Renal artery stenosis: Difference between revisions
Esther Lee (talk | contribs) No edit summary |
Esther Lee (talk | contribs) No edit summary |
||
| Line 34: | Line 34: | ||
==Treatment== | ==Treatment== | ||
[[Renal artery stenosis medical therapy|Medical Therapy]] | [[Renal artery stenosis surgery|Surgery]] | [[Renal artery stenosis primary prevention|Primary Prevention]] | [[Renal artery stenosis secondary prevention|Secondary Prevention]] | [[Renal artery stenosis cost-effectiveness of therapy|Cost-Effectiveness of Therapy]] | [[Renal artery stenosis future or investigational therapies|Future or Investigational Therapies]] | [[Renal artery stenosis medical therapy|Medical Therapy]] | [[Renal artery stenosis angioplasty and stenting|Angioplasty and Stenting]] | [[Renal artery stenosis surgery|Surgery]] | [[Renal artery stenosis primary prevention|Primary Prevention]] | [[Renal artery stenosis secondary prevention|Secondary Prevention]] | [[Renal artery stenosis cost-effectiveness of therapy|Cost-Effectiveness of Therapy]] | [[Renal artery stenosis future or investigational therapies|Future or Investigational Therapies]] | ||
==Case Studies== | ==Case Studies== | ||
Revision as of 15:01, 28 September 2012
| Renal artery stenosis | |
 | |
|---|---|
| Renal artery is #3 | |
| ICD-9 | 440.1 |
| DiseasesDB | 11255 |
| MedlinePlus | 001273 |

|
Renal artery stenosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Renal artery stenosis On the Web |
|
American Roentgen Ray Society Images of Renal artery stenosis |
For patient information click here
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Overview
Pathophysiology
Causes
Epidemiology and Demographics
Risk Factors
Diagnosis
Diagnostic Criteria | History and Symptoms | Physical Examination | Laboratory Findings | CT | MRI | Echocardiography or Ultrasound | Other Imaging Findings | Other Diagnostic Studies
Treatment
Medical Therapy | Angioplasty and Stenting | Surgery | Primary Prevention | Secondary Prevention | Cost-Effectiveness of Therapy | Future or Investigational Therapies
Case Studies
Pathophysiology
The macula densa of the kidney senses a decreased systemic blood pressure due to the pressure drop over the stenosis. The response of the kidney to this decreased blood pressure is activation of the renin-angiotension aldosterone system, which normally counteracts low blood pressure, but in this case lead to hypertension (high blood pressure). The decreased perfusion pressure (caused by the stenosis) leads to decreased blood flow (hypoperfusion) to the kidney and a decrease in the GFR. If the stenosis is long standing and severe the GFR in the affected kidneys never increases again and (pre-renal) renal failure is the result.
Signs and symptoms
Most cases of renal artery stenosis are asymptomatic, and the main problem is high blood pressure that cannot be controlled with medication. Deterioration in renal function may develop if both kidneys are poorly supplied, or when treatment with an ACE inhibitor is initiated. Some patients present with episodes of flash pulmonary edema (sudden left ventricular heart failure).[1]
Differential Diagnosis
- Acute renal failure
- Atherosclerosis
- Chronic glomerulonephritis
- Hypersensitivity nephropathy
- Hypertension
- Malignant hypertension
- Nephrosclerosis
- Renovascular hypertension
- Uremia
Diagnosis
A clinical prediction rule is available to guide diagnosis.[2]
- refractory hypertension - high blood pressure that can not be controlled adequately with antihypertensives
- auscultation (with stethoscope) - bruit ("rushing" sound) on affected side, inferior of the costal margin
- captopril challenge test
- captopril test dose effect on the differential renal function as measured by MAG3 scan.[3]
- renal artery arteriogram
Diagnostic Findings
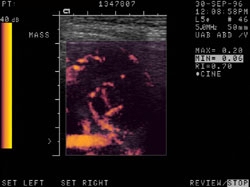
Ultrasonography
-

Abdominal pain in a patient with previous renal transplant. 1) Juxtanephric mass surrounding renal vessels, differential includes adenopathy, hematoma and abscess. 2) Renal artery stenosis of CRT.
-

Abdominal pain in a patient with previous renal transplant. 1) Juxtanephric mass surrounding renal vessels, differential includes adenopathy, hematoma and abscess. 2) Renal artery stenosis of CRT


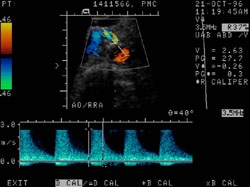
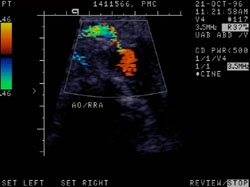
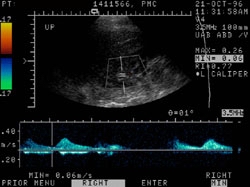
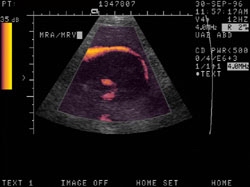
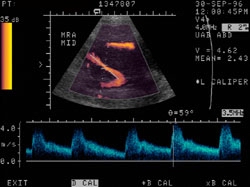
Doppler USG
Case #1
-
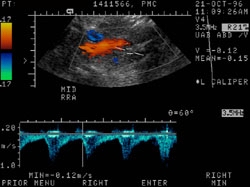
Renal artery stenosis. The patient is a 75 year old white female with a history of hypertension. she is s/p left nephrectomy approximately 10 years ago for renal cell carcinoma. 1. Definite renal artery stenosis involving the origin of the right renal artery. 2. Focal dilatation of the distal abdominal aorta, but no frank aneurysm.
-
Renal artery stenosis. The patient is a 75 year old white female with a history of hypertension. she is s/p left nephrectomy approximately 10 years ago for renal cell carcinoma. 1. Definite renal artery stenosis involving the origin of the right renal artery. 2. Focal dilatation of the distal abdominal aorta, but no frank aneurysm.
-
Renal artery stenosis. The patient is a 75 year old white female with a history of hypertension. she is s/p left nephrectomy approximately 10 years ago for renal cell carcinoma. 1. Definite renal artery stenosis involving the origin of the right renal artery. 2. Focal dilatation of the distal abdominal aorta, but no frank aneurysm.
-
Renal artery stenosis. The patient is a 75 year old white female with a history of hypertension. she is s/p left nephrectomy approximately 10 years ago for renal cell carcinoma. 1. Definite renal artery stenosis involving the origin of the right renal artery. 2. Focal dilatation of the distal abdominal aorta, but no frank aneurysm.




Case #2
-

Abdominal pain in a patient with previous renal transplant. 1) Juxtanephric mass surrounding renal vessels, differential includes adenopathy, hematoma and abscess. 2) Renal artery stenosis of CRT
-
Abdominal pain in a patient with previous renal transplant. 1) Juxtanephric mass surrounding renal vessels, differential includes adenopathy, hematoma and abscess. 2) Renal artery stenosis of CRT
-
Abdominal pain in a patient with previous renal transplant. 1) Juxtanephric mass surrounding renal vessels, differential includes adenopathy, hematoma and abscess. 2) Renal artery stenosis of CRT
-
Abdominal pain in a patient with previous renal transplant. 1) Juxtanephric mass surrounding renal vessels, differential includes adenopathy, hematoma and abscess. 2) Renal artery stenosis of CRT




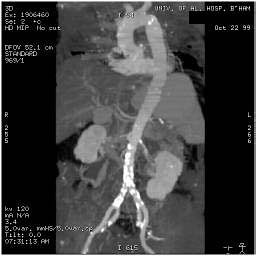
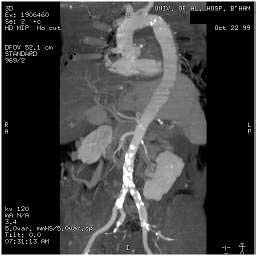
Magnetic Resonance Angiography
Case #1
-
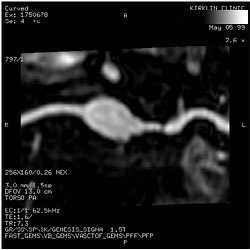
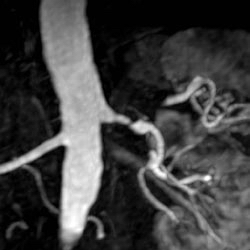
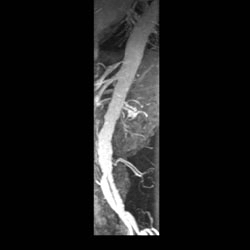
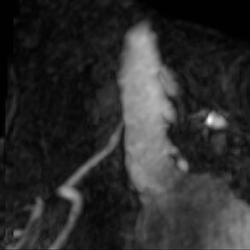
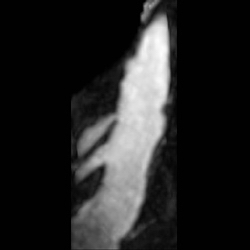
High grade left main renal artery stenosis, MRA. 76 year old male with hypertension.
-
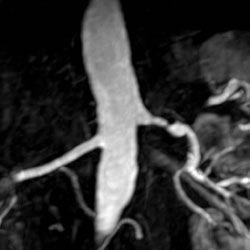
High grade left main renal artery stenosis, MRA. 76 year old male with hypertension.
-
High grade left main renal artery stenosis, MRA. 76 year old male with hypertension.
-

High grade left main renal artery stenosis, MRA. 76 year old male with hypertension.
-

High grade left main renal artery stenosis, MRA. 76 year old male with hypertension.
-

High grade left main renal artery stenosis, MRA. 76 year old male with hypertension.
-
High grade left main renal artery stenosis, MRA. 76 year old male with hypertension.
-

High grade left main renal artery stenosis, MRA. 76 year old male with hypertension.
-

High grade left main renal artery stenosis, MRA. 76 year old male with hypertension.









Case #2
-

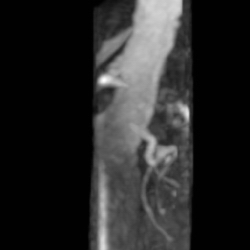
MRA: Renal artery stenosis.
-

MRA: Renal artery stenosis.
-
MRA: Renal artery stenosis.
-
MRA: Renal artery stenosis.
-

MRA: Renal artery stenosis.
-

MRA: Renal artery stenosis.
-

MRA: Renal artery stenosis.
-
MRA: Renal artery stenosis.
-

MRA: Renal artery stenosis.
-
MRA: Renal artery stenosis.










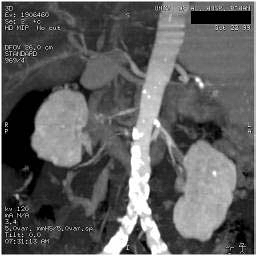
Case #3
-

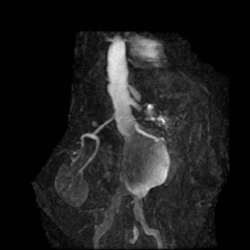
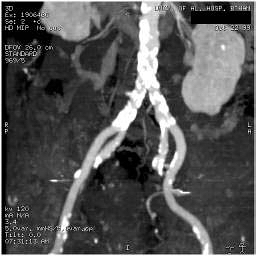
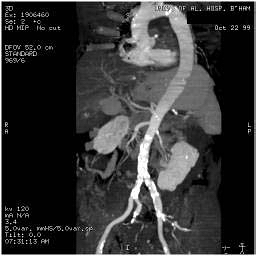
Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-

Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-

Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-

Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-

Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-
Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-

Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-

Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-

Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-
Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-

Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-

Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-
Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-
Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-

Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-
Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-
Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.
-
Atherosclerotic plaques seen in the distal aortic arch, aortic bifurcation, and in the external iliac arteries. right renal artery stenosis. A 74 year-old male who is status post thromboembolic event of his RLE.


















Treatment
When high-grade renal artery stenosis is documented and blood pressure cannot be controlled with medication, or if renal function deteriorates, renal artery stenosis is often treated invasively. Renal artery stenosis is most commonly treated by endovascular techniques (i.e. angioplasty with or without stenting). A 2003 meta-analysis found that angioplasty was safe and effective in this context.[4] There are ongoing clinical trials to compare medical management and angioplasty with stenting to medical management alone. These include CORAL and ASTRAL, both scheduled to report results in 2010. In addition to endovascular treatment, surgical resection and anastomosis is a rarely-used option.
Life Style Modification
The first step in treating RAS is making lifestyle changes that promote healthy blood vessels in general. Exercising, controlling weight, and choosing healthy foods may help to keep arteries disease free and flexible. Smoking cessation is one of the best things to save kidneys and other organs.
Blood Pressure Control
RAS causes high blood pressure, which can damage the kidneys. Damaged kidneys, in turn, can make your blood pressure even higher. If left uncontrolled, this vicious cycle can lead to kidney failure and damage the heart and blood vessels throughout the body.
Controlling renovascular hypertension is often difficult but usually achievable. It may require two or more different kinds of blood pressure medicine. Blood pressure medicines work in different ways.
Sometimes, by combining two or more blood pressure medicines that work in different ways, you may be able to control your blood pressure and stop the progression of kidney failure. Each type of blood pressure medicine has its own potential side effects; therefore, the choice of medicine is best determined by you and your doctor.
In addition to antihypertensives, prescription of a cholesterol lowering drug to prevent the plaques from forming in the arteries, and a blood-thinner, such as aspirin, to help the blood flow more easily through the arteries.
Angioplasty and stenting
Angioplasty is a procedure in which a catheter is put into the renal artery, usually through the groin, just as in a conventional angiogram. In addition, for angioplasty, a tiny balloon at the end of the catheter can be inflated to flatten the plaque against the wall of the artery. Then your doctor may position a small mesh tube, called a stent, to keep plaque flattened and the artery open.
Surgery
If RAS advances until the artery is nearly or completely blocked, the patient may need surgery to open up the flow of blood to the kidney. Different types of surgery for RAS include the following:
Endarterectomy
In an endarterectomy, a vascular surgeon removes the plaque
Bypass surgery
To create a bypass, a vascular surgeon uses a vein or synthetic tube to connect the kidney to the aorta. This new path serves as an alternate route for blood to flow around the blocked artery into the kidney.
Related Chapters
Examples of Renal Artery Stenosis
{{#ev:youtube|xeV3lmYi1Hk}}
- Right Renal Artery Stenosis
{{#ev:youtube|4UzLFatOg1Q}}
- Aortogram of Bilateral Renal Artery Stenosis
{{#ev:youtube|cL1TQFUU2Iw}}
Reference
- ↑ Pickering TG, Herman L, Devereux RB; et al. (1988). "Recurrent pulmonary oedema in hypertension due to bilateral renal artery stenosis: treatment by angioplasty or surgical revascularisation". Lancet. 2 (8610): 551–2. PMID 2900930.
- ↑ Krijnen P, van Jaarsveld BC, Steyerberg EW, Man in 't Veld AJ, Schalekamp MA, Habbema JD (1998). "A clinical prediction rule for renal artery stenosis". Ann. Intern. Med. 129 (9): 705–11. PMID 9841602.
- ↑ Roccatello D, Picciotto G (1997). "Captopril-enhanced scintigraphy using the method of the expected renogram: improved detection of patients with renin-dependent hypertension due to functionally significant renal artery stenosis" (PDF). Nephrol. Dial. Transplant. 12 (10): 2081–6. doi:10.1093/ndt/12.10.2081. PMID 9351069.
- ↑ Nordmann AJ, Woo K, Parkes R, Logan AG (2003). "Balloon angioplasty or medical therapy for hypertensive patients with atherosclerotic renal artery stenosis? A meta-analysis of randomized controlled trials". Am. J. Med. 114 (1): 44–50. PMID 12557864.