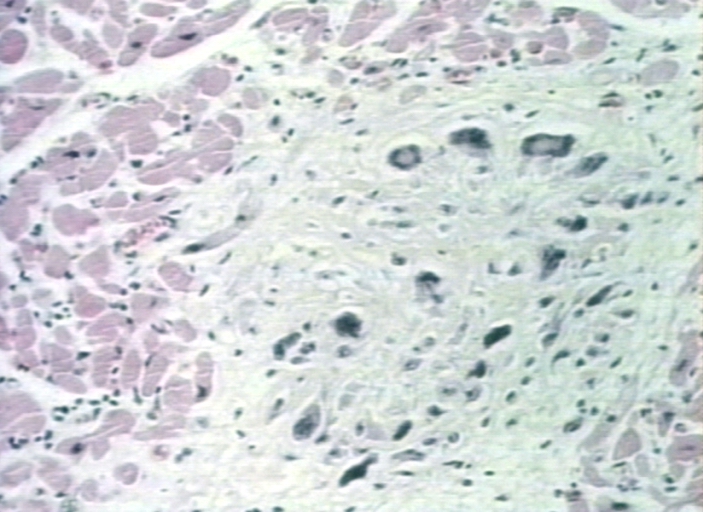
Aschoff bodies in rheumatic heart disease


References
- ↑ Jones TD. The diagnosis of rheumatic fever. JAMA. 1944; 126:481–484
- ↑ Ferrieri P. Proceedings of the Jones criteria workshop. Circulation 2002; 106: 2521–23
- ↑ Steven J Parrillo, DO, FACOEP, FACEP. "eMedicine — Rheumatic Fever".
- ↑ "Guidelines for the diagnosis of rheumatic fever. Jones Criteria, 1992 update. Special Writing Group of the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease of the Council on Cardiovascular Disease in the Young of the American Heart Association". JAMA. 268 (15): 2069–73. 1992. PMID 1404745.
- ↑ Abbas and Lechtman. mBasic Immunology: Functions and Disorders of the Immune System. Elsevier Inc. 2004.
- ↑ Kumar et al. Robbins and Cotran Pathologic Basis of Disease. Elsevier Inc. 2005
- ↑ "Robbins & Cotran Pathologic Basis of Disease".
- ↑ "Rheumatic Heart Disease/Rheumatic Fever". American Heart Association. Retrieved 2008-02-17.
External links
- Rheumatic fever information from Seattle Children's Hospital Heart Center
Template:Bacterial diseases Template:Hypersensitivity and autoimmune diseases Template:SIB
zh-min-nan:Hong-sip-jia̍t de:Rheumatisches Fieber it:Febbre reumatica nl:Acuut reuma sr:Реуматска грозница