Pulmonary hypertension pathophysiology: Difference between revisions
No edit summary |
No edit summary |
||
| Line 35: | Line 35: | ||
* Down regulation of the [[voltage-gated potassium channel]]s has also been linked with altered pulmonary vascular tone, dysregulation of cellular homeostasis, and induction of proliferative sequelae in vascular [[smooth muscle cell]]s. | * Down regulation of the [[voltage-gated potassium channel]]s has also been linked with altered pulmonary vascular tone, dysregulation of cellular homeostasis, and induction of proliferative sequelae in vascular [[smooth muscle cell]]s. | ||
3. '''''Proliferation-mediated remodeling''''' | 3. '''''Proliferation-mediated remodeling''''' | ||
* [[Serotonin]] exerts both vasoconstrictive and mitogenic effects on [[smooth muscle cell]]s (SMC). | |||
[[Serotonin]] exerts both vasoconstrictive and mitogenic effects on [[smooth muscle cell]]s (SMC). Serotonin may bind to 5-hydroxytryptamine 1A and 2B receptors or may enter SMC via [[SERT|serotonin transporter]] which induces generation of [[reactive oxygen species|ROS]], [[rho kinase]], and [[MAPK|mitogen-activated protein kinases]]. This in turn leads to the expression of [[growth factor]]s and proliferation. [[Bone morphogenetic protein|Bone morphogenetic protein (BMP)]] is also involved in the SMC proliferation. Upon binding of BMP to its heterodimerized receptors, a group of cytoplasmic proteins known as receptor-mediated [[Smad]]s are phosphorylated and translocated to the nucleus where they upregulate genes related to anti-proliferation. Serotonin is shown to antagonize the BMP/Smad pathway thus facilitating the proliferation of [[smooth muscle cell]]s. | * Serotonin may bind to 5-hydroxytryptamine 1A and 2B receptors or may enter SMC via [[SERT|serotonin transporter]] which induces generation of [[reactive oxygen species|ROS]], [[rho kinase]], and [[MAPK|mitogen-activated protein kinases]]. | ||
* This in turn leads to the expression of [[growth factor]]s and proliferation. [[Bone morphogenetic protein|Bone morphogenetic protein (BMP)]] is also involved in the SMC proliferation. | |||
* Upon binding of BMP to its heterodimerized receptors, a group of cytoplasmic proteins known as receptor-mediated [[Smad]]s are phosphorylated and translocated to the nucleus where they upregulate genes related to anti-proliferation. | |||
* Serotonin is shown to antagonize the BMP/Smad pathway thus facilitating the proliferation of [[smooth muscle cell]]s. | |||
4. '''''Inflammation-mediated remodeling''''' | 4. '''''Inflammation-mediated remodeling''''' | ||
| Line 44: | Line 46: | ||
Shown below is an image depicting remodeling in pulmonary arterial hypertension. | Shown below is an image depicting remodeling in pulmonary arterial hypertension. | ||
<figure-inline><figure-inline><figure-inline>[[File:Pathophysiology of pulmonary hypertension.png|661x661px]]</figure-inline></figure-inline></figure-inline> | <figure-inline><figure-inline><figure-inline><figure-inline>[[File:Pathophysiology of pulmonary hypertension.png|661x661px]]</figure-inline></figure-inline></figure-inline></figure-inline> | ||
===Genetic Mutations=== | ===Genetic Mutations=== | ||
Revision as of 19:58, 26 February 2018
|
Pulmonary Hypertension Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Pulmonary hypertension pathophysiology On the Web |
|
American Roentgen Ray Society Images of Pulmonary hypertension pathophysiology |
|
Risk calculators and risk factors for Pulmonary hypertension pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Assistant Editor(s)-in-Chief: Ralph Matar; Rim Halaby
Overview
Pulmonary hypertension (PH) is a pathological condition of the pulmonary vasculature present in several disease states and leading to hemodynamical derangement. PH is defined as an elevated mean pulmonary artery pressure (PAP) as measured by right heart catheterization at rest. The factors that are in involved in the pathophysiology of the increase in the mean pulmonary arterial pressure are: increase in pulmonary vascular resistance, increase in the right sided cardiac output and increase in the mean pulmonary venous pressure. To note that “Pulmonary arterial hypertension” (PAH) refers to group 1 PAH in the updated WHO classification. “Pulmonary hypertension” (PH) refers to any of group 2 PH through group 5 PH. PH is also used when referring to all five groups collectively.
Pathophysiology
PH is defined as an elevated mean pulmonary artery pressure (PAP) ≥ 25 mmHg as measured by right heart catheterization at rest. The elevation in PAP results from an elevation in the pulmonary vascular resistance caused by a multifactorial pathogenesis involving genetic and environmental factors.
Pulmonary hypertension has several pathophysiologic mechanisms depending on the underlying etiology. Nevertheless, the following sequence of events is almost always present:
- An initiating factor leads to increased resistance in the pulmonary vasculature causing narrowing of the vessels and impaired blood flow.
- As a consequence, the right ventricle adapts by increasing right ventricular systolic pressures to preserve the cardiac output from the right heart.
- Over time, increasing right ventricular systolic pressures will subsequently result in chronic changes in the pulmonary circulation and the affected blood vessels progressively become stiffer and thicker, further increasing the blood pressure within the lungs and impairing blood flow.
- In addition, the increased workload of the heart causes thickening and enlargement of the right ventricle, making the heart less able to pump blood through the lungs, causing right heart failure. Factors that might affect the ability of the right ventricle to adapt to an increased pulmonary vascular resistance are:
- Age of the patient at onset
- Rapidity of onset of pulmonary hypertension
- Coexisting hypoxemia
Pulmonary Arterial Hypertension
Molecular and Cellular Changes
Pulmonary arterial hypertension is characterized by endothelial dysfunction resulting from an imbalance between apoptosis and proliferation of pulmonary artery smooth muscle cells favoring the proliferation. There is also thickened and disordered adventitia due to excessive amounts of adventitial metalloproteinases. Several pathways are implicated in development of vascular remodeling, which is the hallmark of pathologic changes in pulmonary hypertension:
1. Thrombosis-mediated remodeling
- Thrombin plays a key role in mediating vascular remodeling by activating platelet, upregulating angiogenesis-related genes (including tissue factor [TF], basic fibroblast growth factor [bFGF], and matrix metalloproteinase-2), and transactivating vascular endothelial growth factor (VEGF) by inducing the production of reactive oxygen species (ROS) and the expression of the hypoxia inducible factor-1 alpha.
- Upregulation of TF in the vasculature leads to initiation of coagulation cascade and migration and proliferation of smooth muscle cells upon vascular injury.
- In addition, platelet activation by thrombin results in the release of granules containing substances that promote mitogenesis and vasoconstriction including VEGF, bFGF, platelet-derived growth factor, and serotonin, which also contribute to increased endothelial cell migration and proliferation.
2. Vasoconstriction-mediated remodeling
- Imbalance of vasoactive signals is suggested in the pathogenesis of remodeling.
- Reduced levels of vasodilatory mediators, in particular prostaglandin I2, nitric oxide, and cyclic guanine monophosphate, and elevated levels of vasocontricting molecules such as endothelin 1, thromboxane, and 5-hydroxytryptamine contribute to alterations in the vascular tone.
- Down regulation of the voltage-gated potassium channels has also been linked with altered pulmonary vascular tone, dysregulation of cellular homeostasis, and induction of proliferative sequelae in vascular smooth muscle cells.
3. Proliferation-mediated remodeling
- Serotonin exerts both vasoconstrictive and mitogenic effects on smooth muscle cells (SMC).
- Serotonin may bind to 5-hydroxytryptamine 1A and 2B receptors or may enter SMC via serotonin transporter which induces generation of ROS, rho kinase, and mitogen-activated protein kinases.
- This in turn leads to the expression of growth factors and proliferation. Bone morphogenetic protein (BMP) is also involved in the SMC proliferation.
- Upon binding of BMP to its heterodimerized receptors, a group of cytoplasmic proteins known as receptor-mediated Smads are phosphorylated and translocated to the nucleus where they upregulate genes related to anti-proliferation.
- Serotonin is shown to antagonize the BMP/Smad pathway thus facilitating the proliferation of smooth muscle cells.
4. Inflammation-mediated remodeling
Influx of inflammatory effector cells is stimulated by the release of chemokines such as CCL5 and CX3CL1. On the other hand, endothelial cell and smooth muscle cell dysfunction contributes to the release of vasomotor and growth factors, activation of transcription factors, influx of calcium, and dysfunction of mitochondria. The net effect is a shift of balance in favor of proliferation and suppressed apoptosis, leading to remodeling of the pulmonary vasculature.
Shown below is an image depicting remodeling in pulmonary arterial hypertension.
<figure-inline><figure-inline><figure-inline><figure-inline> </figure-inline></figure-inline></figure-inline></figure-inline>
</figure-inline></figure-inline></figure-inline></figure-inline>
Genetic Mutations
TGF-β Receptor Pathway
- Bone morphogenetic protein receptor II (BMPR2) gene encodes a serine/threonine kinase that functions as a receptor for bone morphogenetic proteins which forms a heterodimer cytoplasmic complex of two type II and two type I receptors. The downstream signaling involves activation of SMAD transcription factor which mediates anti-proliferation in smooth muscle cells.
- Activin-like kinase 1 gene mutations are detected in patients with hereditary hemorrhagic telangiectasia and pulmonary arterial hypertension. Mutation would cause growth-promoting alterations.
Serotoninergic Pathway
- 5- Hydroxytryptamine (serotonin) transporter mutations have also been associated with the proliferation of smooth muscle cells of pulmonary arteries.[1]
Histopathology
PH is a pathological condition present in different disease states that share similar clinical manifestation and some common histopathological features. Shown below is a table that summarizes the classification of PH based on histopathology findings.[2]
| Class | Histopathological findings[2] |
| Pulmonary arteriopathy | Constrictive lesions in pulmonary arteries
Complex lesions in pulmonary arteries
|
| Pulmonary arteriopathy with venous-venular changes | Changes similar to pulmonary arteriopathy PLUS Changes in venules and veins |
| Pulmonary occlusive venopathy (with or without arteriopathy) |
Changes in venules and veins
Changes in the capillaries
Changes in the interstitium |
| Pulmonary microvasculopathy (with or without arteriopathy and/on venopathy) |
Changes in the capillaries
Changes in the interstitium |
| Unclassified | Non specific changes |
Gallery
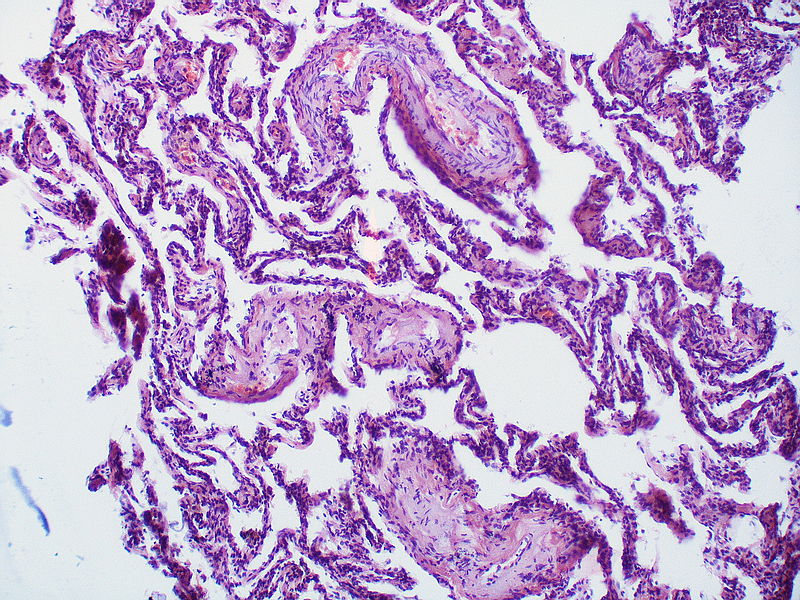
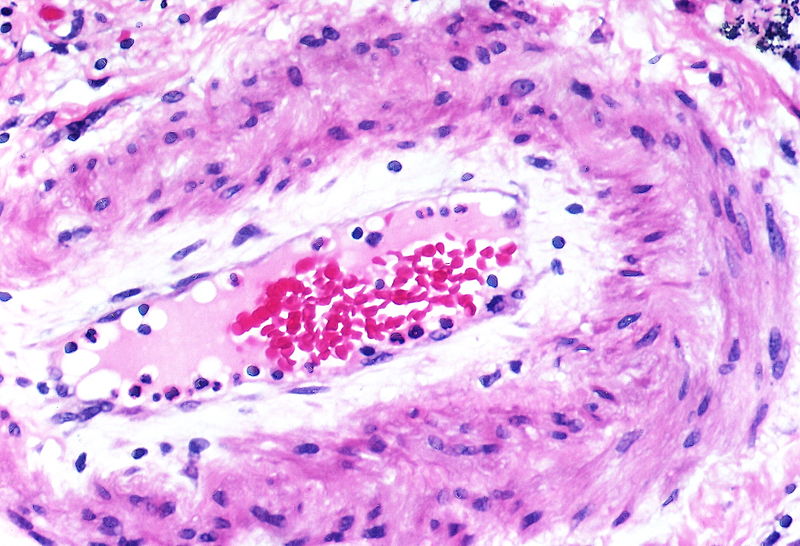
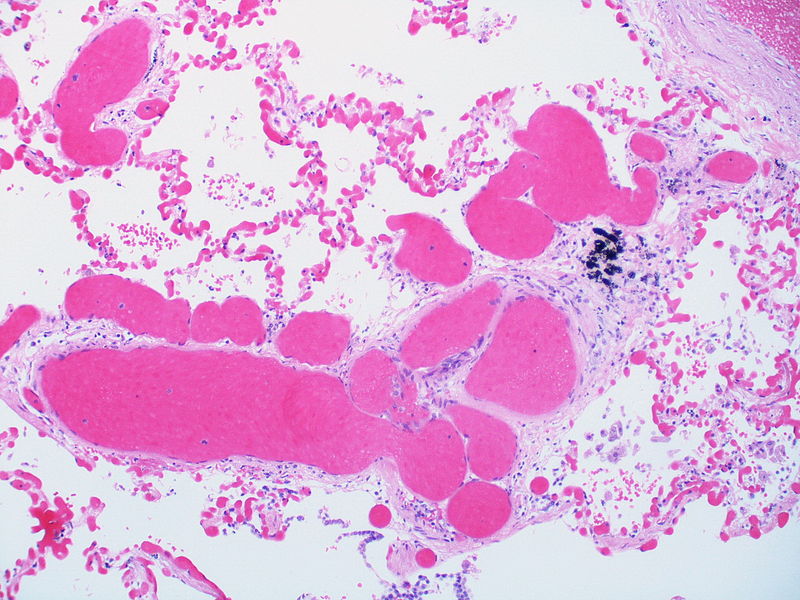
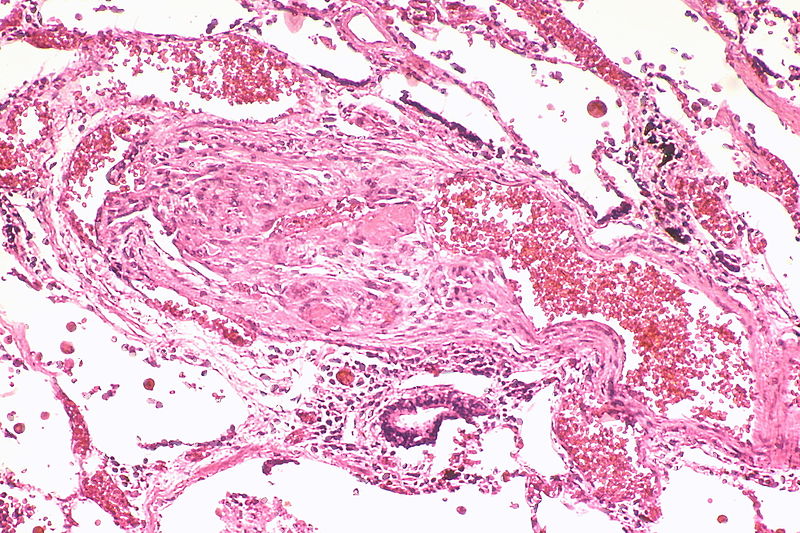
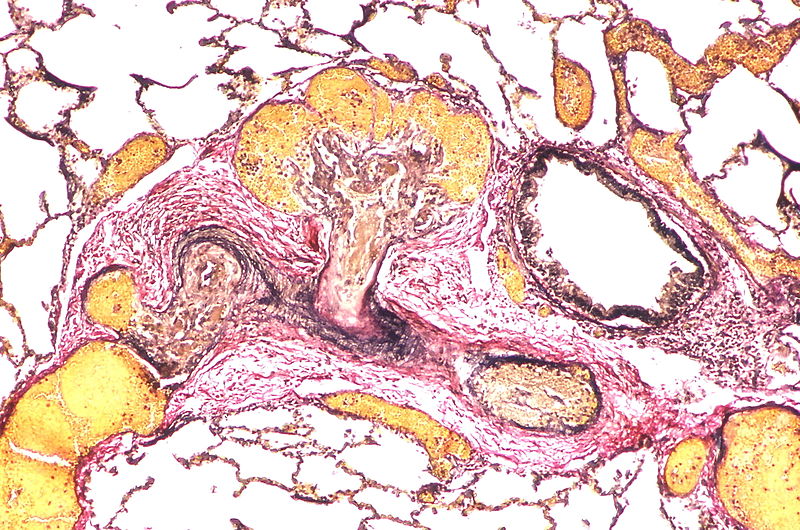
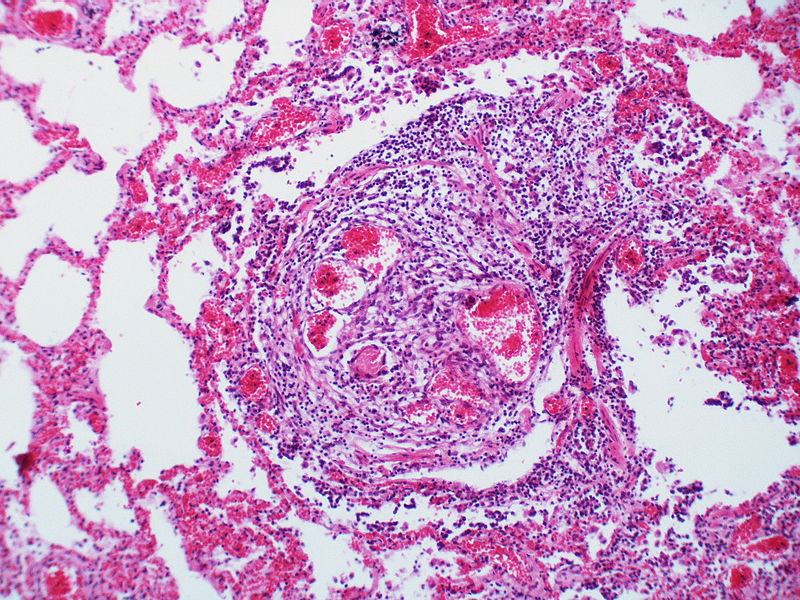
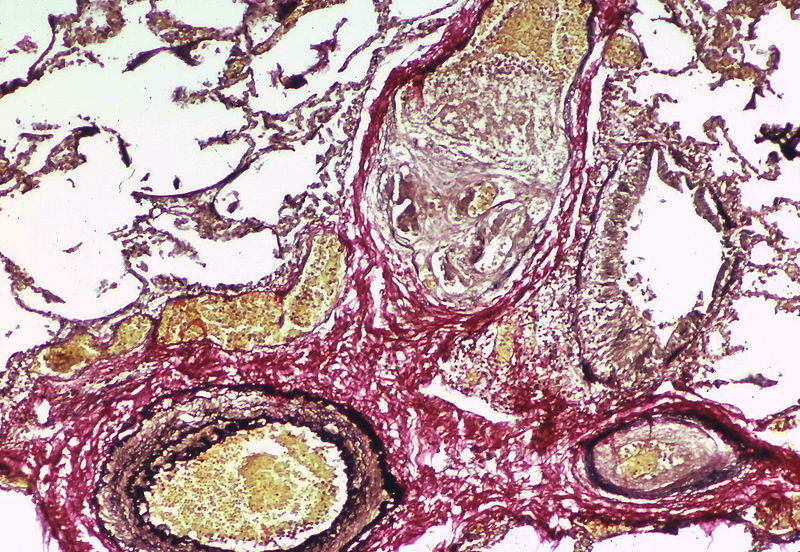
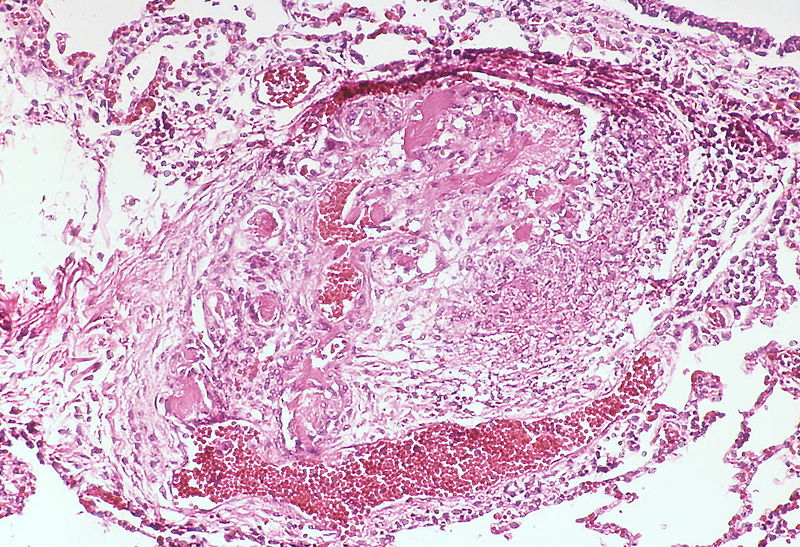
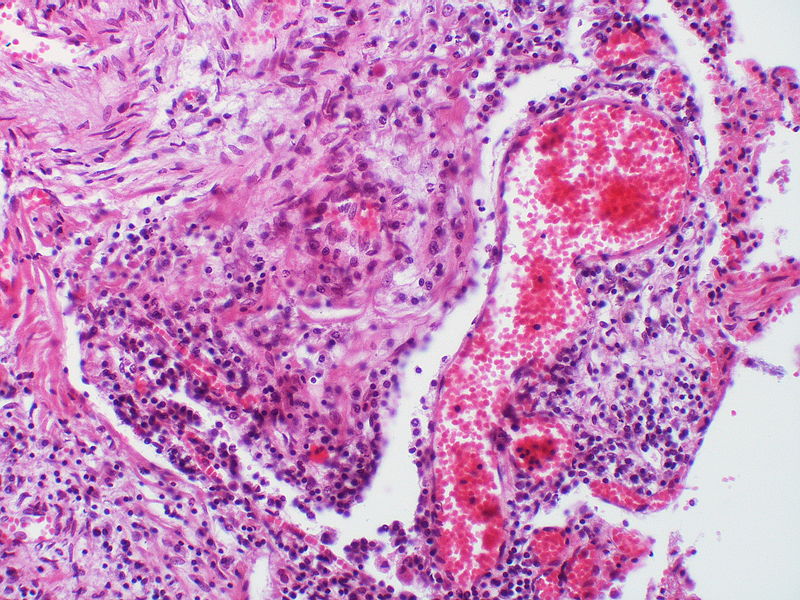
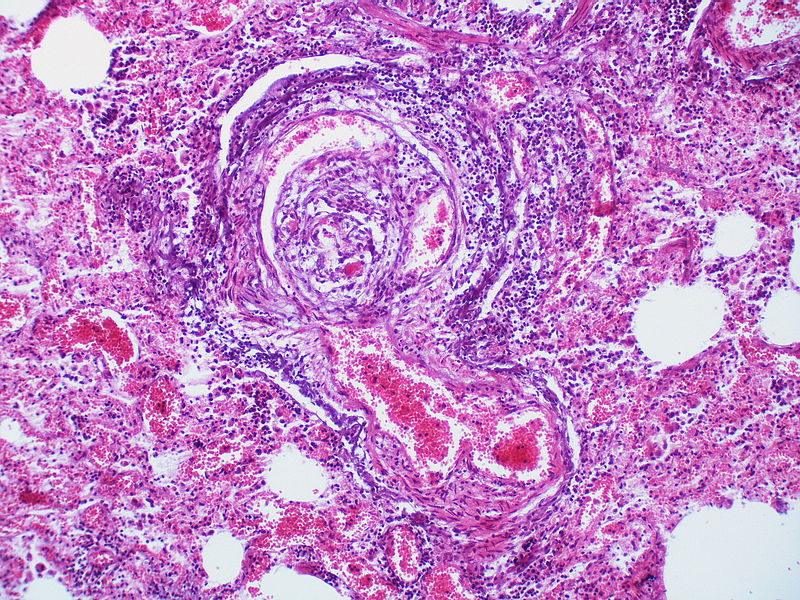
The images below are courtesy of Dr. Yale Rosen (Source:Wikimedia Commons).
-
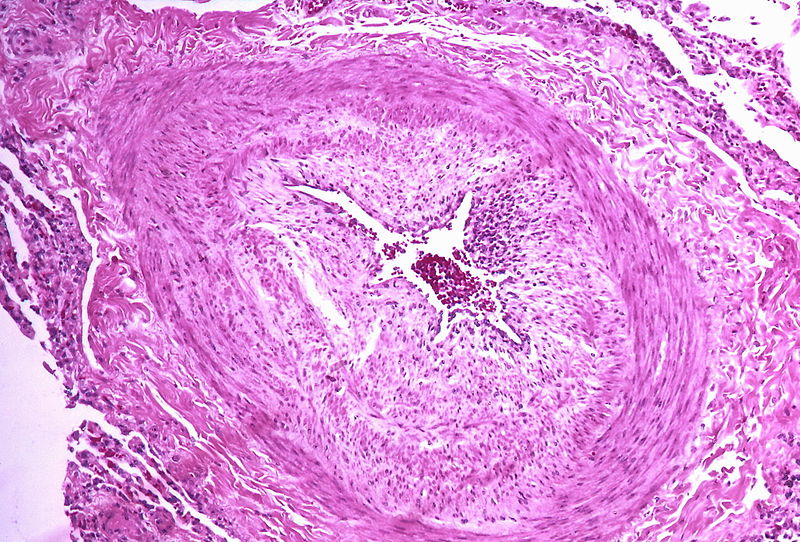
Marked intimal and medial thickening
-
Medial muscle layer thickening involving multiple pulmonary arteries.
-
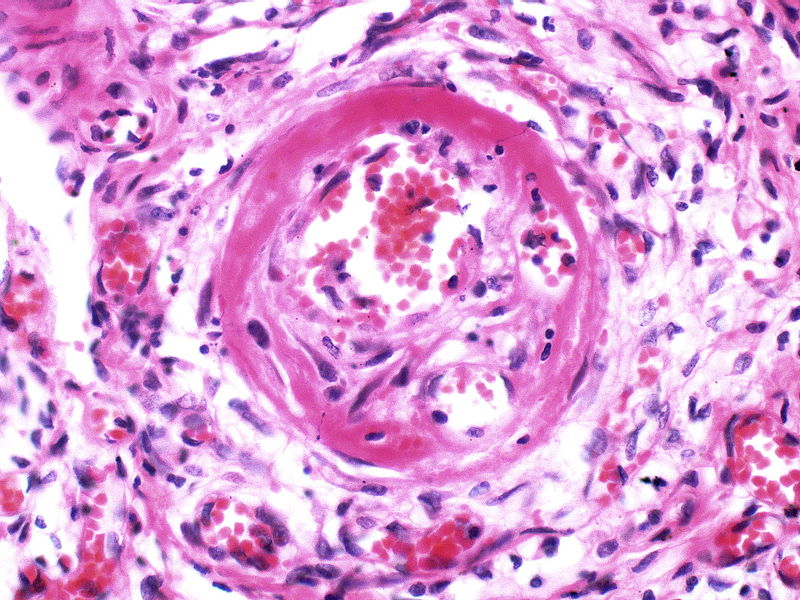
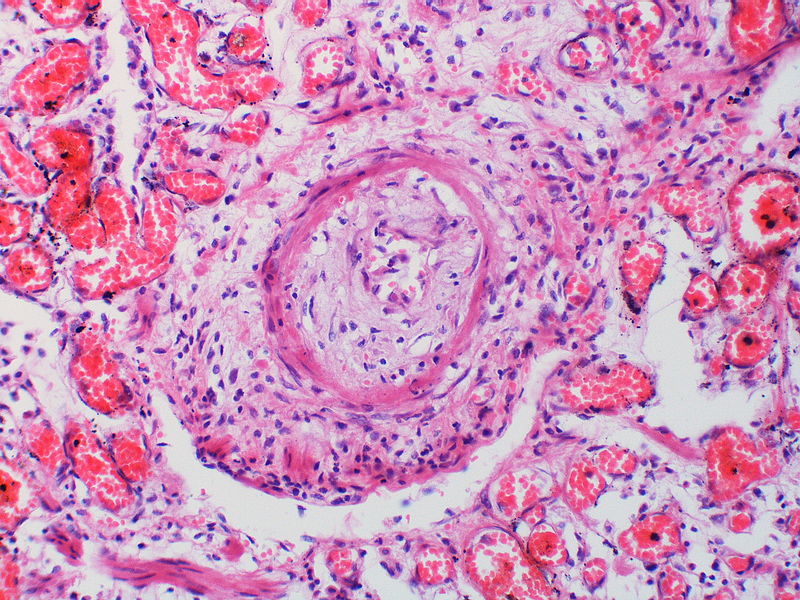
This arteriole exhibits fibrinoid necrosis
-
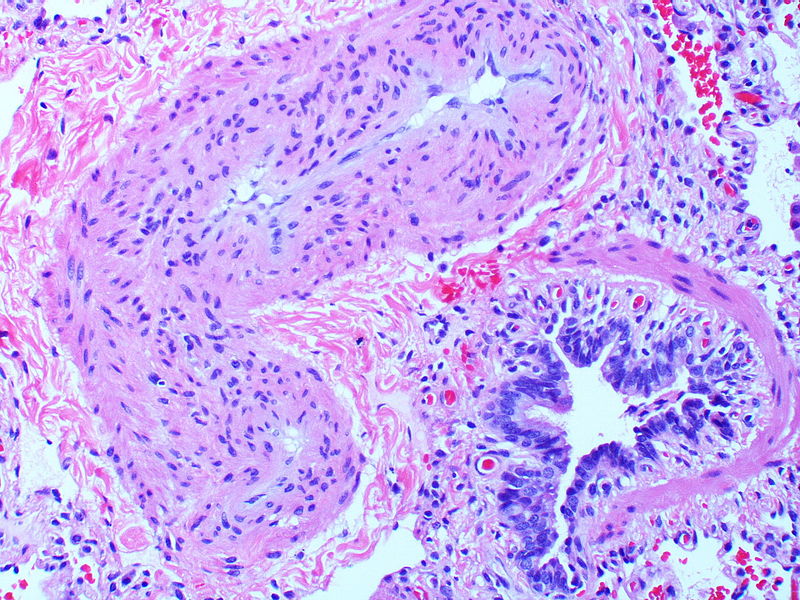
Pronounced thickening of the medial muscle layer.
-
Marked intimal and medical thickening.
-
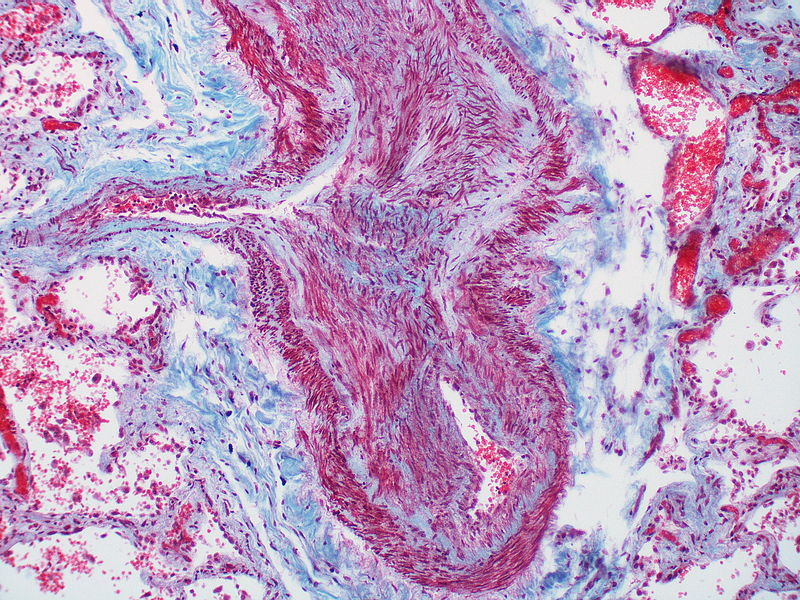
This artery exhibits marked intimal thickening The red-staining cells in the intima are probably myofibroblasts. Masson trichrome stain.
-
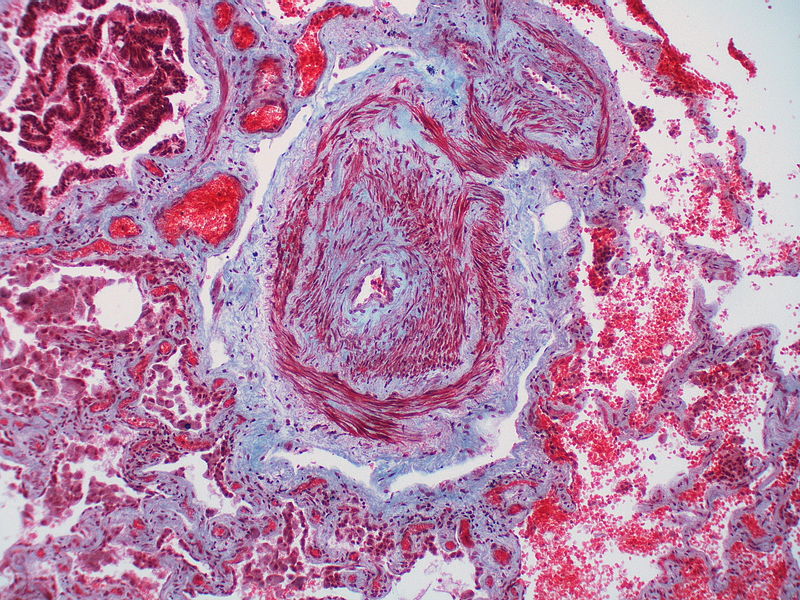
Marked adventitial thickening. Masson trichrome stain.
-
This artery exhibits marked intimal thickening as well as adventitial thickening. The red-staining cells in the intima are probably myofibroblasts. Masson trichrome stain.
-
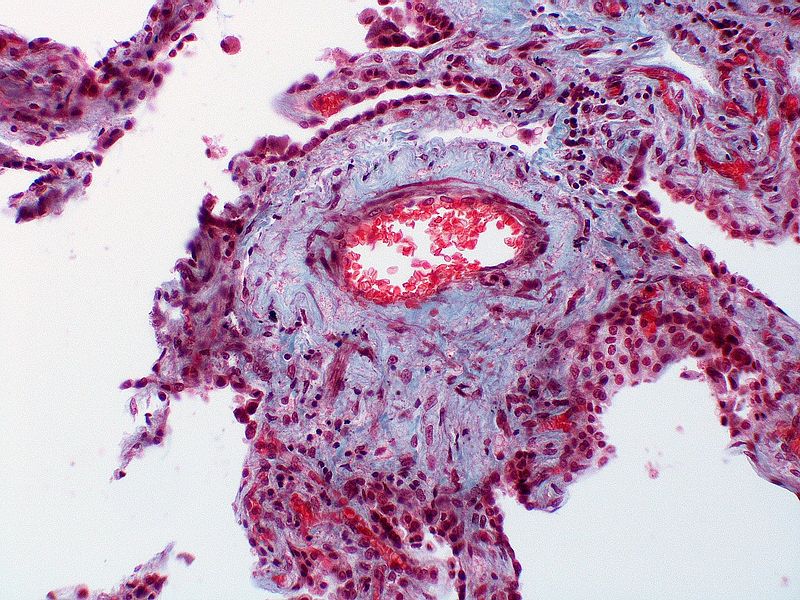
Pulmonary hypertension associated with pulmonary hemangiomatosis. A muscular pulmonary artery surrounded by angiomatous vessels exhibits marked intimal and adventitial thickening.
-
There is thickening of the medial muscle layer as well as mild intimal thickening.
-
Alveolar capillary proliferation as well as proliferation of larger blood vessels, probably venules.
-
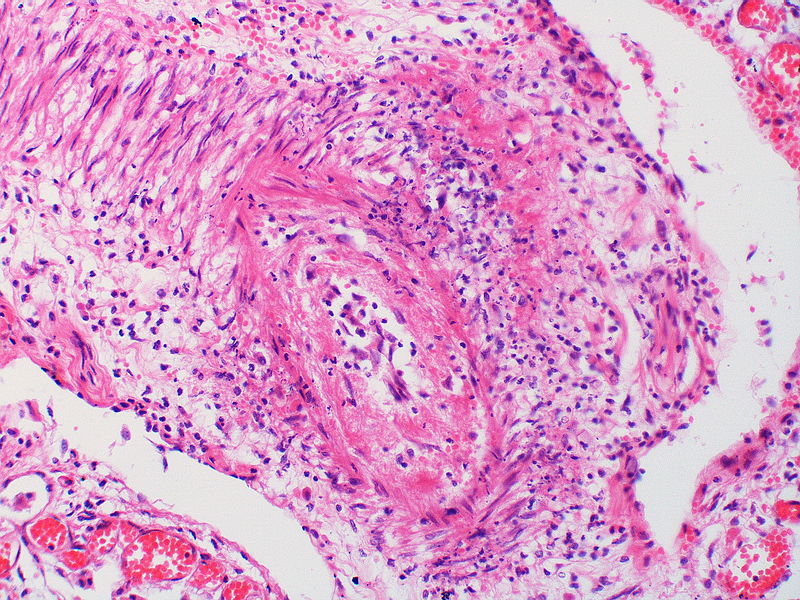
This artery exhibits vasculitis characterized by focal necrosis of the wall accompanied by inflammation.
-
A large dilatation lesion is present on the right side of this image adjacent to an angiomatoid lesion.
-
Two angiomatoid lesions are present. A large dilatation lesion is present adjacent to the angiomatoid lesion that is located just above center.
-

There is angiomatoid (plexiform) lesion.
-
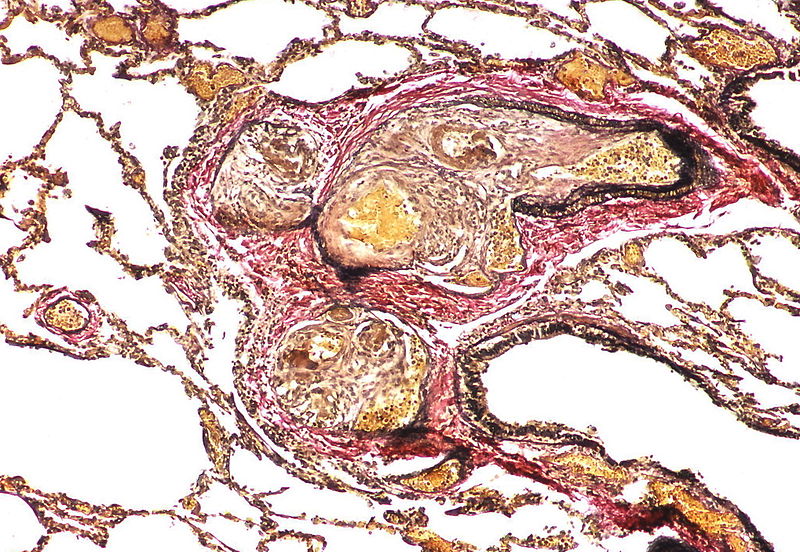
The appearance suggests multiple lesions but a single lesion cannot be excluded. Note the destruction of the arterial wall at the site of the angiomatoid lesion. Destructive arterial changes are frequently associated with angiomatoid lesions. There is elastic stain.
-
This angiomatoid lesion is accompanied by inflammation which is frequently associated with these lesions.
-
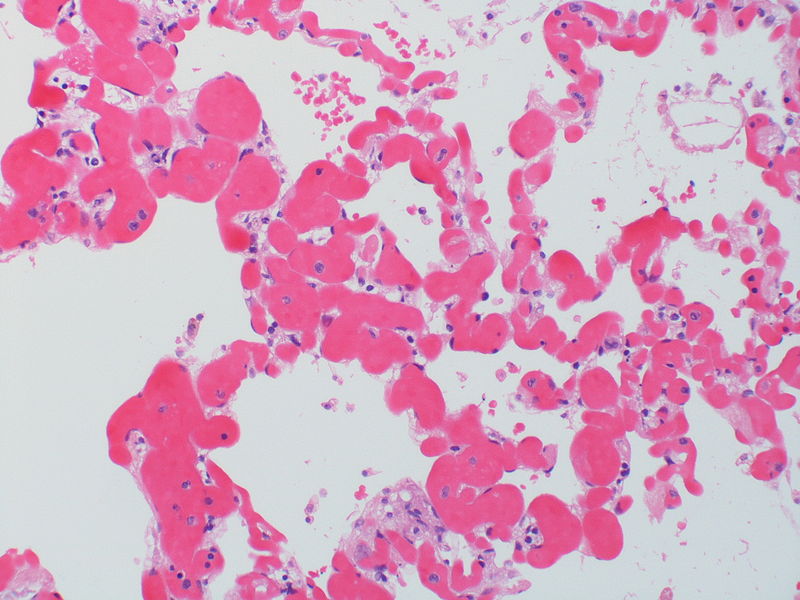
There is proliferation of alveolar wall capillaries which are markedly dilated.
-
A dilatation lesion is seen in the left lower quadrant adjacent to the angiomatoid lesion. There is an elastic stain.
-
This angiomatoid lesion contains multiple thrombi within the vascular spaces. A large dilatation lesion is present adjacent to the bottomof the angiomatoid lesion.
-
A dilatation lesion is present adjacent to the right side of the angiomatoid lesion.
-
There is disaappearance of the arterial wall at the site of the angiomatoid lesions. Arterial wall destruction is a frequent finding in association with angiomatoid lesions. A dilatation lesion encircles the angiomatoid lesion





















References
- ↑ Eddahibi S, Humbert M, Fadel E, Raffestin B, Darmon M, Capron F; et al. (2001). "Serotonin transporter overexpression is responsible for pulmonary artery smooth muscle hyperplasia in primary pulmonary hypertension". J Clin Invest. 108 (8): 1141–50. doi:10.1172/JCI12805. PMC 209526. PMID 11602621.
- ↑ 2.0 2.1 Pietra GG, Capron F, Stewart S, Leone O, Humbert M, Robbins IM; et al. (2004). "Pathologic assessment of vasculopathies in pulmonary hypertension". J Am Coll Cardiol. 43 (12 Suppl S): 25S–32S. doi:10.1016/j.jacc.2004.02.033. PMID 15194175.