Galeazzi fracture

|
WikiDoc Resources for Galeazzi fracture |
|
Articles |
|---|
|
Most recent articles on Galeazzi fracture Most cited articles on Galeazzi fracture |
|
Media |
|
Powerpoint slides on Galeazzi fracture |
|
Evidence Based Medicine |
|
Cochrane Collaboration on Galeazzi fracture |
|
Clinical Trials |
|
Ongoing Trials on Galeazzi fracture at Clinical Trials.gov Trial results on Galeazzi fracture Clinical Trials on Galeazzi fracture at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Galeazzi fracture NICE Guidance on Galeazzi fracture
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Galeazzi fracture Discussion groups on Galeazzi fracture Patient Handouts on Galeazzi fracture Directions to Hospitals Treating Galeazzi fracture Risk calculators and risk factors for Galeazzi fracture
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Galeazzi fracture |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Mohammadmain Rezazadehsaatlou[2].
Overview
The Galeazzi fracture-dislocation is an orthopedic injury pattern with the following definition:
- An isolated fractures of the distal 1/3 radius shaft
- Associated distal radioulnar joint (DRUJ) injury
Historical Perspective
In 1822, Sir Astley Cooper worked on the dislocations and Fracture of human body.
In 1934, Riccardo Galeazzi , an Italian surgeon at the Instituto de Rachitici in Milan, reported on his experience with 18 fractures with with close similarities to the Monteggia lesion.
In 1941, Campbell termed the Galeazzi fracture the "fracture of necessity".
In 1957, Hughston presented the definitive management of the Galeazzi fracture.
Causes
The main etiology of the Galeazzi fracture-dislocation is thought to be an axial loading may be placed on a hyperpronated forearm during falling onto an outstretched hand (FOOSH) with an extended wrist and hyperpronated forearm. Because at this posture the energy from the radius fracture transmitted towards the radioulnar joint cause the dislocation of the DRUJ.
Differentiating Galeazzi fracture-dislocation from other Diseases
Epidemiology and Demographics
Galeazzi fractures account for around 3-7% of all forearm fractures in adults. Normally, 25% of the radial shaft fractures are true Galeazzi type injuries. The most common risk factors for the Galeazzi fracture are: sports (football and wrestling), osteoporosis, and post-menopausal time; consequently, These risk factors cause the highest occurrence in young males (10:10,000) and elderly females (5:10,000). The peak incidence in children is the age of 9 to 12.
Risk Factors
There are different risk factors that presidpose patient for the Galeazzi fracture-dislocation that include::
- High-risk contact sports
- Higher age (elderly adults are higher prone to such fractures)
- Reduced bone density (osteoporosis)
- Direct blow
- Road / traffic accidents
- Falling
- Direct trauma to the arm/forearm
- Taking part in any rough or high-impact sport
- Street fights, gunshot wounds, and domestic violence, may also cause the Galeazzi fracture-dislocation
- Falling on an outstretched hand with the forearm pronated.
- Road traffic accidents.
- Athletic injuries.
- Gunshot wounds.
Screening
Osteoporosis is an important risk factor for human affecting human bone especially in men with the age of older than 50 years old and postmenopausal and women.
Based on the US Preventive Services Task Force (USPSTF) there are three groups of patients need to be screened for the osteoporosis:
- · Men with no history of osteoporosis
- · Women with the age of 65≤ year old, with no previous history of pathological fracture due to the osteoporosis
- · Women with the age of <65 years, with 10-year fracture risk of not less than a 65-year-old white woman (who has not any other risk factor)
Accordingly women older than age of 50 are the main target for the osteoporosis screening. There is no specific recommendation to screen men for the osteoporosis.[1]
The USPSTF recommendations from 2002 included:
Meanwhile, there are two major modalities for the osteoporosis screening:
- · Dual energy x-ray absorptiometry (DXA) of the hip and lumbar spine bones
- · Quantitative ultrasonography of the calcaneus
*It should be noted of the two above mentioned modalities for screening the ultrasonograhy is preferred to the DXA due to its lower cost, lower ionizing radiation, more availability.
After the primary evaluation of the osteoporosis, the further evaluation are required in some cases such as:
· Women with normal bone density or mild osteopenia: T-score of greater than −1.50 – should have screening for 15 years.
· Women with moderate osteopenia: T-score of −1.50 to −1.99 – should have screening for 5 years.
· Women with advanced osteopenia: T-score of −2.00 to −2.49 - should have screening for 1 year.
Natural History, Complications and Prognosis
Natural History
Complications
The overall complication rate in the treatment of Galeazzi fracture-dislocation were found in around 40% of cases:
- Neurovascular compromise: such as Ulna nerve damage
- Compartment syndrome
- Chronic disability of the DRUJ
- Physeal Injury
- Malunion of the radius
- Nonunion
- Infection
- Refracture following plate removal
- Posterior interosseois nerve (PIN) injury.
- Instability of the DRUJ
Prognosis
Successful treatment of Galeazzi fracture-dislocation depends on the on-time interventions such as: reduction of the radius and DRUJ and the restoration of the forearm axis. The incidence of nonunion of Galeazzi fracture-dislocation is very low. On the other hand, the rate of successful union following the open reduction of forearm fractures was reported around 98%. Previous researches showed that the loss of strength at the supination and pronation were found in 12.5% and 27.2%, respectively.
Diagnosis
The diagnosis of a Galeazzi fracture-dislocation should be confirmed using a radiographic examination.
Accordingly, the Walsh classification is based on the position of the radius:
Type I
- Dorsal displacement of the radius
- Caused by supination force
Type II
- Volar displacement of the radius
- Caused by pronation force
The two main views such as anteroposterior (AP) and lateral forearm are needed in this regard:
- Radial shaft fracture:
- Commonly found at the junction of the middle and distal third
- Dorsal/Volar angulation
- Radial shortening may occur
- Dislocation of the distal radioulnar joint
Meanwhile, the following mentioned findings on the obtained radiography (such as plain radiography and the bilateral axial computed tomography (CT)) are suggestive of injury to the distal radioulnar joint (DRUJ):
- The dislocated radius near to the injury site
- Shortened radius by more than 5 mm near to the injury site
- The ulnar styloid base fracture near to the injury site
- Widening of the DRUJ space near to the injury site
History and Symptoms
The related signs and symptoms include:
- Skin lacerations
- Weak pulse
- Open fractures
- Bruising
- Swelling
- Stiffness
- Inability to move
- Pain in touch
- Loss of function of the forearm
- Difficulties in detection of pulses
- Radial nerve damage
In the physical exam the orthopedic surgeon should check the vascular status and amount of swelling in the forearm. In MULTI-trauma patients or in comatose or obtunded patients a tense compartment with neurological signs or stretch pain should be considered as the compartment syndrome, and the compartment pressures should be measured and monitored. Normally the pain and soft-tissue swelling are found at the injury site (distal-third radial fracture site and at the wrist joint). This injury should be confirmed using a radiographic evaluations. Also, patients may loss the pinch mechanism between their thumb and their index finger which can be due to the paralysis of the flexor pollicis longus (FPL) and flexor digitorum profundus (FDP).
Physical Examination
The related signs and symptoms include:
- Edema of the forearm
- Most of the time the edema will be a non-pitting edema
- Depends on the edema extent, it may even lead to compartment syndrome in the anterior and internal compartment of forearm
- Bruising
- As a manifestation of internal injury to the local vessels by trauma or fractures bone
- Decrease in range of motion
- Movement of the fractures limb will be painful if possible at all
- Tenderness
- Deformity
- Fractured bone deformity may be touchable in the internal side of the forearm if the fracture is displaced
In the physical exam the orthopedic surgeon should check the vascular status and amount of swelling in the forearm. In polytrauma patients or in comatose or obtunded patients a tense compartment with neurological signs or stretch pain should be considered as the compartment syndrome, and the compartment pressures should be measured and monitored.
Physical examination of patients with Ulnar bone fracture is usually remarkable for swelling, tenderness, bruises, ecchymosis, deformity and restricted range of motion of the wrist.
Appearance of the Patient
- Patients with Ulnar bone fracture usually appears normal unless the patients had a high energy trauma causing the open wound fracture.
Vital Signs
- Weak pulse may be seen when associated with polytrauma.
- Low blood pressure with normal pulse pressure may be present due to compound fracture with blood loss.
Skin
- Skin examination of patients with Ulnar bone fracture includes:
HEENT
- HEENT examination of patients with Galeazzi fracture-dislocation is usually normal.
Neck
- Neck examination of patients with Galeazzi fracture-dislocation is usually normal
Lungs
- Pulmonary examination of patients with Galeazzi fracture-dislocation is usually normal
Heart
- Cardiovascular examination of patients with Galeazzi fracture-dislocation is usually normal
Abdomen
- Abdominal examination of patients with Galeazzi fracture-dislocation is usually normal
Back
- Back examination of patients with Galeazzi fracture-dislocation is usually normal
Genitourinary
- Genitourinary examination of patients with Galeazzi fracture-dislocation is usually normal
Neuromuscular
- Neuromuscular examination of patients with Galeazzi fracture-dislocation is usually normal
- However, some patients may develop neuropraxia of the branch of the Ulnar nerve resulting in decreased sensation of thumb, index and middle finger.
Laboratory Findings
There is a limited laboratory tests useful in the diagnosis of bone fractures such as the Galeazzi fracture-dislocation. Meanwhile, aged men and women may have some abnormalities in their laboratory findings suggestive of osteoporosis.
Laboratory tests for the diagnosis of osteoporosis are:
- Complete blood count (CBC)
- Serum total calcium level
- Serum Ionized calcium level
- Serum phosphate level
- Serum alkaline phosphatase level
- Serum 25-(OH)-vitamin D level
X Ray
The orthopedic surgeon should consider to have at least two radiographic projections (ie, anteroposterior [AP] and lateral) of the forearm. These show the fracture, the extent of displacement, and the extent of comminution. The orthopedic surgeon should pay serious attention toward finding any foreign bodies in open fractures and gunshot injuries. Also imperative is to include the elbow and wrist joint in the radiographs of ulnar fractures to ensure that the distal radioulnar joint injuries are not missed.
-

Lateral- Type 1 Galeazzi fracture
-
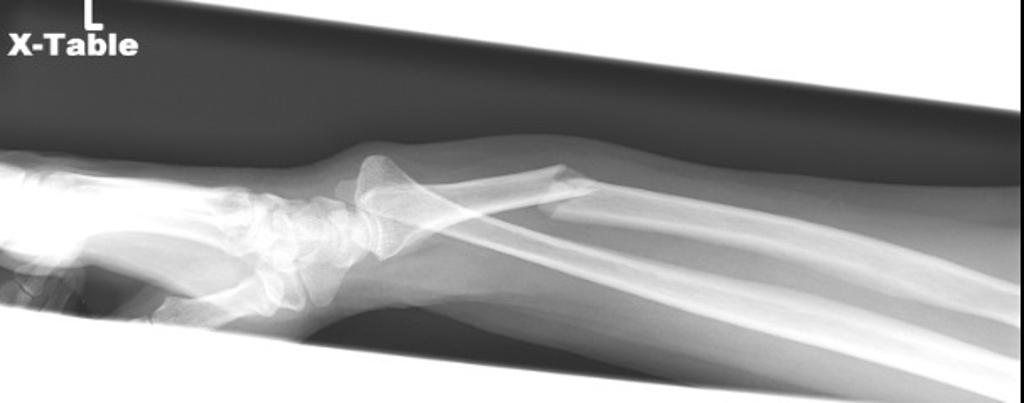
Lateral- Type 1 Galeazzi fracture
-

PA- Type 1 Galeazzi fracture
-

PA- Type 1 Galeazzi fracture

.jpg)
CT
- CT-scan in the case of the Galeazzi fracture-dislocation is the best modality if you can not have an exclusive diagnosis by X-ray itself can not be made.
MRI
- Magnetic resonance imaging (MRI) is an expensive technique that should not be used routinely.
- MRI is a powerful diagnostic tool to assess the abnormalities of the bone, ligaments and soft tissues associated with the Galeazzi fracture-dislocation, but it is known as a limited utility in radioulnar injuries and is not indicated in uncomplicated forearm fractures.
- Meanwhile, the MRI can be useful in in following mentioned evaluations:
- Evaluation of occult fractures
- Evaluation of the post-traumatic or avascular necrosis of carpal bones
- Evaluation of tendons
- Evaluation of nerve
- Evaluation of carpal tunnel syndrome
Other Imaging Findings
There are no other imaging findings associated with Galeazzi fracture-dislocation
Other Diagnostic Studies
There are no other Diagnostic studies associated with Galeazzi fracture-dislocation
Treatment
Immediate stabilization of patients is the first step. Then the radial fracture and the DRUJ stabilization is recommended in these cases. Open forearm fractures considered as a surgical emergency. Galeazzi fractures occurs in younger patients who are skeletally immature; the normally they treated using a closed reduction and casting. Since closed reduction and cast application have led to unsatisfactory results. Then, Almost always the open reduction are necessary for the Galeazzi fractures. There are controversies regarding the indications for intramedullary nailing of forearm fractures.
Non-Operative Treatment
- The first step in managing a patient with a fracture is to stabilize the patient if he/she is unstable due to blood loss, etc by giving them intravenous fluids and giving them some painkillers if the pain is severe.
- In children, the usual plan is to attempt closed reduction followed by cast immobilization. In adults, treatment with immobilization in a molded long arm cast can be used in those rare occasions of a non-displaced fracture of both bones of the forearm. If the fracture shifts in position, it may require surgery to put the bones back together.
- Rigid immobilization is suggested in preference to removable splints in nonoperative treatment for the management of the Galeazzi fracture-dislocation
- For all patients with Galeazzi fracture-dislocation, a post-reduction true lateral radiograph is suggested .
- Operative fixation is suggested in preference to cast fixation for fractures with post-reduction radial shortening greater than 3 mm, dorsal tilt greater than 10º, or intra-articular displacement or step-off greater than 2 mm.
- Patients probably do not need to begin early wrist motion routinely after stable fracture fixation.
- Adjuvant treatment of Galeazzi fracture-dislocation with vitamin C is suggested for the prevention of disproportionate pain
Complications of Non-surgical therapy
Failure of non-surgical therapy is common:
- Re-displacement to its original position even in a cast
- Stiffness
- Post traumatic osteoarthritis leading to wrist pain and loss of function
- Other risks specific to cast treatment include:
- Compression of the swollen arm causing compartment syndrome or carpal tunnel syndrome
- Reflex sympathetic dystrophy is a serious complication
- Stiffness is universal following a prolonged period of immobilization and swelling
Surgery
Returning to the normal physical activity after Galeazzi fracture-dislocation can take weeks to months of therapy under supervision an orthopedist. Meanwhile, a physiotherapy can be helpful for patient to achieve the normal wrist and elbow function caused by the immobilisation. All adult Galeazzi fractures should be considered to be treated with open reduction and internal fixation (ORIF).
-

PA- Type 1 Galeazzi fracture
Operation
- There are a variety of methods and implants useful to stabilize the Galeazzi fracture-dislocation, ranging from closed reduction and percutaneous pin fixation to the use of intra-medullary devices.
- However, the most common fixation methods to treat complex Galeazzi fracture-dislocation include external fixation, and open reduction and internal fixation.
External Fixation With or Without Percutaneous Pin Fixation
- Wrist spanning external fixation employs ligamentotaxis to restore and maintain length, alignment, and rotation of ulnar bone.
- Reduction is typically obtained through closed or minimally open methods and preserves the fracture biology.
- The addition of percutaneous pins enhances the ability to reduce and stabilize fracture fragments.
Complications of External Fixation
- Pin tract infection
- Injury to the superficial branch of the nerve
- Complex regional pain syndrome
Open reduction and internal fixation with plates and screws
- This is the most common type of surgical repair for Galeazzi fracture-dislocation
- During this type of procedure, the bone fragments are first repositioned (reduced) into their normal alignment.
- The bones held together with special screws and metal plates attached to the outer surface of the bone.
Complications of open reduction and internal fixation with plates and screws
- Infection
- Damage to nerves and blood vessels
- Synostosis
- Nonunion
Pain Management
Pain after an injury or surgery is a natural part of the healing process.
Medications are often prescribed for short-term pain relief after surgery or an injurysuch as:
- opioids
- non-steroidal anti-inflammatory drugs (NSAIDs)
- local anesthetics
Be aware that although opioids help relieve pain after surgery or an injury, they are a narcotic and can be addictive. It is important to use opioids only as directed by doctor.
Interventions
The following options can be helpful for patients to rehabilitate after their fracture :
- Joints mobilization
- compression bandage
- Soft tissue massage
- Exercises and Activity modification
- Forearm taping
- Forearm bracing
Postoperative Rehabilitation
- Complex Galeazzi fracture-dislocation warrant individualized immobilization and rehabilitation strategies.
- Similarly, the addition of a thumb spica cast or orthosis with positioning of the wrist in slight ulnar deviation for management of a comminuted radial column fracture may prevent loss of reduction. *Because most multifragmentary Galeazzi fracture-dislocation are the result of high-energy injuries, a prolonged period of wrist immobilization and soft-tissue rest may be beneficial and has not been shown to affect clinical outcomes.
- The wrist is typically immobilized for 2 weeks post-operatively in a sugar tong splint with neutral forearm rotation.
- At 6 weeks post-operatively, the wrist is placed into a removable orthosis, and active and passive range of motion (ROM) is initiated.
- Full weight bearing commences at approximately 3 months post-operatively after consolidation of the fracture is noted on radiographs.
- The presence of varying degrees of hand, wrist, and elbow stiffness is inevitable and may result from poor pain control, lack of effort in controlled mobilization, edema, concomitant ipsilateral upper extremity fractures, or peripheral nerve injuries.
- Early stretching and mobilization of the intrinsic and extrinsic tendons of the hand is important to prevent finger stiffness.
- Edema control can be initiated with compression gloves, digital massage, and active and passive ROM of the hand.
- A home exercise program or outpatient occupational therapy is started immediately post-operatively to maintain full range of motion of the hand and limit the development of intrinsic muscle tightness
Primary Prevention
There are various preventive options to reduce the incidence of the Galeazzi fracture-dislocation
- Using forearm and wrist guards during practicing sports (skating, biking)
- Using forearm and wrist guards during driving motorbikes
- Avoid falls in elderly individuals
- Prevention and/or treatment of osteoporosis
- Healthy diet
Secondary Prevention
It should be noted that the Post-menopausal women specially older than the age of 65 are at the higher risk of osteoporosis consequently these type of patients at greater risk for the pathological fractures .
So the Calcium and vitamin D supplementation play important role in increasing the bone mineral density (BMD) consequently decrease the risk of fracture in these type of patients. Also, avoiding excessive alcohol and quitting smoking play important role in this regard.
Detecting osteoporosis:
- DEXA(dual-energy x-ray absorptiometry) scan
- Serum calcium and vitamin D levels
- Ultrasonography of the calcaneus
Pharmacological therapy
- The primary goal for the treatment of osteoporosis is to reduce longtime fracture risk in patients. Increasing bone mineral density (BMD) in response to the treatment is far less important than improvement of clinical aspects of osteoporosis, i.e., osteoporoticfracture. Therefore, most of the drugs efficacy is measured by the extent they improve the fracture risk instead of increasing BMD.
- During the treatment, if a single fracture happens, it does not necessarily indicate treatment failure or the need to be started on an alternative treatment or patient referral to a specialist.
- Calcium and vitamin D supplementation have been found to be effective in reducing the long term fracture risk, significantly. In order to suggest the people to use vitamin D and calcium supplements, the physician needs to make sure that patient is not able to obtain the nutrients through the daily intake. The available supplemental ions of calcium include calcium carbonate, calcium citrate, and vitamin D3 in various dosage forms.
Life style modifications
- Exercise: Exercise promotes the mineralization of bone and bone accumulation particularly during growth. High impact exercise, in particular, has been shown to prevent the development of osteoporosis. However, it can have a negative effect on bone mineralization in cases of poor nutrition, such as anorexia nervosa and celiac disease.
- Nutrition: A diet high in calcium and vitamin D prevents bone loss. Patients at risk for osteoporosis, such as persons with chronic steroid use are generally treated with vitamin D and calcium supplementation. In renal disease, more active forms of vitamin D, such as 1,25-dihydroxycholecalciferol or calcitriol are used; as the kidney cannot adequately generate calcitriol from calcidiol (25-hydroxycholecalciferol), which is the storage form of vitamin D.
- By quitting smoking, osteoporosis as well as other diseases can be prevented.
- Avoiding excessive alcohol intake or drinking only in moderation (1–2 alcoholic beverages/day).
- Taking least possible dosages of certain medications that are associated with osteoporosis (anticonvulsants or corticosteroids).