Aortic coarctation pathophysiology: Difference between revisions
(New page: {{Template:Aortic Coarctation}} {{CMG}} '''Associate Editor-in-Chief:''' {{CZ}} ==Pathophysiology== Coarctation of the aorta can be either congenital or acquired. '''Congenital coarcta...) |
Ahmed Younes (talk | contribs) No edit summary |
||
| (32 intermediate revisions by 7 users not shown) | |||
| Line 1: | Line 1: | ||
<div style="-webkit-user-select: none;"> | |||
{|class="infobox" style="position: fixed; top: 65%; right: 10px; margin: 0 0 0 0; border: 0; float: right; | |||
|- | |||
| {{#ev:youtube|https://https://www.youtube.com/watch?v=0OqTJwZkRL4|350}} | |||
|- | |||
|}__NOTOC__ | |||
{{Aortic coarctation}} | |||
{{CMG}}; '''Associate Editor(s)-In-Chief:''' [[Priyamvada Singh|Priyamvada Singh, M.B.B.S.]][mailto:psingh13579@gmail.com], {{CZ}}; '''Assistant Editor(s)-In-Chief:''' [[Kristin Feeney|Kristin Feeney, B.S.]][mailto:kfeeney@elon.edu] | |||
==Overview== | |||
An aortic coarctation results from both, [[congenital]] and [[acquired]] means. Factors directly influencing the pathophysiology include defect location and sites of secondary [[dilation]]. | |||
==Pathophysiology== | |||
<div align="left"> | |||
<gallery heights="225" widths="225"> | |||
Image:COA_PAth.jpg|Coarctation of the descending aorta. | |||
Image:Coarctation and PDA.png|Schematic drawing of alternative locations of a coarctation of the aorta, relative to the ductus arteriosus. A: ductal coarctation, B: preductal coarctation, C: postductal coarctation. 1: Aorta ascendens, 2: Arteria pulmonalis, 3: Ductus arteriosus, 4: Aorta descendens, 5: Trunchus brachiocephalicus, 6: Arteria carotis communis sinister, 7: Arteria subclavia sinister | |||
</gallery> | |||
</div> | |||
Coarctation of the aorta can be: | |||
*[[Congenital]] coarctation resulting from an infolding of the aortic media that incorportaes ductal tissue, forming a ridge that eccentrically narrows the lumen of the vessel. Subsequent intimal proliferation on the ridge leads to progressive narrowing of the vessel lumen. There is a [[dilatation]] before and after the narrowing, giving the [[aorta]] an hourglass appearance. The exact etiology of the aortic abnormality remains unclear but likely involves a defect in the vascular wall of the [[aorta]] due to reduced antegrade intrauterine [[blood flow]] or to constriction of ductal tissue extending into the [[thoracic aorta]]. | |||
*[[Acquired]] coarctation occurring in systemic arteritides such as [[Takayasu arteritis]]. Additionally it may occur in rare cases of severe [[atherosclerosis]]. | |||
<br clear="left"/> | |||
===Defect Location=== | |||
[[Image:COA.jpg|center|500px]] | |||
<br clear="left"/> | |||
*95% of the lesions are located distal to the left [[subclavian artery]] and proximal to the [[ductus arteriosus]] (preductal coarctation) or just at or distal to the ductus (postductal coarctation). | |||
*5% of coarctations are located proximal to the left [[subclavian artery]], or rarely in the [[abdominal aorta]]. | |||
*In some cases, coarctation presents as a long segment or a tubular [[hypoplasia]]. | |||
*The [[stenosis]] is caused by an infolding of the left posterolateral aspect of the aortic wall resulting in an eccentric narrowing. | |||
===Sites of Secondary Dilation=== | |||
*[[Aorta]] proximal to the coarct | |||
*[[Aorta]] distal to the coarctation | |||
*[[Left subclavian artery]] | |||
*The narrowing progresses throughout life, and extensive [[collaterals]] develop from the subclavian (predominantly) and [[axillary arteries]] through: | |||
:#[[Internal mammary artery]] | |||
:#[[Scapular artery]] | |||
:#[[Intercostal arteries]] | |||
:#Epigastric arteries | |||
:#[[Anterior spinal arteries]] | |||
===Genetics=== | |||
* Aortic coarctation, like many [[congenital heart disease]]s, is more common in patients with other [[genetic condition]]s. | |||
* As many as 10-25% of patients with [[Turner syndrome]] have an accompanying coarctation of the aorta. | |||
===Gross Pathology=== | |||
<small> [http://www.peir.net Images courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology] </small> | |||
== | <div align="left"> | ||
Coarctation of the aorta | <gallery heights="225" widths="225"> | ||
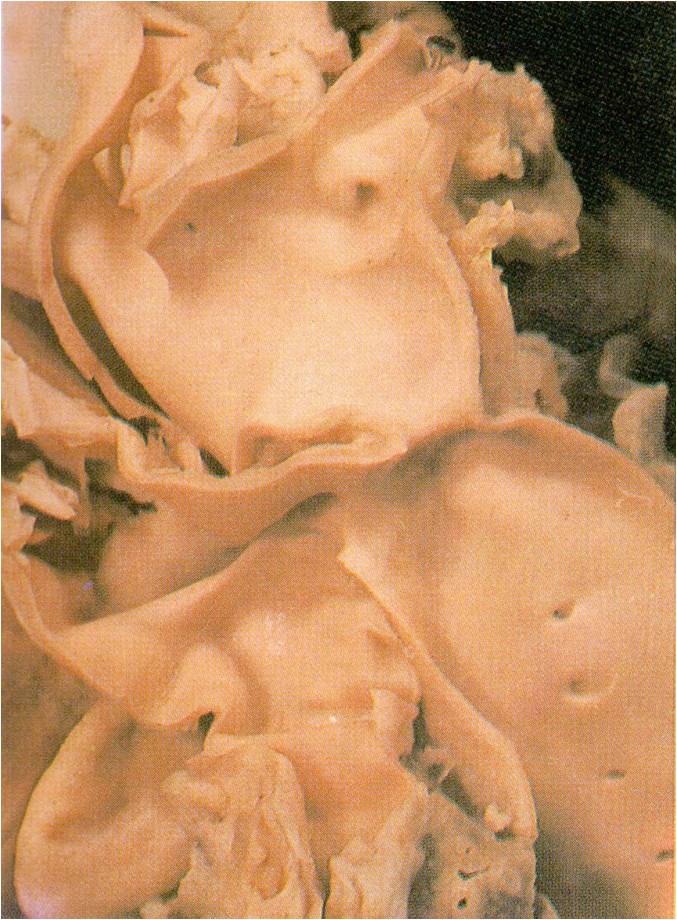
Image:Aortic coarctation adult type.jpg|AORTA: Coarctation, Adult: Gross, fixed tissue, an excellent illustration of postductal coarctation | |||
Image:Hypoplastic aortic arch with infantile type coarctation.jpg|AORTA: Coarctation: Gross, hypoplastic aortic arch and infantile coarctation well demonstrated. | |||
Image:COA 3.jpg|Localized Coarctation of the aorta. | |||
</gallery> | |||
</div> | |||
===Associated Conditions=== | |||
* It is commonly associated with [[bicuspid aortic valve]]. | |||
* There is 5 fold increase in the intracranial [[aneurysm]] in patient with coarctation. | |||
==Videos== | |||
{{#ev:youtube|SiNJfvK_qeI}} | |||
==References== | ==References== | ||
{{reflist|2}} | {{reflist|2}} | ||
{{WH}} | |||
{{WS}} | |||
[[CME Category::Cardiology]] | |||
[[Category:Cardiology]] | [[Category:Cardiology]] | ||
[[Category:Pediatrics]] | [[Category:Pediatrics]] | ||
[[Category: | [[Category:Disease]] | ||
[[Category:Congenital heart disease]] | |||
Latest revision as of 16:03, 11 July 2017
| https://https://www.youtube.com/watch?v=0OqTJwZkRL4%7C350}} |
|
Aortic coarctation Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Aortic coarctation pathophysiology On the Web |
|
American Roentgen Ray Society Images of Aortic coarctation pathophysiology |
|
Risk calculators and risk factors for Aortic coarctation pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-In-Chief: Priyamvada Singh, M.B.B.S.[2], Cafer Zorkun, M.D., Ph.D. [3]; Assistant Editor(s)-In-Chief: Kristin Feeney, B.S.[4]
Overview
An aortic coarctation results from both, congenital and acquired means. Factors directly influencing the pathophysiology include defect location and sites of secondary dilation.
Pathophysiology
-
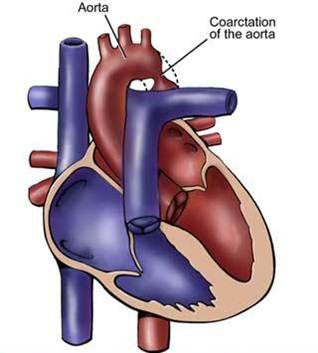
Coarctation of the descending aorta.
-
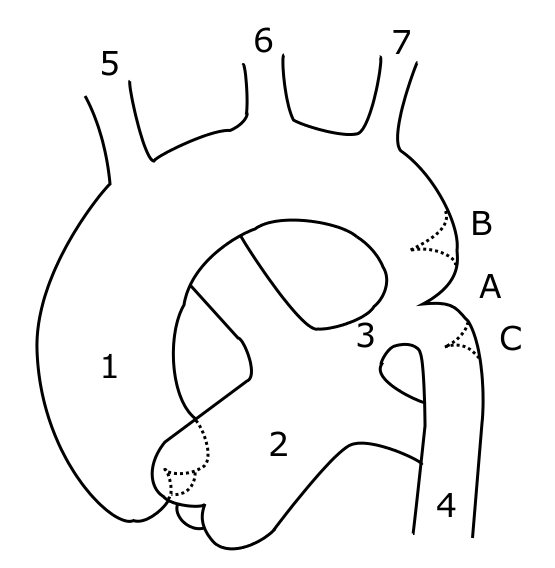
Schematic drawing of alternative locations of a coarctation of the aorta, relative to the ductus arteriosus. A: ductal coarctation, B: preductal coarctation, C: postductal coarctation. 1: Aorta ascendens, 2: Arteria pulmonalis, 3: Ductus arteriosus, 4: Aorta descendens, 5: Trunchus brachiocephalicus, 6: Arteria carotis communis sinister, 7: Arteria subclavia sinister


Coarctation of the aorta can be:
- Congenital coarctation resulting from an infolding of the aortic media that incorportaes ductal tissue, forming a ridge that eccentrically narrows the lumen of the vessel. Subsequent intimal proliferation on the ridge leads to progressive narrowing of the vessel lumen. There is a dilatation before and after the narrowing, giving the aorta an hourglass appearance. The exact etiology of the aortic abnormality remains unclear but likely involves a defect in the vascular wall of the aorta due to reduced antegrade intrauterine blood flow or to constriction of ductal tissue extending into the thoracic aorta.
- Acquired coarctation occurring in systemic arteritides such as Takayasu arteritis. Additionally it may occur in rare cases of severe atherosclerosis.
Defect Location

- 95% of the lesions are located distal to the left subclavian artery and proximal to the ductus arteriosus (preductal coarctation) or just at or distal to the ductus (postductal coarctation).
- 5% of coarctations are located proximal to the left subclavian artery, or rarely in the abdominal aorta.
- In some cases, coarctation presents as a long segment or a tubular hypoplasia.
- The stenosis is caused by an infolding of the left posterolateral aspect of the aortic wall resulting in an eccentric narrowing.
Sites of Secondary Dilation
- Aorta proximal to the coarct
- Aorta distal to the coarctation
- Left subclavian artery
- The narrowing progresses throughout life, and extensive collaterals develop from the subclavian (predominantly) and axillary arteries through:
- Internal mammary artery
- Scapular artery
- Intercostal arteries
- Epigastric arteries
- Anterior spinal arteries
Genetics
- Aortic coarctation, like many congenital heart diseases, is more common in patients with other genetic conditions.
- As many as 10-25% of patients with Turner syndrome have an accompanying coarctation of the aorta.
Gross Pathology
-

AORTA: Coarctation, Adult: Gross, fixed tissue, an excellent illustration of postductal coarctation
-

AORTA: Coarctation: Gross, hypoplastic aortic arch and infantile coarctation well demonstrated.
-
Localized Coarctation of the aorta.



Associated Conditions
- It is commonly associated with bicuspid aortic valve.
- There is 5 fold increase in the intracranial aneurysm in patient with coarctation.
Videos
{{#ev:youtube|SiNJfvK_qeI}}