Neck of femur fracture pathophysiology
|
Neck of femur fracture Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Neck of femur fracture pathophysiology On the Web |
|
American Roentgen Ray Society Images of Neck of femur fracture pathophysiology |
|
Risk calculators and risk factors for Neck of femur fracture pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Rohan A. Bhimani, M.B.B.S., D.N.B., M.Ch.[2]
Overview
The pattern of fracture and degree of comminution are the resultant of several factors or variables such as the nature of injury, the bone quality, the age and weight of the patient, the energy involved, and the position of the hip and leg at the time of impact. Various combinations of these variables lead to a variety of different fracture patterns.
Pathophysiology
 |
{kind=link}
- The fracture pattern and severity of comminution depends on multiple factors including:[1]
- Decrease in bone mass density involves following process:[2]
- Autophagy is the mechanism through which osteocytes evade oxidative stress.
- The capability of autophagy in cells decreases as they age, a major factor of aging.
- As osteocytes grow, viability of cells decrease thereby decreasing the bone mass density.
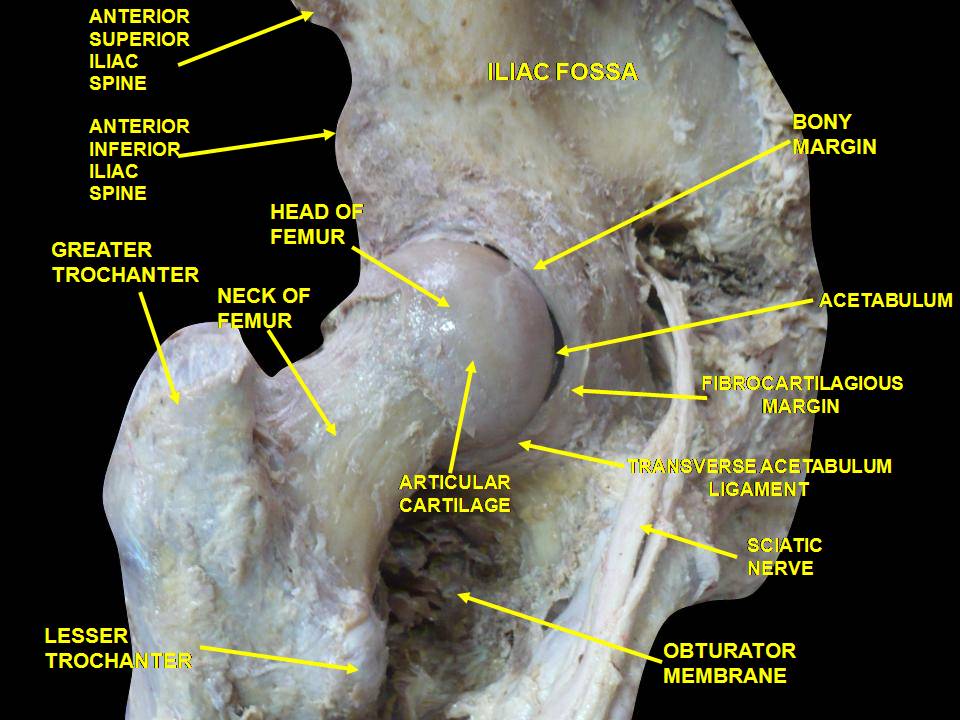
Anatomy
- The femoral neck of femur is supported by five groups of trabecular bone.[3][4]
- The thickest trabeculae bone is situated at the medial femoral neck, the calcar, and is known as the primary compressive trabeculae.
- The primary tensile group stretches from the inferior part of the femoral head, across the superior region, and ends in the lateral femur just distal to the greater trochanter .
- However, Ward’s triangle an area of relative weakness , is situated in the femoral neck which is formed by the intersections of three groups of trabeculae.
- The neck–shaft angle in a normal adult is between 125 and 135°.
- Femoral anteversion is defined as the angle subtended by the long axis of the femoral head and transverse axis of the femoral condyles and has a mean value of 8°.
- The blood supply to the femoral head derives from three main sources:
- These vessels subdivide into ascending retinacular arteries while course along the femoral neck and are at risk of disruption in the event of a femoral neck fracture, thus leading to a substantial risk of developing avascular necrosis.
Mechanism of Fracture
- Femoral neck fractures tend to occur in older adults due to low energy trauma such as fall.[5]
- The mechanisms of injury in elderly include:
- A direct impact onto the lateral hip.
- A twisting injury in which the patient's foot is planted and the body rotates leading to fracture.
- A sudden spontaneous completion of a stress fracture, which may lead to a fall.
- In younger adults, femoral neck fractures occur as a result of high energy trauma such as a motor vehicle accident.
- The femur is usually axially loaded.
- If the hip is in abduction at the time of injury, a femoral neck fracture occurs.
- If the hip is in adduction, it results in a fracture-dislocation.
Factors Affecting Healing
- Factors hampering healing include:[6][7]
- As the fracture is intracapsular, it is bathed in synovial fluid.
- The synovial fluid has a tamponade effect.
- In addition, it also lacks periosteal layer thus callus formation limited, which hampers healing.
Associated Conditions
Conditions associated with poor bone quality leading to neck of femur fracture include:[8]
- Osteoporosis
- Osteopenia
- chronic stroke
- Diabetes
- Rheumatoid arthritis
- Chronic kidney disease
- Hyperparathyroidism
- Hypophosphatemic rickets
- Immobility
- Menopause
- Multiple myeloma
- Mixed connective tissue disease
- Paget's disease of bone
- Primary hypoparathyroidism
- Short stature
- Chronic corticosteroid use
Gross Pathology
On gross pathology, decreased bone density and small pores in diaphysis of bones are characteristic findings of osteoporosis, leading to distal radius fracture.[9]
 |
Microscopic Pathology
- On microscopy, characteristic findings of bone with osteoporosis is increased number of osteoclasts and decreased number of osteoblasts under the microscope.[2]
References
- ↑ Azar, Frederick (2017). Campbell's operative orthopaedics. Philadelphia, PA: Elsevier. ISBN 9780323374620.
- ↑ 2.0 2.1 Onal M, Piemontese M, Xiong J, Wang Y, Han L, Ye S; et al. (2013). "Suppression of autophagy in osteocytes mimics skeletal aging". J Biol Chem. 288 (24): 17432–40. doi:10.1074/jbc.M112.444190. PMC 3682543. PMID 23645674.
- ↑ Ejnisman L, Philippon MJ, Lertwanich P, Pennock AT, Herzog MM, Briggs KK; et al. (2013). "Relationship between femoral anteversion and findings in hips with femoroacetabular impingement". Orthopedics. 36 (3): e293–300. doi:10.3928/01477447-20130222-17. PMID 23464948.
- ↑ Ehlinger, M.; Moser, T.; Adam, P.; Bierry, G.; Gangi, A.; de Mathelin, M.; Bonnomet, F. (2011). "Early prediction of femoral head avascular necrosis following neck fracture". Orthopaedics & Traumatology: Surgery & Research. 97 (1): 79–88. doi:10.1016/j.otsr.2010.06.014. ISSN 1877-0568.
- ↑ Blair B, Koval KJ, Kummer F, Zuckerman JD (1994). "Basicervical fractures of the proximal femur. A biomechanical study of 3 internal fixation techniques". Clin Orthop Relat Res (306): 256–63. PMID 8070205.
- ↑ Deneka DA, Simonian PT, Stankewich CJ, Eckert D, Chapman JR, Tencer AF (1997). "Biomechanical comparison of internal fixation techniques for the treatment of unstable basicervical femoral neck fractures". J Orthop Trauma. 11 (5): 337–43. PMID 9294797.
- ↑ Stankewich CJ, Chapman J, Muthusamy R, Quaid G, Schemitsch E, Tencer AF; et al. (1996). "Relationship of mechanical factors to the strength of proximal femur fractures fixed with cancellous screws". J Orthop Trauma. 10 (4): 248–57. PMID 8723403.
- ↑ Rockwood, Charles (2010). Rockwood and Green's fractures in adults. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN 9781605476773.
- ↑ Rockwood, Charles (2010). Rockwood and Green's fractures in adults. Philadelphia, PA: Wolters Kluwer Health/Lippincott Williams & Wilkins. ISBN 9781605476773.