Piperacillin
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Overview
Piperacillin is an antibiotic that is FDA approved for the treatment of serious infections caused by susceptible strains ,hepatobiliary and surgical infections caused by E. coli, Pseudomonas aeruginosa, enterococci, Clostridium spp., anaerobic cocci, or Bacteroides spp,urinary tract infections, septicemia, lower respiratorytract infections, skin, infections ,bone and joint infections. Common adverse reactions include thrombophlebitis, erythema multiforme, stevens-johnson syndrome, toxic epidermal necrolysis, agranulocytosis, hemolytic anemia, pancytopenia, anaphylaxis, seizure, renal failure.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Therapeutic
- Piperacillin is indicated for the treatment of serious infections caused by susceptible strains of the designated microorganisms in the conditions listed below:
- Intra-Abdominal Infections including hepatobiliary and surgical infections caused by E. coli, Pseudomonas aeruginosa, enterococci, Clostridium spp., anaerobic cocci, or Bacteroides spp., including B. fragilis.
- Urinary Tract Infections caused by E. coli, Klebsiella spp., P. aeruginosa, Proteus spp., including P. mirabilis, or enterococci.
- Gynecologic Infections including endometritis, pelvic inflammatory disease, pelvic cellulitis caused by Bacteroides spp., including B. fragilis, anaerobic cocci, Neisseria gonorrhoeae, or enterococci (E. faecalis).
- Septicemia including bacteremia caused by E. coli, Klebsiella spp., Enterobacter spp., Serratia spp., P. mirabilis, S. pneumoniae, enterococci, P. aeruginosa, Bacteroides spp., or anaerobic cocci.
- Lower RespiratoryTract Infections caused by E. coli, Klebsiella spp., Enterobacter spp., P. aeruginosa, Serratia spp., H. influenzae, Bacteroides spp., or anaerobic cocci. * Although improvement has been noted in patients with cystic fibrosis, lasting bacterial eradication may not necessarily be achieved.
- Skin and Skin Structure Infections caused by E. coli, Klebsiella spp., Serratia spp., Acinetobacter spp., Enterobacter spp., P. aeruginosa, Morganella morganii, Providencia rettgeri, Proteus vulgaris, P. mirabilis, Bacteroides spp., including B. fragilis, anaerobic cocci, or enterococci.
- Bone and Joint Infections caused by P. aeruginosa, enterococci, Bacteroides spp., or anaerobic cocci.
- Uncomplicated Gonococcal Urethritis caused by N. gonorrhoeae.
- Piperacillin has also been shown to be clinically effective for the treatment of infections at various sites caused by Streptococcus species including S. pyogenes and S. pneumoniae; however, infections caused by these organisms are ordinarily treated with more narrow spectrum penicillins.
- Because of its broad spectrum of bactericidal activity against gram-positive and gram-negative aerobic and anaerobic bacteria, piperacillin is particularly useful for the treatment of mixed infections and presumptive therapy prior to the identification of the causative organisms.
- Also, piperacillin may be administered as single drug therapy in some situations where normally two antibiotics might be employed.
- Piperacillin has been successfully used with aminoglycosides, especially in patients with impaired host defenses. Both drugs should be used in full therapeutic doses.
- Appropriate cultures should be made for susceptibility testing before initiating therapy and therapy adjusted, if appropriate, once the results are known.
Prophylaxis
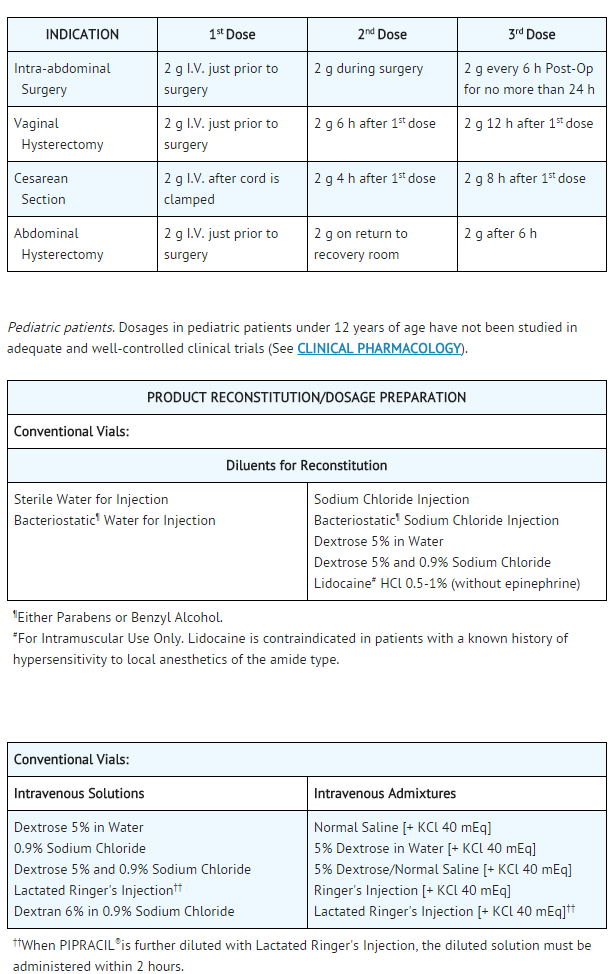
- Piperacillin is indicated for prophylactic use in surgery including intra-abdominal (gastrointestinal and biliary) procedures, vaginal hysterectomy, abdominal hysterectomy, and cesarean section.
- Effective prophylactic use depends on the time of administration; piperacillin should be given one-half to one hour before the operation so that effective levels can be achieved in the site prior to the procedure.
- The prophylactic use of piperacillin should be stopped within 24 hours, since continuing administration of any antibiotic increases the possibility of adverse reactions, but in the majority of surgical procedures, does not reduce the incidence of subsequent infections. If there are signs of infection, specimens for culture and susceptibility testing should be obtained for identification of the causative microorganism so that appropriate therapy can be instituted.
- To reduce the development of drug-resistant bacteria and maintain the effectiveness of piperacillin and other antibacterial drugs, piperacillinshould only be used to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy.
- Piperacillin may be administered by the intramuscular route or intravenously as a three- to five-minute intravenous injection or as a 20- to 30-minute infusion. The usual dosage of piperacillin for serious infections is 3 to 4 g given every four to six hours as a 20- to 30-minute infusion. For serious infections, the intravenous route should be used.
- Piperacillin should not be mixed with an aminoglycoside in a syringe or infusion bottle since this can result in inactivation of the aminoglycoside.
- The maximum daily dose for adults is usually 24 g/day, although higher doses have been used.
- Intramuscular injections should be limited to 2 g per injection site. This route of administration has been used primarily in the treatment of patients with uncomplicated gonorrhea and urinary tract infections.

This image is provided by the National Library of Medicine.

- The average duration of piperacillin treatment is from seven to ten days, except in the treatment of gynecologic infections, which is from three to ten days; the duration should be guided by the patient's clinical and bacteriological progress. For most acute infections, treatment should be continued for at least 48 to 72 hours after the patient becomes asymptomatic. * Antibiotic therapy for S. pyogenes infections should be maintained for at least ten days to reduce the risk of rheumatic fever.
- When piperacillin is given concurrently with aminoglycosides, both drugs should be used in full therapeutic doses.
Renal Impairment

This image is provided by the National Library of Medicine.

- For patients on hemodialysis, the maximum daily dose is 6 g/day (2 g every 8 hours). In addition, because hemodialysis removes 30% to 50% of piperacillin in 4 hours, a 1-g additional dose should be administered following each dialysis period.
- For patients with renal failure and hepatic insufficiency, measurement of serum levels of piperacillin will provide additional guidance for adjusting dosage.
Prophylaxis
- When possible, piperacillin should be administered as a 20- to 30-minute infusion just prior to anesthesia. Administration while the patient is awake will facilitate identification of possible adverse reactions during drug infusion.
This image is provided by the National Library of Medicine.

Intravenous Administration
- Reconstitution Directions for Conventional Vials:
- Reconstitute each gram of piperacillin with at least 5 mL of a suitable diluent (except Lidocaine HCl 0.5%-1% without epinephrine) listed above. Shake well until dissolved. Reconstituted solution may be diluted to the desired volume (eg, 50 or 100 mL) in the above listed intravenous solutions and admixtures.
DIRECTIONS FOR ADMINISTRATION
Intermittent IV Infusion
- Infuse diluted solution over period of about 30 minutes. During infusion, it is desirable to discontinue the primary intravenous solution.
Intravenous Injection (Bolus)
- Reconstituted solution should be injected slowly over a 3-to 5-minute period to help avoid vein irritation.
- Intramuscular Administration (Conventional Vials Only)
- Reconstitution Directions
- Reconstitute each gram of piperacillin with 2 mL of a suitable diluent listed above to achieve a concentration of 1 g per 2.5 mL. Shake well until dissolved.
DIRECTIONS FOR ADMINISTRATION
- When indicated by clinical and bacteriological findings, intramuscular administration of 6 to 8 g daily of piperacillin, in divided doses, may be utilized for initiation of therapy.
- In addition, intramuscular administration of the drug may be considered for maintenance therapy after clinical and bacteriologic improvement has been obtained with intravenous piperacillin sodium treatment. Intramuscular administration should not exceed 2 g per injection at any one site.
- The preferred site is the upper outer quadrant of the buttock (ie, gluteus maximus).
- The deltoid area should be used only if well-developed, and then only with caution to avoid radial nerve injury. Intramuscular injections should not be made into the lower or mid-third of the upper arm.
- Stability of piperacillin Following Reconstitution
- Piperacillin is stable in both glass and plastic containers when reconstituted with recommended diluents and when diluted with the intravenous solutions and intravenous admixtures indicated above.
- Pharmacy vials should be used immediately after reconstitution. Discard any unused portion after 24 hours if stored at room temperature (20° to 25°C [68° to 77°F]), or after 48 hours if stored at refrigerated temperature (2° to 8°C [36° to 46°F]). Vials should not be frozen after reconstitution.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Piperacillin in adult patients.
Non–Guideline-Supported Use
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Piperacillin in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Piperacillin in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Piperacillin in pediatric patients.
Contraindications
- Piperacillin is contraindicated in patients with a history of allergic reactions to any of the betalactams, including penicillins and/or cephalosporins.
Warnings
- SERIOUS AND OCCASIONALLY FATAL HYPERSENSITIVITY (ANAPHYLACTIC/ANAPHYLACTOID) REACTIONS HAVE BEEN REPORTED IN PATIENTS ON PENICILLIN THERAPY. THESE REACTIONS ARE MORE LIKELY TO OCCUR IN INDIVIDUALS WITH A HISTORY OF PENICILLIN HYPERSENSITIVITY AND/OR A HISTORY OF SENSITIVITY TO MULTIPLE ALLERGENS. THERE HAVE BEEN REPORTS OF INDIVIDUALS WITH A HISTORY OF PENICILLIN HYPERSENSITIVITY WHO HAVE EXPERIENCED SEVERE REACTIONS WHEN TREATED WITH CEPHALOSPORINS. BEFORE INITIATING THERAPY WITH piperacillin, CAREFUL INQUIRY SHOULD BE MADE CONCERNING PREVIOUS HYPERSENSITIVITY REACTIONS TO PENICILLINS, CEPHALOSPORINS OR OTHER ALLERGENS. IF AN ALLERGIC REACTION OCCURS, piperacillin SHOULD BE DISCONTINUED AND APPROPRIATE THERAPY INSTITUTED. SERIOUS ANAPHYLACTIC/ANAPHYLACTOID REACTIONS REQUIRE IMMEDIATE EMERGENCY TREATMENT WITH EPINEPHRINE. OXYGEN, INTRAVENOUS STEROIDS AND AIRWAY MANAGEMENT, INCLUDING INTUBATION, SHOULD ALSO BE ADMINISTERED AS INDICATED.
- Clostridium difficile associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including piperacillin, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon leading to overgrowth of C. difficile.
- C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. difficile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents.
- If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. Appropriate fluid and electrolyte management, protein supplementation, antibiotic treatment of C. difficile, and surgical evaluation should be instituted as clinically indicated.
Adverse Reactions
Clinical Trials Experience
There is limited information regarding Clinical Trial Experience of Piperacillin in the drug label.
Postmarketing Experience
- Piperacillin is generally well tolerated. The most common adverse reactions have been local in nature, following intravenous or intramuscular injection. The following adverse reactions may occur:
Local Reactions
- In clinical trials thrombophlebitis was noted in 4% of patients. Pain, erythema, and/or induration at the injection site occurred in 2% of patients. Less frequent reactions including ecchymosis, deep vein thrombosis, and hematomas have also occurred.
Gastrointestinal
- Diarrhea and loose stools were noted in 2% of patients. Other less frequent reactions included vomiting, nausea, increases in liver enzymes (LDH, AST, ALT), hyperbilirubinemia, cholestatic hepatitis, bloody diarrhea, and pseudomembranous colitis. The onset of pseudomembranous colitis symptoms may occur during or after antibiotic treatment.
Hypersensitivity Reactions
- Anaphylactic/anaphylactoid reactions (some leading to shock and fatalities) have been reported.
- Rash was noted in 1% of patients. Other less frequent findings included pruritus, vesicular eruptions, and positive Coombs tests.
- Other dermatologic manifestations, such as erythema multiforme, urticaria, toxic epidermal necrolysis and Stevens-Johnson syndrome have been reported.
Renal
- Elevations of creatinine or BUN, renal failure and interstitial nephritis have been reported.
Central Nervous System
Hemic and Lymphatic
- Hemolytic anemia, agranulocytosis, pancytopenia, prolonged bleeding time, reversible leukopenia, neutropenia, thrombocytopenia, and/or eosinophilia have been reported. As with other β-lactam antibiotics, reversible leukopenia (neutropenia) is more apt to occur in patients receiving prolonged therapy at high dosages or in association with drugs known to cause this reaction.
Serum Electrolytes
- Individuals with liver disease or individuals receiving cytotoxic therapy or diuretics were reported to demonstrate a decrease in serum potassium concentrations with high doses of piperacillin.
- Hypokalemia has been reported.
Skeletal
- Prolonged muscle relaxation.
Other
- Fever, superinfection, including candidiasis; hemorrhagic manifestations have been reported.
- Piperacillin therapy has been associated with an increased incidence of fever and rash in cystic fibrosis patients.
Drug Interactions
Aminoglycosides
- The mixing of piperacillin with an aminoglycoside in vitro can result in substantial inactivation of the aminoglycoside.
Vecuronium
- When used in the perioperative period, piperacillin has been implicated in the prolongation of the neuromuscular blockade of vecuronium. Caution is indicated when piperacillin is used perioperatively. In one controlled clinical study, the ureidopenicillins, including piperacillin, were reported to prolong the action of vecuronium. Due to their similar mechanism of action, it is expected that the neuromuscular blockade produced by any of the non-depolarizing muscle relaxants could be prolonged in the presence of piperacillin.
Probenecid
- The oral combination of probenecid before intramuscular injection of piperacillin produces an increase in piperacillin peak serum level of about 30%.
Anticoagulants
- Coagulation parameters should be tested more frequently and monitored regularly during simultaneous administration of high doses of heparin, oral anticoagulants, or other drugs that may affect the blood coagulation system or the thrombocyte function.
Methotrexate
- Piperacillin sodium may reduce the excretion of methotrexate. Therefore, serum levels of methotrexate should be monitored in patients to avoid drug toxicity.
Drug/Laboratory Test Interactions
- As with other penicillins, the administration of piperacillin may result in a false-positive reaction for glucose in the urine using a copper-reduction method. It is recommended that glucose tests based on enzymatic glucose oxidase reactions be used.
- There have been reports of positive test results using the Bio-Rad Laboratories Platelia Aspergillus EIA test in patients receiving piperacillin/tazobactam injection who were subsequently found to be free of Aspergillus infection. Cross-reactions with non-Aspergillus polysaccharides and polyfuranoses with the Bio-Rad Laboratories Platelia Aspergillus EIA test have been reported.
- Therefore, positive test results in patients receiving piperacillin should be interpreted cautiously and confirmed by other diagnostic methods.
Use in Specific Populations
Pregnancy
- Teratology studies have been performed in mice (I.V.) and rats (I.V., I.P. and SQ) and have revealed no evidence of harm to the fetus due to piperacillin administered up to a dose which is approximately half the maximum recommended human daily dose based on body-surface area (mg/m2). In pharmacokinetic studies in pregnant and nonpregnant rats, in which piperacillin was administered I.V. at a dose which is half the maximum daily dose administered in teratology studies, serum concentrations in rats were approximately 10 times the maximum serum concentration seen in man. In other studies in mice and rats, in which piperacillin (in combination with a beta-lactamase inhibitor, tazobactam) was administered I.V. at approximately half the maximum daily dose administered in teratology studies, plasma concentrations of piperacillin were approximately 2 times (mice) and 5 times (rats) the serum concentrations seen in man.
- There are, however, no adequate and well-controlled studies with piperacillin in pregnant women. Because animal reproduction studies are not always predictive of the human response, this drug should be used during pregnancy only if clearly needed.
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Piperacillin in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Piperacillin during labor and delivery.
Nursing Mothers
- Piperacillin is excreted in low concentrations in human milk. Caution should be exercised when piperacillin is administered to nursing mothers.
Pediatric Use
- Safety and effectiveness in pediatric patients have not been established.
- Data from published pharmacokinetics studies indicate that the elimination half-life of piperacillin in neonates is twofold to fourfold longer than that seen in pediatric patients 1 month of age and above as well as in adults. In infants, children, and adolescents, the elimination half-life of piperacillin is shorter than that observed in adults. As in adults, the elimination of piperacillin is decreased in pediatric patients with renal impairment.
Geriatic Use
- Clinical studies of piperacillin did not include sufficient numbers of subjects aged 65 and over to determine whether they respond differently from younger subjects.
- In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concomitant disease or other drug therapy.
- Piperacillin contains 42.5 mg (1.85 mEq) of sodium per gram. At the usual recommended doses, patients would receive between 255 and 765 mg/day (11.1 and 33.3 mEq) of sodium. The geriatric population may respond with a blunted natriuresis to salt loading. The total sodium content from dietary and non-dietary sources may be clinically important with regard to such diseases as congestive heart failure.
- This drug is known to be substantially excreted by the kidney, and the risk of toxic reactions to this drug may be greater in patients with impaired renal function. Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
Gender
There is no FDA guidance on the use of Piperacillin with respect to specific gender populations.
Race
There is no FDA guidance on the use of Piperacillin with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Piperacillin in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Piperacillin in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Piperacillin in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Piperacillin in patients who are immunocompromised.
Administration and Monitoring
Administration
Monitoring
- Coagulation parameters should be tested more frequently and monitored regularly during simultaneous administration of high doses of heparin, oral anticoagulants, or other drugs that may affect the blood coagulation system or the thrombocyte function.
- Piperacillin sodium may reduce the excretion of methotrexate. Therefore, serum levels of methotrexate should be monitored in patients to avoid drug toxicity.
- Because elderly patients are more likely to have decreased renal function, care should be taken in dose selection, and it may be useful to monitor renal function.
IV Compatibility
There is limited information regarding IV Compatibility of Piperacillin in the drug label.
Overdosage
- There is no specific information on overdose with piperacillin. Other penicillin-class drugs in overdosage, however, have the potential to cause neuromuscular hyperirritability or convulsive seizures.
- In case of overdosage, discontinue medication, treat symptomatically, and institute supportive measures as required. Piperacillin can be removed by hemodialysis but not peritoneal dialysis.
Pharmacology

Mechanism of Action
There is limited information regarding Piperacillin Mechanism of Action in the drug label.
Structure
- PIPRACIL, sterile piperacillin sodium, is a semisynthetic broad-spectrum penicillin for parenteral use derived from D(-)-α-aminobenzylpenicillin. The chemical name of piperacillin sodium is sodium (2S,5R,6R)-6-[(R)-2-(4-ethyl-2,3-dioxo-1-piperazinecarboxamido)-2-phenylacetamido]-3,-3-dimethyl-7-oxo-4-thia-1-azabicyclo[3.2.0]heptane-2-carboxylate. The chemical formula is C23H26N5NaO7S, and the molecular weight is 539.54. Its structural formula is:

This image is provided by the National Library of Medicine.

- Piperacillin sodium powder is a white to off-white solid having the characteristic appearance of products prepared by freeze-drying. It is freely soluble in water and in alcohol. The pH of an aqueous solution containing 400 milligrams per milliliter ranges from 5.5 to 7.5. One g contains 1.85 mEq (42.5 mg) of sodium (Na+).
Pharmacodynamics
There is limited information regarding Pharmacodynamics of Piperacillin in the drug label.
Pharmacokinetics
Intravenous Administration
- In healthy adult volunteers, mean serum piperacillin concentrations immediately after a two‑to three‑minute intravenous injection of 2, 4, or 6 g were 305, 412, and 775 μg/mL, respectively. Serum concentrations lack dose proportionality.
- A 30-minute infusion of 6 g every 6 h gave, on the fourth day, a mean peak serum concentration of 420 μg/mL.
Intramuscular Administration
- Piperacillin is rapidly absorbed after intramuscular injection. In healthy volunteers, the mean peak serum concentration occurs approximately 30 minutes after a single dose of 2 g and is about 36 μg/mL. The oral administration of 1 g probenecid before injection produces an increase in piperacillin peak serum level of about 30%. The area under the curve (AUC) is increased by approximately 60%.
Pharmacokinetics
- Piperacillin is not absorbed when given orally. Peak serum concentrations are attained approximately 30 minutes after intramuscular injections and immediately after completion of intravenous injection or infusion. The serum half-life in healthy volunteers ranges from 36 minutes to one hour and 12 minutes. The mean elimination half-life of piperacillin in healthy adult volunteers is 54 minutes following administration of 2 g and 63 minutes following 6 g. As with other penicillins, piperacillin is eliminated primarily by glomerular filtration and tubular secretion; it is excreted rapidly as unchanged drug in high concentrations in the urine.
- Approximately 60% to 80% of the administered dose is excreted in the urine in the first 24 hours. Piperacillin urine concentrations, determined by microbioassay, are as high as 14,100 μg/mL following a 6-g intravenous dose and 8,500 μg/mL following a 4-g intravenous dose. These urine drug concentrations remain well above 1,000 μg/mL throughout the dosing interval.
Distribution
- Piperacillin binding to human serum proteins is 16%. The drug is widely distributed in human tissues and body fluids, including bone, prostate, and heart, and reaches high concentrations in bile. After a 4-g bolus injection, maximum biliary concentrations average 3,205 μg/mL. It penetrates into the cerebrospinal fluid in the presence of inflamed meninges.
Nonclinical Toxicology
There is limited information regarding Nonclinical Toxicology of Piperacillin in the drug label.
Clinical Studies
There is limited information regarding Clinical Studies of Piperacillin in the drug label.
How Supplied
- PIPRACIL ® (piperacillin for injection) is available in vials containing freeze-dried piperacillin sodium powder equivalent to two, three, and four g of piperacillin. One g of piperacillin (as a monosodium salt) contains 1.85 mEq (42.5 mg) of sodium.
- Product Numbers
- 2 gram/Vial-10 per box-NDC 0206-3879-16
- 3 gram/Vial-10 per box-NDC 0206-3882-55
- 4 gram/Vial-10 per box-NDC 0206-3880-25
Storage
- Store at controlled room temperature 20°C-25°C
Images
Drug Images
{{#ask: Page Name::Piperacillin |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel

{{#ask: Label Page::Piperacillin |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
There is limited information regarding Patient Counseling Information of Piperacillin in the drug label.
Precautions with Alcohol
- Alcohol-Piperacillin interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- PIPRACIL ®[2]
Look-Alike Drug Names
There is limited information regarding Piperacillin Look-Alike Drug Names in the drug label.
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
- ↑ Winston DJ, Ho WG, Young LS, Hewitt WL, Gale RP (1982). "Piperacillin plus amikacin therapy v carbenicillin plus amikacin therapy in febrile, granulocytopenic patients". Arch Intern Med. 142 (9): 1663–7. PMID 6214228 PMID: 6214228 Check
|pmid=value (help). - ↑ "PIPRACIL- piperacillin sodium injection, powder, lyophilized, for solution".