C-reactive protein: Difference between revisions
No edit summary |
|||
| Line 151: | Line 151: | ||
|-bgcolor="LightSteelBlue" | |-bgcolor="LightSteelBlue" | ||
| '''Genetic''' | | '''Genetic''' | ||
|bgcolor="Beige"| | |bgcolor="Beige"| [[Allan-Herndon-Dudley syndrome]],[[Alport syndrome]],[[Andersen-Tawil syndrome]],[[ASPM (Genetics)]],[[Ataxia Telangiectasia]],[[Atransferrinemia]],[[Bloom syndrome]],[[Cardiofaciocutaneous syndrome]],[[Chronic granulomatous disease]],[[Congenital Adrenal Hyperplasia]],[[Congenital muscular dystrophy]],[[Cystic Fibrosis]],[[Down syndrome]],[[Dubin-Johnson syndrome]],[[Familial Mediterranean fever]],[[Friedreich's ataxia]],[[Myotonia congenita]],[[Myotonic dystrophy]],[[Neurofibromatosis]],[[Niemann-Pick disease]],[[Noonan syndrome]],[[Osteogenesis imperfecta]],[[Otospondylomegaepiphyseal dysplasia]],[[Pachyonychia congenita]],[[Pendred syndrome]],[[Polycystic kidney disease]],[[Primary biliary cirrhosis]],[[Primary ciliary dyskinesia]],[[Pseudoxanthoma elasticum]],[[Rett syndrome]],[[Rubinstein-Taybi syndrome]],[[Salla disease]],[[Sickle-cell disease]],[[Stargardt's disease]],[[Tay-Sachs Disease]],[[Treacher Collins syndrome]],[[Usher syndrome]],[[Vitelliform macular dystrophy]],[[Von Hippel-Lindau disease]],,[[Von Willebrand disease]],[[Waldenström macroglobulinemia]],[[Walker-Warburg syndrome]],[[Werner syndrome]],[[Williams syndrome]],[[Wiskott-Aldrich syndrome]],[[Wolfram syndrome]],[[X-linked adrenal hypoplasia congenita]],[[X-linked alpha thalassemia mental retardation syndrome]],[[X-linked congenital stationary night blindness]],[[ZAP70 deficiency]],[[Norrie disease]] | ||
|- | |- | ||
|-bgcolor="LightSteelBlue" | |-bgcolor="LightSteelBlue" | ||
Revision as of 03:41, 14 June 2012
| C-reactive protein, pentraxin-related | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
 | |||||||||||
| Identifiers | |||||||||||
| Symbols | CRP ; MGC149895; MGC88244; PTX1 | ||||||||||
| External IDs | Template:OMIM5 Template:MGI HomoloGene: 476 | ||||||||||
| |||||||||||
| RNA expression pattern | |||||||||||
 | |||||||||||
 | |||||||||||
| More reference expression data | |||||||||||
| Orthologs | |||||||||||
| Template:GNF Ortholog box | |||||||||||
| Species | Human | Mouse | |||||||||
| Entrez | n/a | n/a | |||||||||
| Ensembl | n/a | n/a | |||||||||
| UniProt | n/a | n/a | |||||||||
| RefSeq (mRNA) | n/a | n/a | |||||||||
| RefSeq (protein) | n/a | n/a | |||||||||
| Location (UCSC) | n/a | n/a | |||||||||
| PubMed search | n/a | n/a | |||||||||
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [3]
Overview
C-reactive protein (CRP) is a plasma protein, an acute phase protein produced by the liver. It is a member of the pentraxin family of proteins. It should not be confused with C-peptide or Protein C.
C-reactive protein (CRP) is an inflammatory marker with a very large body of evidence demonstrating its prognostic utility in apparently healthy patients, as well as patients with acute coronary syndromes. Pre-angioplasty levels of CRP predict outcome, CRP levels rise after angioplasty, and it appears that the rise can be blunted by GP IIb/IIIa inhibitors.
History and nomenclature
C-reactive protein was originally discovered by Tillett and Francis in 1930 as a substance in the serum of patients with acute inflammation that reacted with the C polysaccharide of pneumococcus.[1] Initially it was thought that CRP might be a pathogenic secretion, as it was elevated in people with a variety of illnesses, including carcinomas. Discovery of hepatic synthesis and secretion of CRP closed that debate
Genetics and biochemistry
The CRP gene is located on the first chromosome (1q21-q23). CRP is a 224 residue protein[2] with a monomer molar mass of 25106 Da. The protein is an annular pentameric disc in shape. Proteins with this type of configuration are known as pentraxins. Native CRP is a bit different as it has 10-subunits making two pentameric discs, with an overall molecular mass of 251060 Da.
Pathophysiology
In the field of atherosclerosis, it is unclear if CRP plays a putative role in disease or is a marker of ongoing disease.
- C-reactive protein (CRP) is an acute phase protein formed in the liver. The stimulus for CRP production is IL-6.
- CRP rises more than 6 hours after triggering stimulus
- Upon resolution of condition, CRP rapidly declines
- CRP is considered to be a better indicator for an inflammatory response because of its shorter half-life and rapid increase
Function
CRP is a member of the class of acute phase reactants as its levels rise dramatically during inflammatory processes occurring in the body. This increment is due to a rise in the plasma concentration of IL-6, which is produced by macrophages, endothelial cells and T-cells as well as adipocytes. CRP binds to phosphorylcholine on microbes. It is thought to assist in complement binding to foreign and damaged cells and enhances phagocytosis by macrophages, which express a receptor for CRP. It is also believed to play an important role in innate immunity, as an early defense system against infections.
Diagnostic use
CRP is used mainly as a marker of inflammation. Measuring and charting C-reactive protein values can prove useful in determining disease progress or the effectiveness of treatments. Blood, usually collected in a serum-separating tube, is analysed in a medical laboratory or at the point of testing.
Various analytical methods are available for CRP determination, such as ELISA, immunoturbidimetry, rapid immunodiffusion and visual agglutination.
Viral infections tend to give a lower CRP level than bacterial infection.
Cardiology diagnostic test
Arterial damage is thought to result from inflammation due to chemical insults. CRP is a general marker for inflammation and infection, so it can be used as a very rough proxy for heart disease risk. Since many things can cause elevated CRP, this is not a very specific prognostic indicator. Also, these values refer only to prolonged elevation, so a single measurement would be meaningless.
C-reactive protein blood test[3]
- Low risk: <1mg/L
- High risk: >3mg/L
Differential Diagnosis
Increased
- Acute pancreatitis
- Bacteria
- Bechterew's Disease
- Degenerative joint diseases
- Dermatomyositis
- Fungi
- Inflammatory Bowel Disease
- Juvenile Arthritis
- Leukemia
- Malignant tumors
- Myocardial Infarction
- Parasites
- Polymyalgia Rheumatica
- Polymyositis
- Postoperatively
- Post Percutaneous Coronary Intervention (PCI)
- Pseudogout
- Psoriasis arthropathy
- Reiter's Syndrome
- Rheumatoid Arthritis
- Sjogren's Syndrome
- Systemic Lupus Erythematosus
- Vasculitis
- Viruses
- Wegener's Granulomatosis
Complete Differential Diagnosis of the Causes of ...
(By organ system)
Role in cardiovascular disease
Recent research suggests that patients with elevated basal levels of CRP are at an increased risk for diabetes,[4][5] hypertension and cardiovascular disease. A study of over 700 nurses showed that those in the highest quartile of trans fat consumption had blood levels of C-reactive protein (CRP, a pro-inflammatory cytokine which is a cardiovascular disease risk factor) that were 73% higher than those in the lowest quartile.[6] Although one group of researchers indicated that CRP may only be a moderate risk factor for cardiovascular disease,[7] this study (known as the Reykjavik Study) was found to have some problems for this type of analysis related to the characteristics of the population studied, and there was an extremely long follow-up time which may have attenuated the association between CRP and future outcomes.[8] Others have shown that CRP can exacerbate ischemic necrosis in a complement-dependent fashion and that CRP inhibition can be a safe and effective therapy for myocardial and cerebral infarcts.[9]
To measure the CRP level, a "high-sensitivity" CRP or hs-CRP test needs to be performed and analyzed by a laboratory. This is an automated blood test designed for greater accuracy in measuring low levels of CRP, which allows the physician to assess cardiovascular risk. If a result in the low-risk range is found ( < 1 mg/L), it does not need repeating. Higher levels need repeating, and clinical evaluation as necessary.
Role in colon cancer
The role of inflammation in cancer is not well known. Some organs of the body show greater risk of cancer when they are chronically inflamed.
Blood samples of persons with colon cancer have an average CRP concentration of 2.69 milligrams per liter. Persons without colon cancer average 1.97 milligrams per liter. The difference was statistically significant.[10] These findings concur with previous studies that indicate that anti-inflammatory drugs could lower colon cancer risk.[11]
Related chapters
Additional images
-
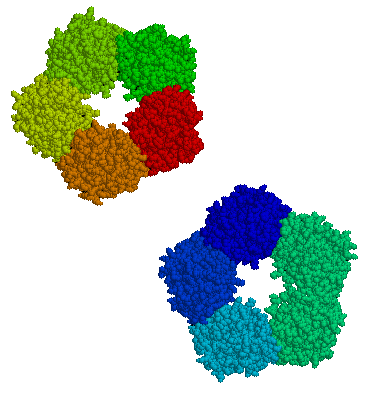
C-reactive protein

References
- ↑ Tillett WS, Francis Jr T (1930). "Serological reactions in pneumonia with a nonprotein somatic fraction of pneumococcus". J Exp Med. 52: 561–585.
- ↑ NCBI Entrez Protein #CAA39671 [1]
- ↑ Torelli, Julius (2005), Beyond Cholesterol, p.45. ISBN 0-312-34863-0
- ↑ Pradhan AD (2001). "C-reactive protein, interleukin 6, and risk of developing type 2 diabetes mellitus". JAMA. 286: 327&ndash, 334. PMID 11466099.
- ↑ Dehghan A (2007). "Genetic variation, C-reactive protein levels, and incidence of diabetes". Diabetes. 56: 872. PMID 17327459.
- ↑ Esther Lopez-Garcia (2005). "Consumption of Trans Fatty Acids Is Related to Plasma Biomarkers of Inflammation and Endothelial Dysfunction". The Journal of Nutrition. 135 (3): 562&ndash, 566. PMID 15735094.
- ↑ John Danesh (2004). "C-Reactive Protein and Other Circulating Markers of Inflammation in the Prediction of Coronary Heart Disease". New England Journal of Medicine. 350 (14): 1387&ndash, 1397. PMID 15070788.
- ↑ Koenig, Wolfgang (2006). C-Reactive Protein – A Critical Cardiovascular Risk Marker [2]
- ↑ Pepys MB, Hirschfield GM, Tennent GA, Gallimore JR, Kahan MC, Bellotti V, Hawkins PN, Myers RM, Smith MD, Polara A, Cobb AJ, Ley SV, Aquilina JA, Robinson CV, Sharif I, Gray GA, Sabin CA, Jenvey MC, Kolstoe SE, Thompson D, Wood SP (2006). "Targeting C-reactive protein for the treatment of cardiovascular disease". Nature. 440: 1217&ndash, 1221. PMID 16642000.
- ↑ Erlinger TP, Platz EA, Rifai N, Helzlsouer KJ (2004). "C-reactive protein and the risk of incident colorectal cancer". Journal of the American Medical Association. 291 (Feb. 4): 585–590. PMID 14762037.
- ↑ Baron JA; et al. (2003). "A randomized trial of aspirin to prevent colorectal adenomas". New England Journal of Medicine. 348: 891–899. PMID 12621133.
Resources
- MedlinePlus Encyclopedia 003356
- Inflammation, Heart Disease and Stroke: The Role of C-Reactive Protein (American Heart Association)
- C-Reactive+Protein at the US National Library of Medicine Medical Subject Headings (MeSH)
da:CRP de:C-reaktives Protein it:Proteina C-reattiva he:חלבון מגיב C nl:C-reactief proteïne no:C-reaktivt protein fi:CRP sv:C-reaktivt protein