Placenta previa
| https://https://www.youtube.com/watch?v=xnRIF8SDYf8%7C350}} |
For patient information, click here Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
|
Placenta previa Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Placenta previa On the Web |
|
American Roentgen Ray Society Images of Placenta previa |
Overview
Placenta praevia (placenta previa AE) is an obstetric complication in which the placenta has attached to the uterine wall close to or covering the cervix [2]. It can some times occur in the latter part of the first trimester, but usually during the second or third. It is a leading cause of antepartum haemorrhage (vaginal bleeding). It affects approximately 0.5% of all labours.
Pathophysiology
No specific cause of placenta praevia has yet been found but it is hypothesized to be related to abnormal vascularisation of the endometrium caused by scarring or atrophy from previous trauma, surgery, or infection.
In the last trimester of pregnancy the isthmus of the uterus unfolds and forms the lower segment. In a normal pregnancy the placenta does not overlie it, so there is no bleeding. If the placenta does overlie the lower segment, it may shear off and a small section may bleed.
Women with placenta praevia often present with painless, bright red vaginal bleeding. This bleeding often starts mildly and may increase as the area of placental separation increases. Praevia should be suspected if there is bleeding after 24 weeks of gestation. Abdominal examination usually finds the uterus non-tender and relaxed. Leopold's Maneuvers may find the fetus in an oblique or breech position or lying transverse as a result of the abnormal position of the placenta. Praevia can be confirmed with an ultrasound. In parts of the world where an ultrasound not available, it is not uncommon to confirm the diagnosis with an examination in the surgical theatre.
The proper timing of an examination in theatre is important. If the woman is not bleeding severely she can be managed non-operatively until the 36th week. By this time the baby's chance of survival is as good as at full term.
Placenta praevia is classified according to the placement of the placenta:
- Type I or low lying: The placenta encroaches the lower segment of the uterus but does not infringe on the cervical os.
- Type II or marginal: The placenta touches, but does not cover, the top of the cervix.
- Type III or partial: The placenta partially covers the top of the cervix.
- Type IV or complete: The placenta completely covers the top of the cervix. This type of praevia often will not bleed until labour starts.
Placenta praevia is itself a risk factor of placenta accreta.
Risk factors
The following have been identified as risk factors for placenta praevia:
- Previous placenta praevia, caesarean delivery,[1] or abortion.
- Women who have had previous pregnancies, especially a large number of closely spaced pregnancies, are at higher risk.
- Women who are younger than 20 are at higher risk and women older than 30 are at increasing risk as they get older.
- Women with a large placentae from twins or erythroblastosis are at higher risk.
- Women who smoke or use cocaine may be at higher risk.
- Race is a controversial risk factor, with some studies finding minorities at higher risk and others finding no difference.
Diagnostic Findings
MRI
-
 Placenta previa
Placenta previa -
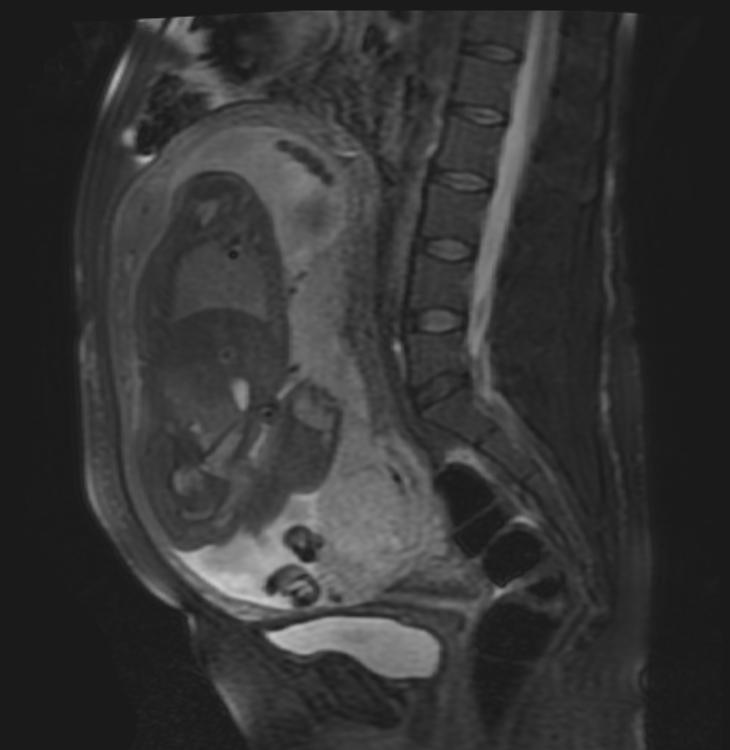 Placenta previa
Placenta previa -
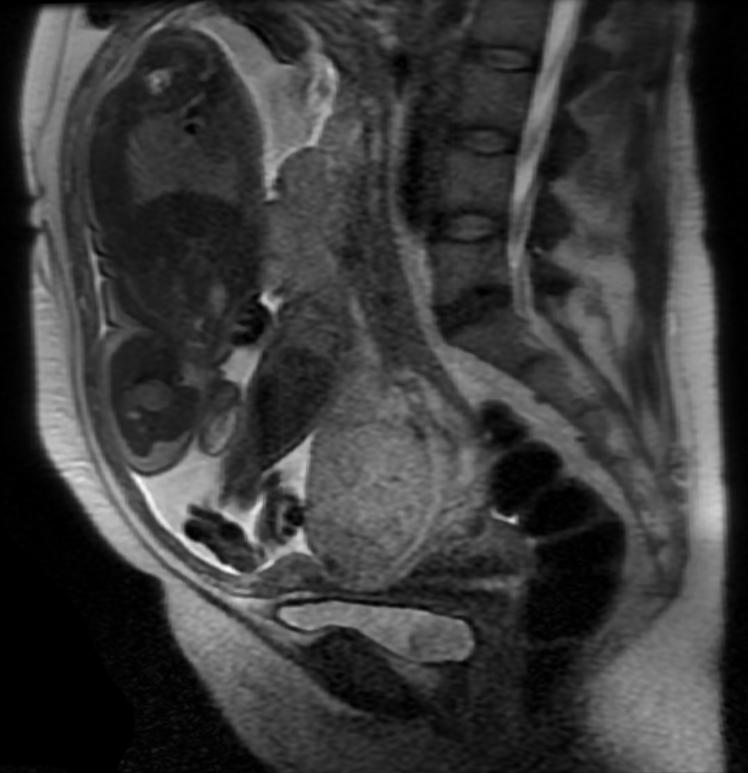 Placenta previa
Placenta previa



Intervention
An initial assessment to determine the status of the mother and fetus is required. Although mothers used to be treated in the hospital from the first bleeding episode until birth, it is now considered safe to treat placenta praevia on an outpatient basis if the fetus is at less than 37 weeks of gestation, and neither the mother or the fetus are in distress.
Immediate delivery of the fetus may be indicated if the fetus is mature or if the fetus or mother are in distress. Blood volume replacement (to maintain blood pressure) and blood plasma replacement (to maintain fibrinogen levels) may be necessary.
It is controversial if vaginal delivery or a Ceasarean section is the safest method of delivery. In cases of fetal distress a Ceasarean section is indicated. Caesarian section is contraindicated in cases of disseminated intravascular coagulation.
A problem exists in places where a Ceasarean section cannot be performed, due to the lack of a surgeon or equipment. In these cases the infant can be delivered vaginally. There are two ways of doing this with a placenta praevia:
- The baby's head can be brought down to the placental site (if necessary with Willet's forceps or a vulsellum) and a weight attached to his scalp
- A leg can be brought down and the baby's buttocks used to compress the placental site
The goal of this type of delivery is to save the mother, and both methods will often kill the baby. These methods were used for many years before Ceasarean section and saved the lives of both mothers and babies with this condition.
The main risk with a vaginal delivery with a praevia is that as you are trying to bring down the head or a leg, you might separate more of the placenta and increase the bleeding.
Placenta praevia increases the risk of puerperal sepsis and postpartum haemorrhage because the lower segment to which the placenta was attached contracts less well post-delivery.
Contraindicated medications
Placenta previa is considered an absolute contraindication to the use of the following medications:
References
- ↑ Weerasekera DS (2000). "Placenta praevia and scarred uterus - an obstetrician's dilemma". Journal of obstetrics and gynaecology : the journal of the Institute of Obstetrics and Gynaecology. 20 (5): 484–5. doi:10.1080/014436100434659. PMID 15512632.
Template:SIB de:Placenta praevia it:Placenta previa sv:Placenta praevia