Scabies
Template:DiseaseDisorder infobox
For patient information click here
|
WikiDoc Resources for Scabies |
|
Articles |
|---|
|
Most recent articles on Scabies |
|
Media |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Scabies at Clinical Trials.gov Clinical Trials on Scabies at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Scabies
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Directions to Hospitals Treating Scabies Risk calculators and risk factors for Scabies
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Scabies |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2], Dima Nimri, M.D. [3]
Synonyms and keywords: Norwegian scabies
Overview
Historical Perspective
Classification
Scabies can be divided into 2 major types depending on the resultant skin lesions:[1][2][3][4][5][6][7][8]
| Type of Scabies | Number of mites | Age Group | Associated Conditions | Characteristic Lesion | Areas of Predilection | Itching | Complications |
|---|---|---|---|---|---|---|---|
| Typical Infestation | Usually less than 100 | Mostly children and adolescents | Patients are usually healthy | Papules, which can progress to vesicles and bullae | Intense | Secondary bacterial infection of the skin and soft tissues | |
| Crusted Scabies (Scabies Crustosa, Norwegian Scabies, Keratotic Scabies) | Typically thousands | Mostly elderly |
|
Exfoliating scales and crusts, which can become warty | Minimal or absent | Sepsis |
Pathophysiology
Pathogenesis
Microscopic Pathology
The histopathology of scabies consists of mites being surrounded by an inflammatory infiltrate of eosinophils, lymphocytes and histiocytes.[1][9][10]
Causes
The cause of scabies infection is Sarcoptes scabiei.[11] For more information about the causative organism, click here.
Differentiating Scabies from Other Diseases
Scabies must be differentiated from the following pathologies:[1][12][13][14][15][16][17][18]
| Disease | Skin Lesions | Crusting | Itching | Age Group |
|---|---|---|---|---|
| Eczema | ✔ | |||
| Tinea | ||||
| Atopic dermatitis | ||||
| SLE | ||||
| Bullous pemphigoid | ✔ | |||
| Langerhans cell histiocytosis | ✔ | |||
| Urticaria pigmentosa | ||||
| Seborrheic dermatitis | ✔ | |||
| Psoriasis | ✔ | |||
| Pyoderma without scabies | ✔ |
Epidemiology and Demographics
Epidemiology
Prevalence
The following data exists on the prevalence of scabies around the world:[11]
- The prevalence of scabies worldwide varies greatly; it ranges from 200 to 71,400 per 100,00 cases.
- All regions had a prevalence of more than 10,000 per 100,000 cases, except in Europe and the Middle East.
- It is estimated that there are 100 million cases of scabies worldwide.
Demographics
Age
Scabies is more common in children and adolescents than adults.[19][20][21][22]
Region
- The Pacific and Latin America have the highest prevalence of scabies worldwide, while it is the lowest in Europe and the Middle East.[11]
Risk Factors
The following are believed to be risk factors for scabies:[11][1][23][24][25][26][27][28][19]
- Living in high-risk areas, such as Sub-Saharan Africa and indigenous communities in Australia and New Zealand
- Living in crowded areas
- Homeless or displaced children
- Poor hygiene: the role of poor hygiene in the development of scabies is uncertain, as mites burrowed under the skin remain alive even after daily hot baths and are usually resistant to water and soap
- Immunocompromised individuals, such as the elderly, malnourished and those with HIV, DM are at risk of developing Norwegian Scabies, which is the severe form
Screening
There are no screening recommendations for scabies.[29]
Natural History, Complications and Prognosis
Natural History
Complications
Major complications of scabies include:[11][1][30]
- Secondary bacterial infection of the skin and soft tissue, caused mainly by S. aureus and S. pyogenes, which include:
- Secondary bacterial infection of the skin and soft tissue can progress to life-threatening complications such as:
Prognosis
Diagnosis
History and Symptoms
- In suspected cases of scabies, make sure to enquire about the following:[19]
- History of exposure to a known case of scabies or coming in close contact with patients with a similar complaint (mainly itching)
- In the case of children, ask about daycare attendance
- History of hospitalization
- Recent travel history
- The main symptoms in patients with scabies include:
Physical Examination
In patients with scabies, skin should be carefully examined to look for:[1][11][31][32][28][33][34][19]
- Burrows: are the tunnels which the female mite penetrates into the skin. Initially, they are not clinically visible and can only be seen several days later, when the host immune system forms a local reaction around the tunnel. Burrows are characterized by short, wavy lines.
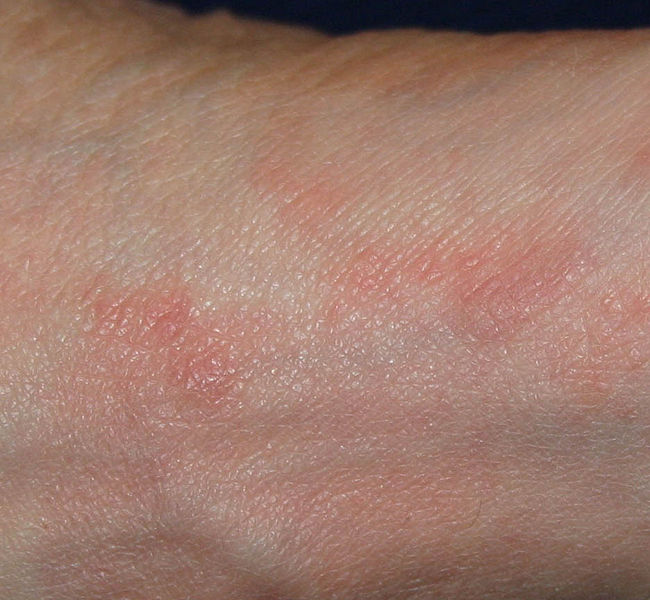
- Papules: they are usually small and erythematous. The distribution of the papules is variable; they can be sparse or very close to each other. Over the course of the infection, papules can transform into vesicles and/or bullae. Characteristic distribution of scabies usually involves the web spaces of fingers and toes, the wrists and areolae of breasts in females and penis in males. The back is usually spared, while face and neck involvement are usually only seen in infants and children.
- Excoriations: skin excoriations are commonly seen in patients with scabies, due to the intense itching associated with the infection.
Skin
-

-
-

-

-

-
![Scabies (common location in ventral wrist) [35]](/images/7/75/Scabies_%28common_location_is_ventral_wrist%29.jpg)
Scabies (common location in ventral wrist) [35]





![Scabies (common location in ventral wrist) [35]](/index.php/File:Scabies_(common_location_is_ventral_wrist).jpg)
Ears

Extremities
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/b/b2/Norwegian_scabies25.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/1/15/Norwegian_scabies26.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/9/92/Norwegian_scabies41.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/7/73/Norwegian_scabies42.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/e/ef/Norwegian_scabies43.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/e/e3/Norwegian_scabies44.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/2/25/Norwegian_scabies45.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/4/4c/Norwegian_scabies01.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/8/83/Norwegian_scabies02.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/4/48/Norwegian_scabies15.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/2/2a/Norwegian_scabies16.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/9/94/Norwegian_scabies21.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-

-

![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies25.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies26.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies41.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies42.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies43.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies44.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies45.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies01.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies02.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies15.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies16.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies21.jpg)


Trunk
-

-

-

-

-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/b/bd/Norwegian_scabies08.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/6/61/Norwegian_scabies09.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]
-
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/images/e/e8/Norwegian_scabies10.jpg)
Norwegian scabies. Adapted from Dermatology Atlas.[36]




![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies08.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies09.jpg)
![Norwegian scabies. Adapted from Dermatology Atlas.[36]](/index.php/File:Norwegian_scabies10.jpg)
Genitales






Laboratory Findings
- Serologic testing for Sarcoptes scabiei has a very high sensitivity and specificity.[19][37]
- Peripheral IgE levels are elevated in patients with Norwegian Scabies.[9][10]
Other Diagnostic Studies
Light Microscopy
The gold standard for diagnosis of scabies infection is visualization of the ova, feces or the mite itself on light microscopy.[19][38][39]
Skin Biopsy
Skin biopsy is another means for diagnosing scabies. Visualization of the mites in the stratum corneum layer of the skin confirms the diagnosis.[19]
Treatment
Medical Therapy
Medical therapy in patients with scabies consists of antimicrobial therapy, mainly either with topical permethrin or oral ivermectin. Patients may experience worsening pruritus and erythema early during the administration of antimicrobial therapy. However, the parasite is gradually eliminated during the body's natural shedding process. The following summarizes the preferred antimicrobial regimens in the treatment of scabies:[40][19][38][41][1][42][43][44]
- Antimicrobial therapy
- 1. Adult
- Preferred regimen (1): Permethrin 5% cream applied to all areas of the body from the neck down and washed off after 8–14 hours
- Preferred regimen (2): Ivermectin 200 ug/kg given orally, 4 times daily and repeated in 2 weeks
- Alternative regimen: Lindane (1%) 1 oz of lotion or 30 g of cream applied in a thin layer to all areas of the body from the neck down and thoroughly washed off after 8 hours
- Note: Patients may experience worsening pruritus and erythema early during the administration of antimicrobial therapy
- 2. Infants and young children
- Preferred regimen: Permethrin 5% cream applied to all areas of the body from the neck down and washed off after 8–14 hours
- Note: Infants and young children aged< 10 years should not be treated with lindane
- 3. Crusted Scabies
- Preferred regimen: (Topical scabicide 5% topical Benzyl benzoate 5% OR topical Permethrin 5% cream (full-body application to be repeated daily for 7 days then twice weekly until discharge or cure) AND treatment with Ivermectin 200 ug/kg PO on days 1,2,8,9, and 15. Additional Ivermectin treatment on days 22 and 29 might be required for severe cases
- 4.Pregnant or Lactating Women
- Preferred regimen: Permethrin 5% cream applied to all areas of the body from the neck down and washed off after 8–14 hours
Primary Prevention
Secondary Prevention
References
- ↑ 1.0 1.1 1.2 1.3 1.4 1.5 1.6 Heukelbach J, Feldmeier H (2006). "Scabies". Lancet. 367 (9524): 1767–74. doi:10.1016/S0140-6736(06)68772-2. PMID 16731272.
- ↑ Pomares C, Marty P, Delaunay P (2014). "Isolated itching of the genitals". Am. J. Trop. Med. Hyg. 90 (4): 589–90. doi:10.4269/ajtmh.13-0337. PMC 3973496. PMID 24696404.
- ↑ Eshagh K, DeKlotz CM, Friedlander SF (2014). "Infant with a papular eruption localized to the back". JAMA Pediatr. 168 (4): 379–80. doi:10.1001/jamapediatrics.2013.3986. PMID 24710581.
- ↑ Witkowski JA, Parish LC (1984). "Scabies: a cause of generalized urticaria". Cutis. 33 (3): 277–9. PMID 6723363.
- ↑ Chapel TA, Krugel L, Chapel J, Segal A (1981). "Scabies presenting as urticaria". JAMA. 246 (13): 1440–1. PMID 6790738.
- ↑ Kartono F, Lee EW, Lanum D, Pham L, Maibach HI (2007). "Crusted Norwegian scabies in an adult with Langerhans cell histiocytosis: mishaps leading to systemic chemotherapy". Arch Dermatol. 143 (5): 626–8. doi:10.1001/archderm.143.5.626. PMID 17515513.
- ↑ Wong SS, Woo PC, Yuen KY (2005). "Unusual laboratory findings in a case of Norwegian scabies provided a clue to diagnosis". J. Clin. Microbiol. 43 (5): 2542–4. doi:10.1128/JCM.43.5.2542-2544.2005. PMC 1153733. PMID 15872307.
- ↑ Lin S, Farber J, Lado L (2009). "A case report of crusted scabies with methicillin-resistant Staphylococcus aureus bacteremia". J Am Geriatr Soc. 57 (9): 1713–4. doi:10.1111/j.1532-5415.2009.02412.x. PMID 19895437.
- ↑ 9.0 9.1 Roberts LJ, Huffam SE, Walton SF, Currie BJ (2005). "Crusted scabies: clinical and immunological findings in seventy-eight patients and a review of the literature". J. Infect. 50 (5): 375–81. doi:10.1016/j.jinf.2004.08.033. PMID 15907543.
- ↑ 10.0 10.1 Arlian LG, Morgan MS, Estes SA, Walton SF, Kemp DJ, Currie BJ (2004). "Circulating IgE in patients with ordinary and crusted scabies". J. Med. Entomol. 41 (1): 74–7. PMID 14989349.
- ↑ 11.0 11.1 11.2 11.3 11.4 11.5 Romani L, Steer AC, Whitfeld MJ, Kaldor JM (2015). "Prevalence of scabies and impetigo worldwide: a systematic review". Lancet Infect Dis. 15 (8): 960–7. doi:10.1016/S1473-3099(15)00132-2. PMID 26088526.
- ↑ Feldmeier H, Singh Chhatwal G, Guerra H (2005). "Pyoderma, group A streptococci and parasitic skin diseases -- a dangerous relationship". Trop. Med. Int. Health. 10 (8): 713–6. doi:10.1111/j.1365-3156.2005.01457.x. PMID 16045456.
- ↑ Bastian HM, Lindgren AM, Alarcón GS (1997). "Scabies mimicking systemic lupus erythematosus". Am. J. Med. 102 (3): 305–6. doi:10.1016/S0002-9343(99)80272-1. PMID 9217603.
- ↑ Brar BK, Pall A, Gupta RR (2003). "Bullous scabies mimicking bullous pemphigoid". J. Dermatol. 30 (9): 694–6. PMID 14578561.
- ↑ Burch JM, Krol A, Weston WL (2004). "Sarcoptes scabiei infestation misdiagnosed and treated as Langerhans cell histiocytosis". Pediatr Dermatol. 21 (1): 58–62. PMID 14871329.
- ↑ Mauleón-Fernandez C, Sáez-de-Ocariz M, Rodríguez-Jurado R, Durán-McKinster C, Orozco-Covarrubias L, Ruiz-Maldonado R (2005). "Nodular scabies mimicking urticaria pigmentosa in an infant". Clin. Exp. Dermatol. 30 (5): 595–6. doi:10.1111/j.1365-2230.2005.01832.x. PMID 16045712.
- ↑ Duran C, Tamayo L, de la Luz Orozco M, Ruiz-Maldonado R (1993). "Scabies of the scalp mimicking seborrheic dermatitis in immunocompromised patients". Pediatr Dermatol. 10 (2): 136–8. PMID 8346105.
- ↑ Gach JE, Heagerty A (2000). "Crusted scabies looking like psoriasis". Lancet. 356 (9230): 650. PMID 10968439.
- ↑ 19.0 19.1 19.2 19.3 19.4 19.5 19.6 19.7 Anderson KL, Strowd LC (2017). "Epidemiology, Diagnosis, and Treatment of Scabies in a Dermatology Office". J Am Board Fam Med. 30 (1): 78–84. doi:10.3122/jabfm.2017.01.160190. PMID 28062820.
- ↑ Hengge UR, Currie BJ, Jäger G, Lupi O, Schwartz RA (2006). "Scabies: a ubiquitous neglected skin disease". Lancet Infect Dis. 6 (12): 769–79. doi:10.1016/S1473-3099(06)70654-5. PMID 17123897.
- ↑ Hay RJ, Steer AC, Engelman D, Walton S (2012). "Scabies in the developing world--its prevalence, complications, and management". Clin. Microbiol. Infect. 18 (4): 313–23. doi:10.1111/j.1469-0691.2012.03798.x. PMID 22429456.
- ↑ Burkhart CG, Burkhart CN, Burkhart KM (2000). "An epidemiologic and therapeutic reassessment of scabies". Cutis. 65 (4): 233–40. PMID 10795086.
- ↑ Kristensen JK (1991). "Scabies and Pyoderma in Lilongwe, Malawi. Prevalence and seasonal fluctuation". Int. J. Dermatol. 30 (10): 699–702. PMID 1955222.
- ↑ Estrada B (2003). "Ectoparasitic infestations in homeless children". Semin Pediatr Infect Dis. 14 (1): 20–4. doi:10.1053/spid.2003.127213. PMID 12748918.
- ↑ Currie BJ, Connors CM, Krause VL (1994). "Scabies programs in aboriginal communities". Med. J. Aust. 161 (10): 636–7. PMID 7968739.
- ↑ Terry BC, Kanjah F, Sahr F, Kortequee S, Dukulay I, Gbakima AA (2001). "Sarcoptes scabiei infestation among children in a displacement camp in Sierra Leone". Public Health. 115 (3): 208–11. doi:10.1038/sj/ph/1900748. PMID 11429717.
- ↑ Andrews JR, Tonkin SL (1989). "Scabies and pediculosis in Tokelau Island children in New Zealand". J R Soc Health. 109 (6): 199–203. PMID 2513405.
- ↑ 28.0 28.1 Heukelbach J, Wilcke T, Winter B, Feldmeier H (2005). "Epidemiology and morbidity of scabies and pediculosis capitis in resource-poor communities in Brazil". Br. J. Dermatol. 153 (1): 150–6. doi:10.1111/j.1365-2133.2005.06591.x. PMID 16029341.
- ↑ U.S. Preventive Services Task Forces https://www.uspreventiveservicestaskforce.org/BrowseRec/Search?s=scabies. Accessed on Jan 25, 2017.
- ↑ Engelman D, Kiang K, Chosidow O, McCarthy J, Fuller C, Lammie P, Hay R, Steer A (2013). "Toward the global control of human scabies: introducing the International Alliance for the Control of Scabies". PLoS Negl Trop Dis. 7 (8): e2167. doi:10.1371/journal.pntd.0002167. PMC 3738445. PMID 23951369.
- ↑ Chakrabarti A (1985). "Some epidemiological aspects of animal scabies in human population". Int J Zoonoses. 12 (1): 39–52. PMID 4055268.
- ↑ Burgess I (1994). "Sarcoptes scabiei and scabies". Adv. Parasitol. 33: 235–92. PMID 8122567.
- ↑ Steer AC, Jenney AW, Kado J, Batzloff MR, La Vincente S, Waqatakirewa L, Mulholland EK, Carapetis JR (2009). "High burden of impetigo and scabies in a tropical country". PLoS Negl Trop Dis. 3 (6): e467. doi:10.1371/journal.pntd.0000467. PMC 2694270. PMID 19547749.
- ↑ Lawrence G, Leafasia J, Sheridan J, Hills S, Wate J, Wate C, Montgomery J, Pandeya N, Purdie D (2005). "Control of scabies, skin sores and haematuria in children in the Solomon Islands: another role for ivermectin". Bull. World Health Organ. 83 (1): 34–42. doi:/S0042-96862005000100012 Check
|doi=value (help). PMC 2623469. PMID 15682247. - ↑ http://picasaweb.google.com/mcmumbi/USMLEIIImages
- ↑ 36.00 36.01 36.02 36.03 36.04 36.05 36.06 36.07 36.08 36.09 36.10 36.11 36.12 36.13 36.14 "Dermatology Atlas".
- ↑ Jayaraj R, Hales B, Viberg L, Pizzuto S, Holt D, Rolland JM, O'Hehir RE, Currie BJ, Walton SF (2011). "A diagnostic test for scabies: IgE specificity for a recombinant allergen of Sarcoptes scabiei". Diagn. Microbiol. Infect. Dis. 71 (4): 403–7. doi:10.1016/j.diagmicrobio.2011.09.007. PMID 22018936.
- ↑ 38.0 38.1 Johnston G, Sladden M (2005). "Scabies: diagnosis and treatment". BMJ. 331 (7517): 619–22. doi:10.1136/bmj.331.7517.619. PMC 1215558. PMID 16166133.
- ↑ Hicks MI, Elston DM (2009). "Scabies". Dermatol Ther. 22 (4): 279–92. doi:10.1111/j.1529-8019.2009.01243.x. PMID 19580575.
- ↑ Workowski, Kimberly A.; Bolan, Gail A. (2015-06-05). "Sexually transmitted diseases treatment guidelines, 2015". MMWR. Recommendations and reports: Morbidity and mortality weekly report. Recommendations and reports / Centers for Disease Control. 64 (RR-03): 1–137. ISSN 1545-8601. PMID 26042815.
- ↑ Strong M, Johnstone P (2007). "Interventions for treating scabies". Cochrane Database Syst Rev (3): CD000320. doi:10.1002/14651858.CD000320.pub2. PMID 17636630.
- ↑ Thomas J, Peterson GM, Walton SF, Carson CF, Naunton M, Baby KE (2015). "Scabies: an ancient global disease with a need for new therapies". BMC Infect. Dis. 15: 250. doi:10.1186/s12879-015-0983-z. PMC 4487193. PMID 26123073.
- ↑ Goldust M, Rezaee E, Hemayat S (2012). "Treatment of scabies: Comparison of permethrin 5% versus ivermectin". J. Dermatol. 39 (6): 545–7. doi:10.1111/j.1346-8138.2011.01481.x. PMID 22385121.
- ↑ Usha V, Gopalakrishnan Nair TV (2000). "A comparative study of oral ivermectin and topical permethrin cream in the treatment of scabies". J. Am. Acad. Dermatol. 42 (2 Pt 1): 236–40. doi:10.1016/S0190-9622(00)90131-2. PMID 10642678.