Dyspepsia pathophysiology
|
Dyspepsia Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Dyspepsia pathophysiology On the Web |
|
American Roentgen Ray Society Images of Dyspepsia pathophysiology |
|
Risk calculators and risk factors for Dyspepsia pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Ajay Gade MD[2]]
Overview
The symptoms of functional dyspepsia are directly caused by two major pathophysiological abnormalities in gastric motility and visceral sensitivity. These mechanisms occur in patients who have acquired excessive responsiveness to stress as a result of the environment during early life, genetic abnormalities, residual inflammation after gastrointestinal infections, or other causes. The process may be modified by factors including psychophysiological abnormalities, abnormal secretion of gastric acid, Helicobacter pylori infection, diet, and lifestyle.
Pathophysiology
The pathophysiology of dyspepsia is as follows:[1][2][3][4][5][6][7]
Physiology of digestion
- In humans, digestion begins in the mouth where food is chewed.
- Salivary amylase aids in the chemical breakdown of polysaccharides such as starch into disaccharides such as maltose.
- The chewed food is pushed down the esophagus into the stomach through peristaltic contraction of these muscles.
- Food enters the stomach where it is further broken down and thoroughly mixed with gastric acid, pepsin, and other digestive enzymes to break down proteins, fats and carbohydrates.
- After consumption of food, digestive "tonic" and peristaltic contractions begin, which helps break down the food and move it through the gastrointestinal tract. Gastric emptying is the release of food from the stomach into the duodenum.
- Gastric emptying has attracted medical interest as rapid gastric emptying is related to obesity and delayed gastric emptying syndrome is associated with diabetes mellitus, aging, gastroparesis and gastroesophageal reflux.
- After being processed in the stomach, food is passed to the small intestine. The majority of digestion and absorption occurs here after the milky chyme enters the duodenum. Here it is further mixed with three different digestive juices:
- Bile which is produced by the liver and stored in the gallbladder emulsifies fats and neutralizes the chyme.
- Pancreatic juice made by the pancreas. It secrete enzymes such as pancreatic amylase, pancreatic lipase, and trypsinogen.
- Intestinal juice secreted by the intestinal glands in the small intestine. It contains enzymes such as enteropeptidase, erepsin, trypsin, chymotrypsin, maltase, lactase, and sucrase.
Pathophysiology of functional dyspepsia
- The symptoms of functional dyspepsia (FD) are directly caused by two major physiological abnormalities
- Abnormal gastric motility. Gastroparesis and functional dyspepsia may be the same entity[8]
- Visceral hypersensitivity
- These mechanisms occur in patients who have acquired excessive responsiveness to stress as a result of the environment during early life, genetic abnormalities, residual inflammation after gastrointestinal infections, or other causes, with the process modified by factors including psychophysiological abnormalities, abnormal secretion of gastric acid, Helicobacter pylori infection, diet, and lifestyle.
- If the basis of this model of FD pathogenesis is excessive responsiveness of gastrointestinal function to stress and external stimuli, psychosomatic approaches to alter stress perception could be important treatment options.[9]
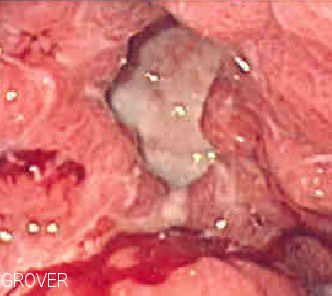
Gross Pathology
There are no significant gross or microscopic pathology associated with dyspepsia, however the gross and microscopic pathology of peptic ulcer disease should be kept in mind.
- Gastric ulcers are most often localized on the lesser curvature of the stomach
- Duodenal ulcers are more located at bulb of duodenum
- Characteristic findings of a peptic ulcer on gross pathology include:
- Round to oval
- Two to four cm diameter
- Smooth base with perpendicular borders.
- Parietal scarring with radial folds may be evident in the surrounding mucosa
-
 A benign gastric ulcer (from the antrum) of a gastrectomy Source:https://commons.wikimedia.org/wiki/File:Benign_gastric_ulcer_1.jpg#/media/File:Benign_gastric_ulcer_1.jpg
A benign gastric ulcer (from the antrum) of a gastrectomy Source:https://commons.wikimedia.org/wiki/File:Benign_gastric_ulcer_1.jpg#/media/File:Benign_gastric_ulcer_1.jpg -
 Duodenal ulcer specimen. Source: https://commons.wikimedia.org/wiki/File:Duodenal_ulcer01.jpg#/media/File:Duodenal_ulcer01.jpg
Duodenal ulcer specimen. Source: https://commons.wikimedia.org/wiki/File:Duodenal_ulcer01.jpg#/media/File:Duodenal_ulcer01.jpg -
 Gastric ulcer specimen Source:https://commons.wikimedia.org/wiki/File:Gastric_ulcer_3.jpg#/media/File:Gastric_ulcer_3.jpg
Gastric ulcer specimen Source:https://commons.wikimedia.org/wiki/File:Gastric_ulcer_3.jpg#/media/File:Gastric_ulcer_3.jpg

.jpg)

Microscopic Pathology
There are no significant gross or microscopic pathology associated with dyspepsia however, the gross and microscopic pathology of peptic ulcer disease should be kept in mind.
- A peptic ulcer is a mucosal defect produced by acid-pepsin aggression which penetrates the muscularis mucosae and muscularis propria
- There is increased plasma cells, neutrophilic infiltrate, villous blunting
- The surface epithelium usually shows mucous cell (pseudopyloric) metaplasia
- During the active phase, the base of the ulcer shows 4 zones:
- Inflammatory exudate: polymorphonuclear infiltration which along with bacterial products stimulate the production of IL-8 and tumor necrosis factor alpha (TNF-α) and IL-1 released by macrophages in response to bacterial lipopolysaccharide
- Fibrinoid necrosis
- Granulation tissue
- Fibrous tissue. The fibrous base of the ulcer may contain vessels with thickened wall or with thrombosis[10]
.jpg)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
References
- ↑ Talley NJ, Ford AC (2015). "Functional Dyspepsia". N. Engl. J. Med. 373 (19): 1853–63. doi:10.1056/NEJMra1501505. PMID 26535514.
- ↑ Napthali K, Koloski N, Walker MM, Talley NJ (2016). "Women and functional dyspepsia". Womens Health (Lond). 12 (2): 241–50. doi:10.2217/whe.15.88. PMC 5375052. PMID 26901578.
- ↑ Talley NJ (2016). "Functional dyspepsia: new insights into pathogenesis and therapy". Korean J. Intern. Med. 31 (3): 444–56. doi:10.3904/kjim.2016.091. PMC 4855108. PMID 27048251.
- ↑ Ganesh M, Nurko S (2014). "Functional dyspepsia in children". Pediatr Ann. 43 (4): e101–5. doi:10.3928/00904481-20140325-12. PMID 24716560.
- ↑ Fock KM (2011). "Functional dyspepsia, H. pylori and post infectious FD". J. Gastroenterol. Hepatol. 26 Suppl 3: 39–41. doi:10.1111/j.1440-1746.2011.06649.x. PMID 21443707.
- ↑ Oustamanolakis P, Tack J (2012). "Dyspepsia: organic versus functional". J. Clin. Gastroenterol. 46 (3): 175–90. doi:10.1097/MCG.0b013e318241b335. PMID 22327302.
- ↑ Kindt S, Dubois D, Van Oudenhove L, Caenepeel P, Arts J, Bisschops R, Tack J (2009). "Relationship between symptom pattern, assessed by the PAGI-SYM questionnaire, and gastric sensorimotor dysfunction in functional dyspepsia". Neurogastroenterol. Motil. 21 (11): 1183–e105. doi:10.1111/j.1365-2982.2009.01374.x. PMID 19663903.
- ↑ Pasricha PJ, Grover M, Yates KP, Abell TL, Bernard CE, Koch KL; et al. (2021). "Functional Dyspepsia and Gastroparesis in Tertiary Care are Interchangeable Syndromes With Common Clinical and Pathologic Features". Gastroenterology. 160 (6): 2006–2017. doi:10.1053/j.gastro.2021.01.230. PMID 33548234 Check
|pmid=value (help). - ↑ Miwa H (2012). "Why dyspepsia can occur without organic disease: pathogenesis and management of functional dyspepsia". J Gastroenterol. doi:10.1007/s00535-012-0625-9. PMID 22766746. Unknown parameter
|month=ignored (help) - ↑ "ATLAS OF PATHOLOGY". Retrieved 2007-08-26.