Thyroid gland: Difference between revisions
m (Thyroid Gland moved to Thyroid gland over redirect) |
|||
| Line 17: | Line 17: | ||
===Embryologic development=== | ===Embryologic development=== | ||
[[Image:Gray42.png|thumb|left|Floor of pharynx of embryo between 18 and 21 days.]] | [[Image:Gray42.png|thumb|left|160|Floor of pharynx of embryo between 18 and 21 days.]] | ||
The thyroid is derived from the third [[branchial pouch]]. In the fetus, at 3-4 weeks of gestation, the thyroid gland appears as an epithelial proliferation in the floor of the pharynx at the base of the tongue between the [[tuberculum impar]] and the [[copula linguae]] at a point latter indicated by the [[foramen cecum]]. Subsequently the thyroid descends in front of the pharyngeal gut as a bilobed diverticulum through the [[thyroglossal duct]]. Over the next few weeks, it migrates to the base of the neck. During migration, the thyroid remains connected to the tongue by a narrow canal, the [[thyroglossal duct]]. | The thyroid is derived from the third [[branchial pouch]]. In the fetus, at 3-4 weeks of gestation, the thyroid gland appears as an epithelial proliferation in the floor of the pharynx at the base of the tongue between the [[tuberculum impar]] and the [[copula linguae]] at a point latter indicated by the [[foramen cecum]]. Subsequently the thyroid descends in front of the pharyngeal gut as a bilobed diverticulum through the [[thyroglossal duct]]. Over the next few weeks, it migrates to the base of the neck. During migration, the thyroid remains connected to the tongue by a narrow canal, the [[thyroglossal duct]]. | ||
Revision as of 23:54, 15 January 2009
|
WikiDoc Resources for Thyroid gland |
|
Articles |
|---|
|
Most recent articles on Thyroid gland Most cited articles on Thyroid gland |
|
Media |
|
Powerpoint slides on Thyroid gland |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Thyroid gland at Clinical Trials.gov Trial results on Thyroid gland Clinical Trials on Thyroid gland at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Thyroid gland NICE Guidance on Thyroid gland
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Thyroid gland Discussion groups on Thyroid gland Patient Handouts on Thyroid gland Directions to Hospitals Treating Thyroid gland Risk calculators and risk factors for Thyroid gland
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Thyroid gland |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [2] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Overview
The thyroid is one of the largest endocrine glands in the body. This gland is found in the neck just below the Adam's apple. The thyroid controls how quickly the body burns energy, makes proteins, and how sensitive the body should be to other hormones.
The thyroid participates in these processes by producing thyroid hormones, principally thyroxine (T4) and triiodothyronine (T3). These hormones regulate the rate of metabolism and affect the growth and rate of function of many other systems in the body. Iodine is an essential component of both T3 and T4. The thyroid also produces the hormone calcitonin, which plays a role in calcium homeostasis.
The thyroid is controlled by the hypothalamus and pituitary. The gland gets its name from the Greek word for "shield", after its shape, a double-lobed structure. Hyperthyroidism (overactive thyroid) and hypothyroidism (underactive thyroid) are the most common problems of the thyroid gland. Specialists are called Thyroidologists.
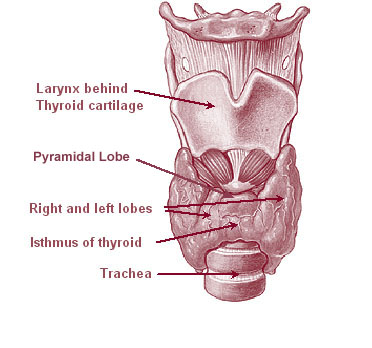
Anatomy
The thyroid is situated on the anterior side of the neck, starting at the oblique line on the thyroid cartilage (just below the laryngeal prominence or Adam's apple), and extending to the 6th Tracheal ring (C-shaped cartilagenous ring of the trachea). It is inappropriate to demarcate the gland's upper and lower border with vertebral levels as it moves position in relation to these during swallowing. It lies over the trachea and is covered by layers of pretracheal fascia (allowing it to move), muscle and skin.
The thyroid is one of the larger endocrine glands - 10-20 grams in adults - and butterfly-shaped. The wings correspond to the lobes and the body to the isthmus of the thyroid. The isthmus overlies tracheal rings 2, 3 and 4. The thyroid may enlarge substantially during pregnancy and when affected by a variety of diseases.
Embryologic development

The thyroid is derived from the third branchial pouch. In the fetus, at 3-4 weeks of gestation, the thyroid gland appears as an epithelial proliferation in the floor of the pharynx at the base of the tongue between the tuberculum impar and the copula linguae at a point latter indicated by the foramen cecum. Subsequently the thyroid descends in front of the pharyngeal gut as a bilobed diverticulum through the thyroglossal duct. Over the next few weeks, it migrates to the base of the neck. During migration, the thyroid remains connected to the tongue by a narrow canal, the thyroglossal duct.
Follicles of the thyroid begin to make colloid in the 11th week and thyroxine by the 18th week.
Histology
At a histological level, there are three primary features of the thyroid:
| Feature | Description |
| Follicles | The thyroid is composed of spherical follicles that selectively absorb iodine (as iodide ions, I-) from the blood for production of thyroid hormones. Twenty-five percent of all the body's iodide ions are in the thyroid gland. Inside the follicles, colloids rich in a protein called thyroglobulin serve as a reservoir of materials for thyroid hormone production and, to a lesser extent, act as a reservoir for the hormones themselves. |
| Thyroid epithelial cells (or "follicular cells") |
The follicles are surrounded by a single layer of thyroid epithelial cells, which secrete T3 and T4. |
| Parafollicular cells (or "C cells") |
Scattered among follicular cells and in spaces between the spherical follicles are another type of thyroid cell, parafollicular cells, which secrete calcitonin. |
Physiology
The primary function of the thyroid is production of the hormones thyroxine (T4), triiodothyronine (T3), and calcitonin. Up to 80% of the T4 is converted to T3 by peripheral organs such as the liver, kidney and spleen. T3 is about ten times more active than T4.[1]
T3 and T4 production and action
Thyroxine is synthesised by the follicular cells from free tyrosine and on the tyrosine residues of the protein called thyroglobulin (TG). Iodine is captured with the "iodine trap" by the hydrogen peroxide generated by the enzyme thyroid peroxidase (TPO)[2] and linked to the 3' and 5' sites of the benzene ring of the tyrosine residues on TG, and on free tyrosine. Upon stimulation by the thyroid-stimulating hormone (TSH), the follicular cells reabsorb TG and proteolytically cleave the iodinated tyrosines from TG, forming T4 and T3 (in T3, one iodine is absent compared to T4), and releasing them into the blood. Deiodinase enzymes convert T4 to T3.[3] Thyroid hormone that is secreted from the gland is about 90% T4 and about 10% T3.[1]
Cells of the brain are a major target for the thyroid hormones T3 and T4. Thyroid hormones play a particularly crucial role in brain development during pregnancy.[4] A transport protein (OATP1C1) has been identified that seems to be important for T4 transport across the blood brain barrier.[5] A second transport protein (MCT8) is important for T3 transport across brain cell membranes.[5]
In the blood, T4 and T3 are partially bound to thyroxine-binding globulin, transthyretin and albumin. Only a very small fraction of the circulating hormone is free (unbound) - T4 0.03% and T3 0.3%. Only the free fraction has hormonal activity. As with the steroid hormones and retinoic acid, thyroid hormones cross the cell membrane and bind to intracellular receptors (α1, α2, β1 and β2), which act alone, in pairs or together with the retinoid X-receptor as transcription factors to modulate DNA transcription[3].
T3 and T4 regulation
The production of thyroxine and triiodothyronine is regulated by thyroid-stimulating hormone (TSH), released by the anterior pituitary. The thyroid and thyrotropes form a negative feedback loop: TSH production is suppressed when the T4 levels are high, and vice versa. The TSH production itself is modulated by thyrotropin-releasing hormone (TRH), which is produced by the hypothalamus and secreted at an increased rate in situations such as cold (in which an accelerated metabolism would generate more heat). TSH production is blunted by somatostatin (SRIH), rising levels of glucocorticoids and sex hormones (estrogen and testosterone), and excessively high blood iodide concentration.
Calcitonin
An additional hormone produced by the thyroid contributes to the regulation of blood calcium levels. Parafollicular cells produce calcitonin in response to hypercalcemia. Calcitonin stimulates movement of calcium into bone, in opposition to the effects of parathyroid hormone (PTH). However, calcitonin seems far less essential than PTH, as calcium metabolism remains clinically normal after removal of the thyroid, but not the parathyroids.
It may be used diagnostically as a tumor marker for a form of thyroid cancer (medullary thyroid adenocarcinoma), in which high calcitonin levels may be present and elevated levels after surgery may indicate recurrence. It may even be used on biopsy samples from suspicious lesions (e.g. swollen lymph nodes) to establish whether they are metastasis of the original cancer.
Calcitonin can be used therapeutically for the treatment of hypercalcemia or osteoporosis.
Significance of iodine
In areas of the world where iodine (essential for the production of thyroxine, which contains four iodine atoms) is lacking in the diet, the thyroid gland can be considerably enlarged, resulting in the swollen necks of endemic goitre.
Thyroxine is critical to the regulation of metabolism and growth throughout the animal kingdom. Among amphibians, for example, administering a thyroid-blocking agent such as propylthiouracil (PTU) can prevent tadpoles from metamorphosing into frogs; conversely, administering thyroxine will trigger metamorphosis.
In humans, children born with thyroid hormone deficiency will have physical growth and development problems, and brain development can also be severely impaired, in the condition referred to as cretinism. Newborn children in many developed countries are now routinely tested for thyroid hormone deficiency as part of newborn screening by analysis of a drop of blood. Children with thyroid hormone deficiency are treated by supplementation with synthetic thyroxine, which enables them to grow and develop normally.
Because of the thyroid's selective uptake and concentration of what is a fairly rare element, it is sensitive to the effects of various radioactive isotopes of iodine produced by nuclear fission. In the event of large accidental releases of such material into the environment, the uptake of radioactive iodine isotopes by the thyroid can, in theory, be blocked by saturating the uptake mechanism with a large surplus of non-radioactive iodine, taken in the form of potassium iodide tablets. While biological researchers making compounds labelled with iodine isotopes do this, in the wider world such preventive measures are usually not stockpiled before an accident, nor are they distributed adequately afterward. One consequence of the Chernobyl disaster was an increase in thyroid cancers in children in the years following the accident. [4]
The use of iodised salt is an efficient way to add iodine to the diet. It has eliminated endemic cretinism in most developed countries, and some governments have made the iodination of flour mandatory. Potassium iodide and Sodium iodide are the most active forms of supplemental iodine.
Diseases
Hyper- and hypofunction (affects about 2% of the population)
- Hypothyroidism (underactivity)
- Hashimoto's thyroiditis / thyroiditis
- Ord's thyroiditis
- Postoperative hypothyroidism
- Postpartum thyroiditis
- Silent thyroiditis
- Acute thyroiditis
- Iatrogenic hypothyroidism
- Hyperthyroidism (overactivity)
- Thyroid storm
- Graves-Basedow disease
- Toxic thyroid nodule
- Toxic nodular struma (Plummer's disease)
- Hashitoxicosis
- Iatrogenic hyperthyroidism
- De Quervain thyroiditis (inflammation starting as hyperthyroidism, can end as hypothyroidism)
Anatomical problems
- Goitre
- Lingual thyroid
- Thyroglossal duct cyst
Tumors
- Thyroid adenoma
- Thyroid cancer
- Papillary
- Follicular
- Medullary
- Anaplastic
- Lymphomas and metastasis from elsewhere (rare)
Deficiencies
Medication linked to thyroid disease includes amiodarone, lithium salts, some types of interferon and IL-2.
Diagnosis
Blood tests
- The measurement of thyroid-stimulating hormone (TSH) levels is often used by doctors as a screening test. Elevated TSH levels can signify an inadequate hormone production, while suppressed levels can point at excessive unregulated production of hormone.
- If TSH is abnormal, decreased levels of thyroid hormones T4 and T3 may be present; these may be determined to confirm this.
- Autoantibodies may be detected in various disease states (anti-TG, anti-TPO, TSH receptor stimulating antibodies).
- There are two cancer markers for thyroid derived cancers. Thyroglobulin (TG) for well differentiated papillary or follcular adenocarcinoma, and the rare medullary thyroid cancer has calcitonin as the marker.
- Very infrequently, TBG and transthyretin levels may be abnormal; these are not routinely tested.
Ultrasound
Nodules of the thyroid may or may not be cancer. Medical ultrasonography can help determine their nature because some of the characteristics of benign and malignant nodules differ. The main characteristics of a thyroid nodule on high frequency thyroid ultrasound are as follows:
| Possible cancer | Benign characteristics |
| irregular border | smooth borders |
| hypoechoic (less echogenic than the surrounding tissue) | hyperechoic |
| microcalcifications | - |
| taller than wide shape on transverse study | - |
| significant intranodular blood flow by power Doppler | - |
| - | "comet tail" artifact as sound waves bounce off intranodular colloid |
Ultrasonography is not always able to separate benign from malignant nodules with complete certainty. In suspicious cases, a tissue sample is often obtained by biopsy for microscopic examination.
Radioiodine scanning and uptake
Thyroid scintigraphy, imaging of the thyroid with the aid of radioactive iodine, usually iodine-123 (123I), is performed in the nuclear medicine department of a hospital or clinic. Radioiodine collects in the thyroid gland before being excreted in the urine. While in the thyroid the radioactive emissions can be detected by a camera, producing a rough image of the shape (a radiodine scan) and tissue activity (a radioiodine uptake) of the thyroid gland.
A normal radioiodine scan shows even uptake and activity throughout the gland. Irregularity can reflect an abnormally shaped or abnormally located gland, or it can indicate that a portion of the gland is overactive or underactive, different from the rest. For example, a nodule that is overactive ("hot") to the point of suppressing the activity of the rest of the gland is usually a thyrotoxic adenoma, a surgically curable form of hyperthyroidism that is hardly ever malignant. In contrast, finding that a substantial section of the thyroid is inactive ("cold") may indicate an area of non-functioning tissue such as thyroid cancer.
The amount of radioactivity can be counted as an indicator of the metabolic activity of the gland. A normal quantitation of radioiodine uptake demonstrates that about 8 to 35% of the administered dose can be detected in the thyroid 24 hours later. Overactivity or underactivity of the gland as may occur with hypothyroidism or hyperthyroidism is usually reflected in decreased or increased radioiondine uptake. Different patterns may occur with different causes of hypo- or hyperthyroidism.
Biopsy
A medical biopsy refers to the obtaining of a tissue sample for examination under the microscope or other testing, usually to distinguish cancer from noncancerous conditions. Thyroid tissue may be obtained for biopsy by fine needle aspiration or by surgery.
Needle aspiration has the advantage of being a brief, safe, outpatient procedure that is safer and less expensive than surgery and does not leave a visible scar. Needle biopsies became widely used in the 1980s, but it was recognized that accuracy of identification of cancer was good but not perfect. The accuracy of the diagnosis depends on obtaining tissue from all of the suspicious areas of an abnormal thyroid gland. The reliability of needle aspiration is increased when sampling can be guided by ultrasound, and over the last 15 years, this has become the preferred method for thyroid biopsy in North America.
Treatment
Medical treatment
Levothyroxine is a stereoisomer of thyroxine which is degraded much slower and can be administered once daily in patients with hypothyroidism.
Graves' disease may be treated with the thioamide drugs propylthiouracil, carbimazole or methimazole, or rarely with Lugol's solution. Hyperthyroidism as well as thyroid tumors may be treated with radioactive iodine.
Percutaneous Ethanol Injections, PEI, for therapy of recurrent thyroid cysts, and metastatic thyroid cancer lymph nodes, as an alternative to the usual surgical method.
Surgery
Thyroid surgery is performed for a variety of reasons. A nodule or lobe of the thyroid is sometimes removed for biopsy or for the presence of an autonomously functioning adenoma causing hyperthyroidism. A large majority of the thyroid may be removed, a subtotal thyroidectomy, to treat the hyperthyroidism of Graves' disease, or to remove a goitre that is unsightly or impinges on vital structures. A complete thyroidectomy of the entire thyroid, including associated lymph nodes, is the preferred treatment for thyroid cancer. Removal of the bulk of the thyroid gland usually produces hypothyroidism, unless the person takes thyroid hormone replacement.
If the thyroid gland must be removed surgically, care must be taken to avoid damage to adjacent structures, the parathyroid glands and the recurrent laryngeal nerve. Both are susceptible to accidental removal and/or injury during thyroid surgery. The parathyroid glands produce parathyroid hormone (PTH), a hormone needed to maintain adequate amounts of calcium in the blood. Removal results in hypoparathyroidism and a need for supplemental calcium and vitamin D each day. The recurrent laryngeal nerves provide motor control for all external muscles of the larynx except for the cricothyroid muscle, also runs along the posterior thyroid. Accidental laceration of either of the two or both recurrent laryngeal nerves may cause paralysis of the vocal cords and their associated muscles, changing the voice quality.
Radioiodine therapy
Large goiters that cause symptoms, but do not harbor cancer, after evaluation, and biopsy of suspicious nodules can be treated by an alternative therapy with radioiodine. The iodine uptake can be high in countries with iodine deficiency, but low in iodine sufficient countries. The 1999 release of rhTSH thyrogen in the USA, can boost the uptakes to 50-60% allowing the therapy with iodine 131. The gland shrinks by 50-60%, but can cause hypothyroidism, and rarely pain syndrome cause by radiation thyroiditis that is short lived and treated by steroids.
History
There are several findings that evidence a great interest for thyroid disorders just in the Medieval Medical School of Salerno (XII Century). Rogerius Salernitanus, the Salernitan surgeon and author of "Post mundi fabricam" (around 1180) was considered at that time the surgical text par excellence all over Europe. In the chapter "De bocio" of his magnus opum he describes several pharmacological and surgical cures, some of which nowadays are reappraised quite scientifically effective.[6]
In modern times, the thyroid was first identified by the anatomist Thomas Wharton (whose name is also eponymised in Wharton's duct of the submandibular gland) in 1656.[7]
Thyroid hormone (or thyroxin) was only identified in the 19th century.
Additional images
-
-
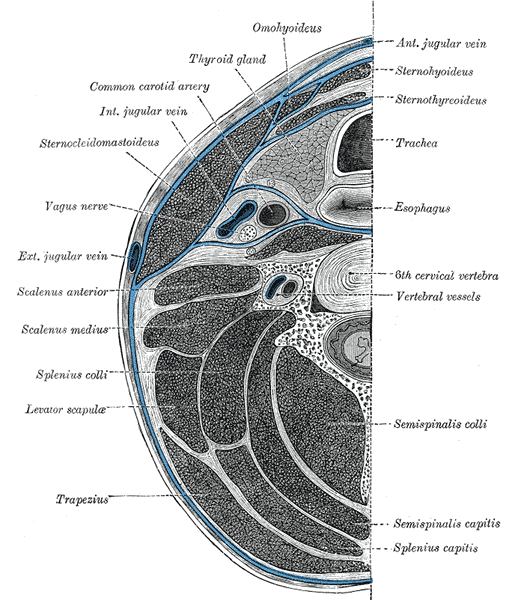
Section of the neck at about the level of the sixth cervical vertebra.
-
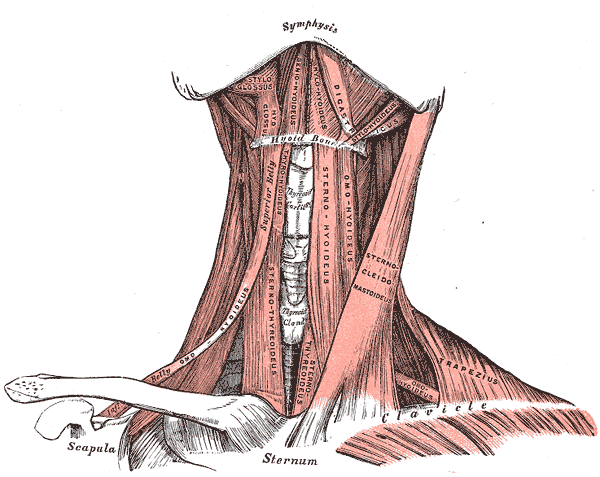
Muscles of the neck. Anterior view.
-
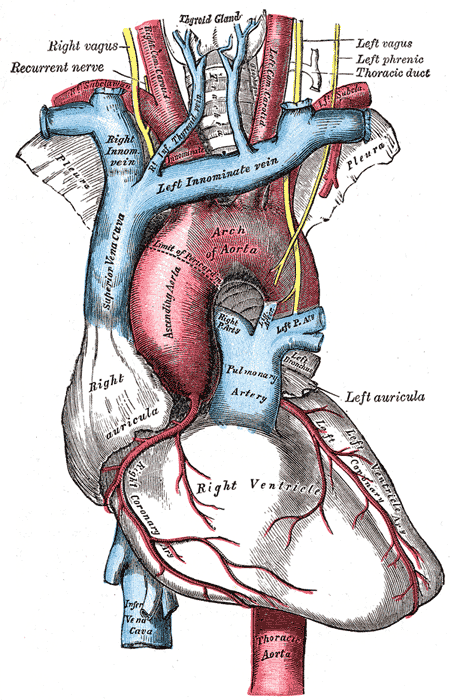
The arch of the aorta, and its branches.
-
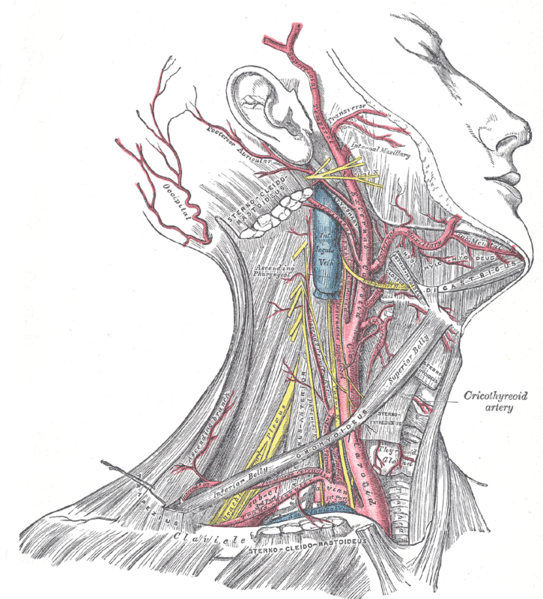
Superficial dissection of the right side of the neck, showing the carotid and subclavian arteries.
-
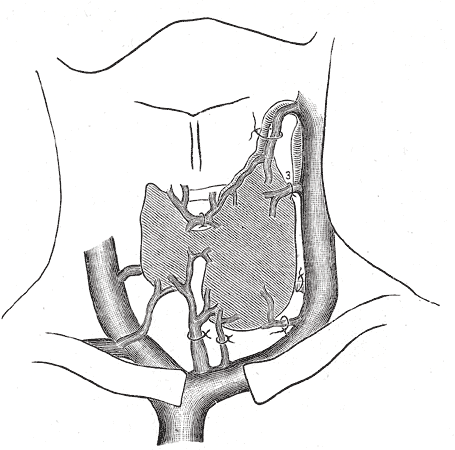
Diagram showing common arrangement of thyroid veins.
-
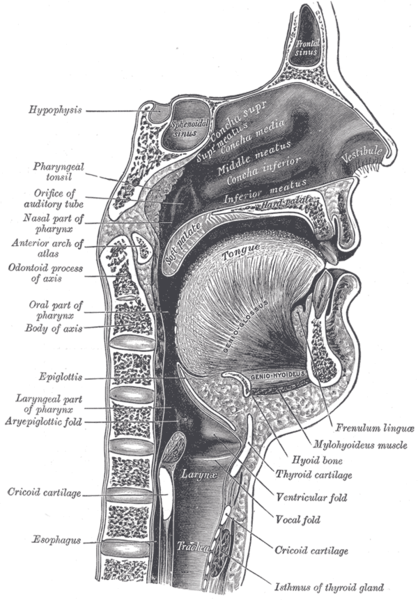
Sagittal section of nose mouth, pharynx, and larynx.
-
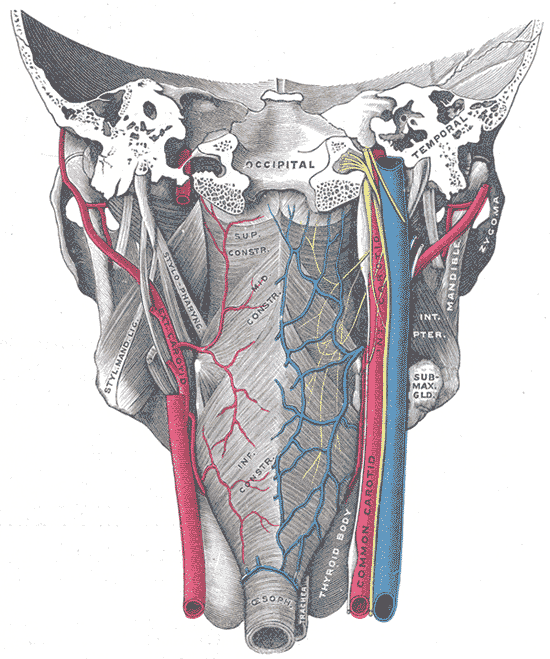
Muscles of the pharynx, viewed from behind, together with the associated vessels and nerves.
-
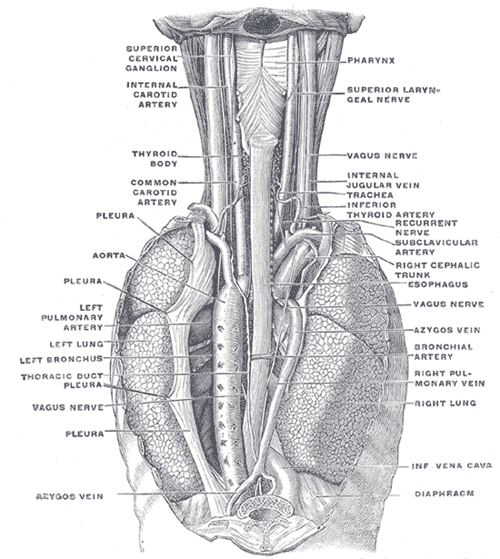
The position and relation of the esophagus in the cervical region and in the posterior mediastinum. Seen from behind.
-
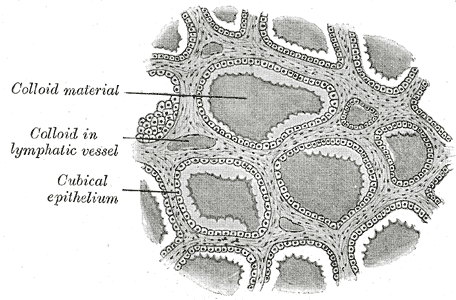
Section of thyroid gland of sheep. X 160.
-

The thymus of a full-term fetus, exposed in situ.
-
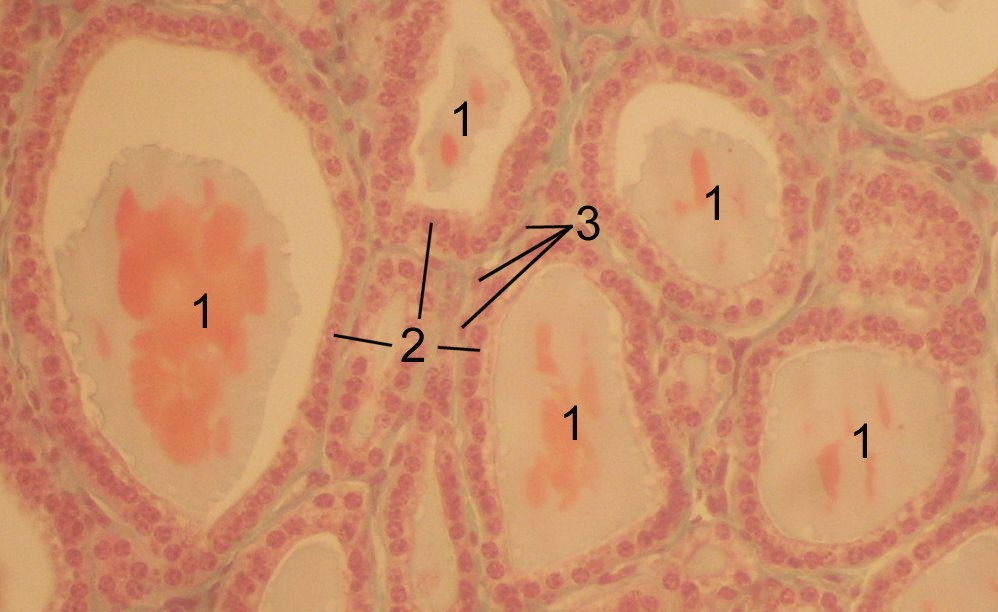
Thyoid histology












See also
References
- ↑ 1.0 1.1 The thyroid gland in Endocrinology: An Integrated Approach by Stephen Nussey and Saffron Whitehead (2001) Published by BIOS Scientific Publishers Ltd. ISBN 1-85996-252-1 .
- ↑ Ekholm R, Bjorkman U (1997). "Glutathione peroxidase degrades intracellular hydrogen peroxide and thereby inhibits intracellular protein iodination in thyroid epithelium". Endocrinology. 138 (7): 2871–2878. PMID 9202230.
- ↑ Bianco AC, Salvatore D, Gereben B, Berry MJ, Larsen PR (2002). "Biochemistry, cellular and molecular biology, and physiological roles of the iodothyronine selenodeiodinases". Endocr Rev. 23 (1): 38–89. PMID 11844744.
- ↑ Kester MH, Martinez de Mena R, Obregon MJ, Marinkovic D, Howatson A, Visser TJ, Hume R, Morreale de Escobar G (2004). "Iodothyronine levels in the human developing brain: major regulatory roles of iodothyronine deiodinases in different areas". J Clin Endocrinol Metab. 89 (7): 3117–3128. PMID 15240580.
- ↑ 5.0 5.1 Jansen J, Friesema ECH, Milici C, Visser TJ (2005). Thyroid hormone transporters in health and disease. Thyroid 15;757-768. PMID 16131319.
- ↑ Bifulco M, Cavallo P. Thyroidology in the medieval medical school of salerno. Thyroid 2007;17:39-40. PMID 17274747.
- ↑ Template:WhoNamedIt
External links
- American Thyroid Association (Thyroid Information and professional organization)
- Histology at KUMC epithel-epith03 "Thyroid Gland"
- New Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer from the American Thyroid Association Taskforce.
- Thyroid Disease Manager (free online textbook)
- Thyroid Disease (Nuclear Medicine Information)
- The Thyroid Foundation of America (Education about Thyroid Disease)
Acknowledgements
The content on this page was first contributed by: C. Michael Gibson, M.S., M.D.
Initial content for this page in some instances came from Wikipedia
List of contributors:
Suggested Reading and Key General References
Suggested Links and Web Resources
For Patients
ar:غدة درقية
cs:Štítná žláza
de:Schilddrüse
eu:Tiroide
fi:Kilpirauhanen
he:בלוטת התריס
hr:Štitna žlijezda
it:Tiroide
la:Glandula thyreoidea
lv:Vairogdziedzeris
lt:Skydliaukė
mk:Штитна жлезда
nl:Schildklier
no:Skjoldbruskkjertel
sk:Štítna žľaza
sr:Штитаста жлезда
sv:Sköldkörtel
th:ต่อมไทรอยด์
yi:טיירויד
Template:SIB