Nasopharyngeal angiofibroma: Difference between revisions
No edit summary |
No edit summary |
||
| Line 7: | Line 7: | ||
==Overview== | ==Overview== | ||
'''Nasopharyngeal angiofibroma''' (also called juvenile nasopharyngeal angiofibroma) is a locally aggressive, benign vascular neoplasm that grows in the [[pterygopalatine fossa]]. The most common symptoms of nasopharyngeal angiofibroma include one-sided nasal obstruction and [[Bleeding|recurrent bleeding]]. | '''Nasopharyngeal angiofibroma''' (also called juvenile nasopharyngeal angiofibroma) is a locally aggressive, benign vascular neoplasm that grows in the [[pterygopalatine fossa]]. The most common symptoms of nasopharyngeal angiofibroma include one-sided nasal obstruction and [[Bleeding|recurrent bleeding]]. Nasopharyngeal angiofibroma may be classified according to Radkowski Classification System (severity) into 3 categories: I, II, and III. The majority of nasopharyngeal angiofibromas are irrigated by the external carotid artery. Genetic alterations associated with the development of nasopharyngeal angiofibroma include: overexpression of PDGF-B, bFGF, [[Vascular endothelial growth factor|VEGF]]. Nasopharyngeal angiofibroma accounts for 0.05% of all head and neck tumors. Nasopharyngeal angiofibromas are more commonly observed among children and adolescents. Males are more commonly affected with nasopharyngeal angiofibroma than females. Common risk factors in the development of nasopharyngeal angiofibroma, include: presence of tumor in the [[pterygoid fossa]] and young age. Physical examination may be remarkable for smooth [[submucosal]] mass in the posterior [[nasal cavity]]. Computed tomography is the imaging modality of choice. On conventional radiography, findings of nasopharyngeal angiofibroma include: visualization of a nasopharyngeal mass, opacification of the [[sphenoid sinus]], and anterior bowing of the posterior wall of the maxillary antrum. Surgery is the mainstay of therapy for nasopharyngeal angiofibroma. Surgical approach for nasopharyngeal angiofibroma will usually depend on the stage. The treatment of choice for early stage for nasopharyngeal angiofibroma is intranasal endoscopic surgery ( e.g. lateral rhinotomy). The treatment of choice for late stage nasopharyngeal angiofibroma include the [[infratemporal fossa]] approach, and the mid-facial degloving approach. Common complications of nasopharyngeal angiofibroma include [[Blindness|transient blindness]], optic nerve damage, and [[Consumption coagulopathy|low-grade consumption coagulopathy]]. | ||
==Historical Perspective== | ==Historical Perspective== | ||
| Line 15: | Line 15: | ||
*Nasopharyngeal angiofibroma may be classified according to Radkowski Classification System into 3 categories:<ref name="pmid11374252">{{cite journal |vauthors=Paris J, Guelfucci B, Moulin G, Zanaret M, Triglia JM |title=Diagnosis and treatment of juvenile nasopharyngeal angiofibroma |journal=Eur Arch Otorhinolaryngol |volume=258 |issue=3 |pages=120–4 |year=2001 |pmid=11374252 |doi= |url=}}</ref> | *Nasopharyngeal angiofibroma may be classified according to Radkowski Classification System into 3 categories:<ref name="pmid11374252">{{cite journal |vauthors=Paris J, Guelfucci B, Moulin G, Zanaret M, Triglia JM |title=Diagnosis and treatment of juvenile nasopharyngeal angiofibroma |journal=Eur Arch Otorhinolaryngol |volume=258 |issue=3 |pages=120–4 |year=2001 |pmid=11374252 |doi= |url=}}</ref> | ||
*'''Stage I''' | *'''Stage I''' | ||
:*Ia: limited to nasal cavity/nasopharynx | :*Ia: limited to nasal cavity/[[nasopharynx]] | ||
:*Ib: extension into one or more paranasal sinuses | :*Ib: extension into one or more [[paranasal sinuses]] | ||
*'''Stage II''' | *'''Stage II''' | ||
:*IIa: minimal extension through [[sphenopalatine foramen]] into pterygomaxillary fossa | :*IIa: minimal extension through [[sphenopalatine foramen]] into [[pterygomaxillary fossa]] | ||
:*IIb: fills pterygomaxillary fossa bowing the posterior wall of the maxillary antrum anteriorly or extending into the orbit via the inferior orbital fissure | :*IIb: fills pterygomaxillary fossa bowing the posterior wall of the maxillary antrum anteriorly or extending into the orbit via the inferior orbital fissure | ||
:*IIc: extends beyond pterygomaxillary fossa into infratemporal fossa | :*IIc: extends beyond pterygomaxillary fossa into [[infratemporal fossa]] | ||
*'''Stage III''' | *'''Stage III''' | ||
:*Stage IIIA: intracranial extension | :*Stage IIIA: intracranial extension | ||
| Line 26: | Line 26: | ||
==Pathophysiology== | ==Pathophysiology== | ||
*The pathogenesis of nasopharyngeal angiofibroma is characterized by the following features: | *The pathogenesis of nasopharyngeal angiofibroma is characterized by the following features: | ||
:*Vascular neoplasm | :*Vascular [[neoplasm]] | ||
:*Originates from the pterygopalatine fossa | :*Originates from the pterygopalatine fossa | ||
:*The majority are associated with the [[external carotid artery]] | :*The majority are associated with the [[external carotid artery]] | ||
*Genetic alterations | *Genetic alterations associated with the development of nasopharyngeal angiofibroma include:<ref name="pmid18228521">{{cite journal |vauthors=Coutinho-Camillo CM, Brentani MM, Nagai MA |title=Genetic alterations in juvenile nasopharyngeal angiofibromas |journal=Head Neck |volume=30 |issue=3 |pages=390–400 |year=2008 |pmid=18228521 |doi=10.1002/hed.20775 |url=}}</ref> | ||
:*Overexpression PDGF-B | :*Overexpression PDGF-B | ||
:*Overexpression bFGF | :*Overexpression bFGF | ||
| Line 36: | Line 36: | ||
:*Tumor suppressor gene p53 | :*Tumor suppressor gene p53 | ||
:*Overexpression of Her-2/neu oncogene | :*Overexpression of Her-2/neu oncogene | ||
*On gross pathology, characteristic findings of nasopharyngeal angiofibroma | *On gross pathology, characteristic findings of nasopharyngeal angiofibroma include: | ||
:*Unencapsulated | :*Unencapsulated | ||
:*Polypoid fibrous mass | :*Polypoid fibrous mass | ||
:*Bleeding on manipulation | :*Bleeding on manipulation | ||
*On microscopic histopathological analysis, characteristic findings of nasopharyngeal angiofibroma | *On microscopic histopathological analysis, characteristic findings of nasopharyngeal angiofibroma include: | ||
:*Fibroblastic cells with plump (near cuboidal) nuclei | :*Fibroblastic cells with plump (near cuboidal) nuclei | ||
:*Fibrous stroma | :*Fibrous stroma | ||
| Line 49: | Line 49: | ||
==Differentiating Nasopharyngeal Angiofibroma from Other Diseases== | ==Differentiating Nasopharyngeal Angiofibroma from Other Diseases== | ||
*Nasopharyngeal angiofibroma must be differentiated from other diseases that cause epistaxis, unilateral nasal obstruction, and rhinorrhea, such as: | *Nasopharyngeal angiofibroma must be differentiated from other diseases that cause [[epistaxis]], unilateral nasal obstruction, and [[rhinorrhea]], such as: | ||
:* Antro-choanal polyp | :* Antro-choanal polyp | ||
:* [[Rhinosporidiosis]] | :* [[Rhinosporidiosis]] | ||
| Line 63: | Line 63: | ||
===Age=== | ===Age=== | ||
*Nasopharyngeal angiofibroma is more commonly observed among patients aged 7-19 years.<ref name="pmid11374252">{{cite journal |vauthors=Paris J, Guelfucci B, Moulin G, Zanaret M, Triglia JM |title=Diagnosis and treatment of juvenile nasopharyngeal angiofibroma |journal=Eur Arch Otorhinolaryngol |volume=258 |issue=3 |pages=120–4 |year=2001 |pmid=11374252 |doi= |url=}}</ref> | *Nasopharyngeal angiofibroma is more commonly observed among patients aged 7-19 years.<ref name="pmid11374252">{{cite journal |vauthors=Paris J, Guelfucci B, Moulin G, Zanaret M, Triglia JM |title=Diagnosis and treatment of juvenile nasopharyngeal angiofibroma |journal=Eur Arch Otorhinolaryngol |volume=258 |issue=3 |pages=120–4 |year=2001 |pmid=11374252 |doi= |url=}}</ref> | ||
===Gender=== | ===Gender=== | ||
*The male to female ratio for nasopharyngeal angiofibroma is approximately 4 to 1.<ref name="pmid11374252">{{cite journal |vauthors=Paris J, Guelfucci B, Moulin G, Zanaret M, Triglia JM |title=Diagnosis and treatment of juvenile nasopharyngeal angiofibroma |journal=Eur Arch Otorhinolaryngol |volume=258 |issue=3 |pages=120–4 |year=2001 |pmid=11374252 |doi= |url=}}</ref> | *The male to female ratio for nasopharyngeal angiofibroma is approximately 4 to 1.<ref name="pmid11374252">{{cite journal |vauthors=Paris J, Guelfucci B, Moulin G, Zanaret M, Triglia JM |title=Diagnosis and treatment of juvenile nasopharyngeal angiofibroma |journal=Eur Arch Otorhinolaryngol |volume=258 |issue=3 |pages=120–4 |year=2001 |pmid=11374252 |doi= |url=}}</ref> | ||
| Line 73: | Line 71: | ||
==Risk Factors== | ==Risk Factors== | ||
*Common risk factors in the development of nasopharyngeal angiofibroma | *Common risk factors in the development of nasopharyngeal angiofibroma include: | ||
:*Presence of tumor in the pterygoid fossa | :*Presence of tumor in the [[pterygoid fossa]] | ||
:*Young age | :*Young age | ||
:*Feeders from the internal carotid artery | :*Feeders from the internal carotid artery | ||
| Line 81: | Line 79: | ||
== Natural History, Complications and Prognosis== | == Natural History, Complications and Prognosis== | ||
*The majority of patients with nasopharyngeal angiofibroma are symptomatic at diagnosis. | *The majority of patients with nasopharyngeal angiofibroma are symptomatic at diagnosis. | ||
*Early clinical features include epistaxis, [[facial pain]], and [[headache]]. | *Early clinical features include [[epistaxis]], [[facial pain]], and [[headache]]. | ||
*If left untreated, the majority of patients with nasopharyngeal angiofibroma may progress to develop malignant transformation. | *If left untreated, the majority of patients with nasopharyngeal angiofibroma may progress to develop malignant transformation. | ||
*Common complications of nasopharyngeal angiofibroma include transient blindness, optic nerve damage, and low-grade consumption coagulopathy. | *Common complications of nasopharyngeal angiofibroma include transient blindness, optic nerve damage, and low-grade consumption coagulopathy. | ||
| Line 89: | Line 87: | ||
== Diagnosis == | == Diagnosis == | ||
===Diagnostic Criteria=== | ===Diagnostic Criteria=== | ||
*The diagnosis of nasopharyngeal angiofibroma is made when | *The diagnosis of nasopharyngeal angiofibroma is made when the following diagnostic criteria are met: | ||
:*Clinical criteria | :*Clinical criteria | ||
::*Young patient | ::*Young patient | ||
| Line 95: | Line 93: | ||
:*Positive physical exam | :*Positive physical exam | ||
::*A smooth submucosal mass in the posterior nasal cavity | ::*A smooth submucosal mass in the posterior nasal cavity | ||
:*Positive imaging finding: | :*Positive imaging finding: visualization of a nasopharyngeal mass | ||
=== Symptoms === | === Symptoms === | ||
*Common symptoms of nasopharyngeal angiofibroma, may include: | *Common symptoms of nasopharyngeal angiofibroma, may include: | ||
:*Epistaxis or blood-tinged nasal discharge | :*[[Epistaxis]] or blood-tinged nasal discharge | ||
:*Unilateral nasal obstruction | :*Unilateral nasal obstruction | ||
:*[[Rhinorrhea]] | :*[[Rhinorrhea]] | ||
:*[[Hearing loss]] | :*[[Hearing loss]] | ||
:*[[Diplopia]] | :*[[Diplopia]] | ||
:* | :*[[Anosmia causes|Anosmia]] (rare) | ||
:*[[Eye pain]] | :*[[Eye pain]] | ||
=== Physical Examination === | === Physical Examination === | ||
*Patients with nasopharyngeal angiofibroma usually are well-appearing. | *Patients with nasopharyngeal angiofibroma usually are well-appearing. | ||
*Physical examination | *Physical examination may be remarkable for: | ||
:*A smooth submucosal mass in the posterior nasal cavity | :*A smooth [[submucosal]] mass in the posterior nasal cavity | ||
=== Laboratory Findings === | === Laboratory Findings === | ||
| Line 117: | Line 115: | ||
===Imaging Findings=== | ===Imaging Findings=== | ||
*Computed tomography is the imaging modality of choice for nasopharyngeal angiofibroma. | *Computed tomography is the imaging modality of choice for nasopharyngeal angiofibroma. | ||
*On conventional radiography, findings of nasopharyngeal angiofibroma | *On conventional radiography, findings of nasopharyngeal angiofibroma include: | ||
:* | :*Visualization of a nasopharyngeal mass | ||
:*Opacification of the sphenoid sinus | :*Opacification of the [[sphenoid sinus]] | ||
:*Anterior bowing of the posterior wall of the maxillary antrum | :*Anterior bowing of the posterior wall of the maxillary antrum | ||
:*''Holman-miller sign'': the anterior bowing of the posterior wall of the maxillary antrum which is seen on lateral skull film or cross-sectional imaging | :*''Holman-miller sign'': the anterior bowing of the posterior wall of the maxillary antrum which is seen on lateral skull film or cross-sectional imaging | ||
:*Widening of the pterygomaxillary fissure and pterygopalatine fossa | :*Widening of the pterygomaxillary fissure and pterygopalatine fossa | ||
:*Erosion of the medial pterygoid plate | :*Erosion of the medial pterygoid plate | ||
*On CT, findings of nasopharyngeal angiofibroma | *On CT, findings of nasopharyngeal angiofibroma include: | ||
:*Bony changes | :*Bony changes | ||
:*Non-encapsulated soft tissue mass | :*Non-encapsulated soft tissue mass | ||
:* | :*Anterior bowing the posterior wall of the maxillary antrum | ||
*On MRI, findings of nasopharyngeal angiofibroma | *On MRI, findings of nasopharyngeal angiofibroma include: | ||
:*T1: intermediate signal | :*T1: intermediate signal | ||
:*T2: heterogeneous signal | :*T2: heterogeneous signal - flow voids appear dark | ||
:*T1 C+ (Gd): shows prominent enhancement | :*T1 C+ (Gd): shows prominent enhancement | ||
*The images below demonstrate findings of nasopharyngeal angiofibroma. | *The images below demonstrate findings of nasopharyngeal angiofibroma. | ||
| Line 149: | Line 147: | ||
:*[[Hormonal therapy]] | :*[[Hormonal therapy]] | ||
:*[[Radiotherapy]] | :*[[Radiotherapy]] | ||
*Hormonal therapy for nasopharyngeal angiofibroma | *Hormonal therapy for nasopharyngeal angiofibroma includes:<ref name="pmid22164185">{{cite journal |vauthors=Nicolai P, Schreiber A, Bolzoni Villaret A |title=Juvenile angiofibroma: evolution of management |journal=Int J Pediatr |volume=2012 |issue= |pages=412545 |year=2012 |pmid=22164185 |pmc=3228400 |doi=10.1155/2012/412545 |url=}}</ref> | ||
:*[[Flutamide]] | :*[[Flutamide]] | ||
*Medical treatment is usually given before surgery to reduce the blood loss | *Medical treatment is usually given before surgery to reduce the blood loss | ||
| Line 159: | Line 157: | ||
*Preoperative embolization is highly suggested for nasopharyngeal angiofibroma. | *Preoperative embolization is highly suggested for nasopharyngeal angiofibroma. | ||
*Surgical approach for nasopharyngeal angiofibroma will depend on the stage.<ref name="pmid22164185">{{cite journal |vauthors=Nicolai P, Schreiber A, Bolzoni Villaret A |title=Juvenile angiofibroma: evolution of management |journal=Int J Pediatr |volume=2012 |issue= |pages=412545 |year=2012 |pmid=22164185 |pmc=3228400 |doi=10.1155/2012/412545 |url=}}</ref> | *Surgical approach for nasopharyngeal angiofibroma will depend on the stage.<ref name="pmid22164185">{{cite journal |vauthors=Nicolai P, Schreiber A, Bolzoni Villaret A |title=Juvenile angiofibroma: evolution of management |journal=Int J Pediatr |volume=2012 |issue= |pages=412545 |year=2012 |pmid=22164185 |pmc=3228400 |doi=10.1155/2012/412545 |url=}}</ref> | ||
:*The treatment of choice | :*The treatment of choice for early stage for nasopharyngeal angiofibroma is intranasal endoscopic surgery. Lateral rhinotomy is the preferred surgical approach. | ||
:*The treatment of choice | :*The treatment of choice for late stage for nasopharyngeal angiofibroma include the infratemporal fossa approach, and the mid-facial degloving approach. | ||
=== Prevention === | === Prevention === | ||
Revision as of 16:04, 26 April 2016
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Maria Fernanda Villarreal, M.D. [2]
Synonyms and keywords: Juvenile nasopharyngeal angiofibroma; angiofibroma of the nasopharynx; JNA
Overview
Nasopharyngeal angiofibroma (also called juvenile nasopharyngeal angiofibroma) is a locally aggressive, benign vascular neoplasm that grows in the pterygopalatine fossa. The most common symptoms of nasopharyngeal angiofibroma include one-sided nasal obstruction and recurrent bleeding. Nasopharyngeal angiofibroma may be classified according to Radkowski Classification System (severity) into 3 categories: I, II, and III. The majority of nasopharyngeal angiofibromas are irrigated by the external carotid artery. Genetic alterations associated with the development of nasopharyngeal angiofibroma include: overexpression of PDGF-B, bFGF, VEGF. Nasopharyngeal angiofibroma accounts for 0.05% of all head and neck tumors. Nasopharyngeal angiofibromas are more commonly observed among children and adolescents. Males are more commonly affected with nasopharyngeal angiofibroma than females. Common risk factors in the development of nasopharyngeal angiofibroma, include: presence of tumor in the pterygoid fossa and young age. Physical examination may be remarkable for smooth submucosal mass in the posterior nasal cavity. Computed tomography is the imaging modality of choice. On conventional radiography, findings of nasopharyngeal angiofibroma include: visualization of a nasopharyngeal mass, opacification of the sphenoid sinus, and anterior bowing of the posterior wall of the maxillary antrum. Surgery is the mainstay of therapy for nasopharyngeal angiofibroma. Surgical approach for nasopharyngeal angiofibroma will usually depend on the stage. The treatment of choice for early stage for nasopharyngeal angiofibroma is intranasal endoscopic surgery ( e.g. lateral rhinotomy). The treatment of choice for late stage nasopharyngeal angiofibroma include the infratemporal fossa approach, and the mid-facial degloving approach. Common complications of nasopharyngeal angiofibroma include transient blindness, optic nerve damage, and low-grade consumption coagulopathy.
Historical Perspective
- Nasopharyngeal angiofibroma was first described by Hippocrates, a Greek physician, in the 5th century BC.
Classification
- Nasopharyngeal angiofibroma may be classified according to Radkowski Classification System into 3 categories:[1]
- Stage I
- Ia: limited to nasal cavity/nasopharynx
- Ib: extension into one or more paranasal sinuses
- Stage II
- IIa: minimal extension through sphenopalatine foramen into pterygomaxillary fossa
- IIb: fills pterygomaxillary fossa bowing the posterior wall of the maxillary antrum anteriorly or extending into the orbit via the inferior orbital fissure
- IIc: extends beyond pterygomaxillary fossa into infratemporal fossa
- Stage III
- Stage IIIA: intracranial extension
Pathophysiology
- The pathogenesis of nasopharyngeal angiofibroma is characterized by the following features:
- Vascular neoplasm
- Originates from the pterygopalatine fossa
- The majority are associated with the external carotid artery
- Genetic alterations associated with the development of nasopharyngeal angiofibroma include:[2]
- Overexpression PDGF-B
- Overexpression bFGF
- Overexpression bFGF
- Deletion of chromosome 17
- Tumor suppressor gene p53
- Overexpression of Her-2/neu oncogene
- On gross pathology, characteristic findings of nasopharyngeal angiofibroma include:
- Unencapsulated
- Polypoid fibrous mass
- Bleeding on manipulation
- On microscopic histopathological analysis, characteristic findings of nasopharyngeal angiofibroma include:
- Fibroblastic cells with plump (near cuboidal) nuclei
- Fibrous stroma
- Abundant capillaries
Causes
- There are no known causes of nasopharyngeal angiofibroma.
Differentiating Nasopharyngeal Angiofibroma from Other Diseases
- Nasopharyngeal angiofibroma must be differentiated from other diseases that cause epistaxis, unilateral nasal obstruction, and rhinorrhea, such as:
- Antro-choanal polyp
- Rhinosporidiosis
- Chordoma
- Nasopharanageal cyst
- Pyogenic granuloma
Epidemiology and Demographics
- Nasopharyngeal angiofibroma is a rare tumor.
- Nasopharyngeal angiofibroma accounts for 0.05% of all head and neck tumors.
- The prevalence of nasopharyngeal angiofibroma is approximately 0.4 per 100,000 individuals worldwide.[1]
Age
- Nasopharyngeal angiofibroma is more commonly observed among patients aged 7-19 years.[1]
Gender
- The male to female ratio for nasopharyngeal angiofibroma is approximately 4 to 1.[1]
Race
- There is no racial predilection for nasopharyngeal angiofibroma.
Risk Factors
- Common risk factors in the development of nasopharyngeal angiofibroma include:
- Presence of tumor in the pterygoid fossa
- Young age
- Feeders from the internal carotid artery
- Residual tumor
Natural History, Complications and Prognosis
- The majority of patients with nasopharyngeal angiofibroma are symptomatic at diagnosis.
- Early clinical features include epistaxis, facial pain, and headache.
- If left untreated, the majority of patients with nasopharyngeal angiofibroma may progress to develop malignant transformation.
- Common complications of nasopharyngeal angiofibroma include transient blindness, optic nerve damage, and low-grade consumption coagulopathy.
- Prognosis is generally good, and the 5-year survival rate of patients with early stage nasopharyngeal angiofibroma is approximately 90%
- Survival rate of patients with late stage nasopharyngeal angiofibroma is approximately 50% to 75%.
Diagnosis
Diagnostic Criteria
- The diagnosis of nasopharyngeal angiofibroma is made when the following diagnostic criteria are met:
- Clinical criteria
- Young patient
- Epistaxis
- Positive physical exam
- A smooth submucosal mass in the posterior nasal cavity
- Positive imaging finding: visualization of a nasopharyngeal mass
Symptoms
- Common symptoms of nasopharyngeal angiofibroma, may include:
- Epistaxis or blood-tinged nasal discharge
- Unilateral nasal obstruction
- Rhinorrhea
- Hearing loss
- Diplopia
- Anosmia (rare)
- Eye pain
Physical Examination
- Patients with nasopharyngeal angiofibroma usually are well-appearing.
- Physical examination may be remarkable for:
- A smooth submucosal mass in the posterior nasal cavity
Laboratory Findings
- There are no specific laboratory findings associated with the diagnosis of nasopharyngeal angiofibroma.
Imaging Findings
- Computed tomography is the imaging modality of choice for nasopharyngeal angiofibroma.
- On conventional radiography, findings of nasopharyngeal angiofibroma include:
- Visualization of a nasopharyngeal mass
- Opacification of the sphenoid sinus
- Anterior bowing of the posterior wall of the maxillary antrum
- Holman-miller sign: the anterior bowing of the posterior wall of the maxillary antrum which is seen on lateral skull film or cross-sectional imaging
- Widening of the pterygomaxillary fissure and pterygopalatine fossa
- Erosion of the medial pterygoid plate
- On CT, findings of nasopharyngeal angiofibroma include:
- Bony changes
- Non-encapsulated soft tissue mass
- Anterior bowing the posterior wall of the maxillary antrum
- On MRI, findings of nasopharyngeal angiofibroma include:
- T1: intermediate signal
- T2: heterogeneous signal - flow voids appear dark
- T1 C+ (Gd): shows prominent enhancement
- The images below demonstrate findings of nasopharyngeal angiofibroma.
-
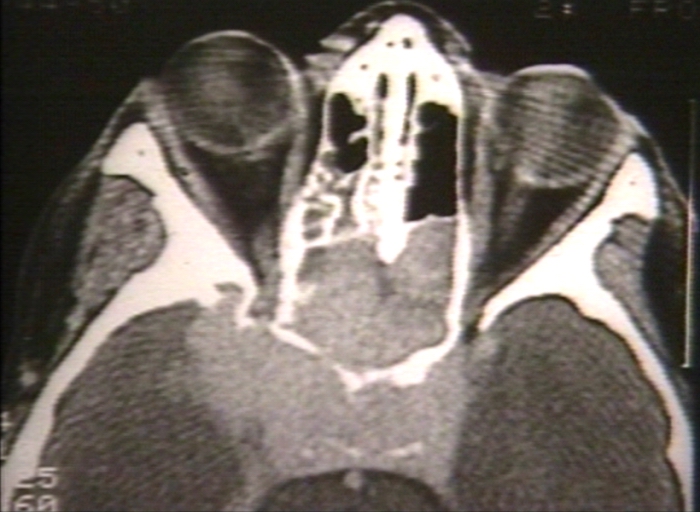
Nasopharyngeal angiofibroma. Skull base invasionImage courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology
-
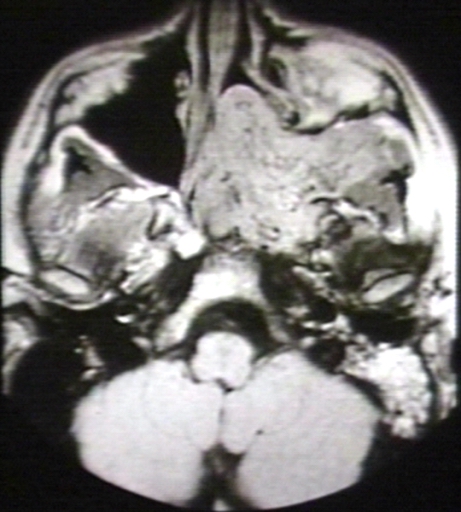
MRI (T1): Nasopharyngeal angiofibroma 1/3 Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology
-
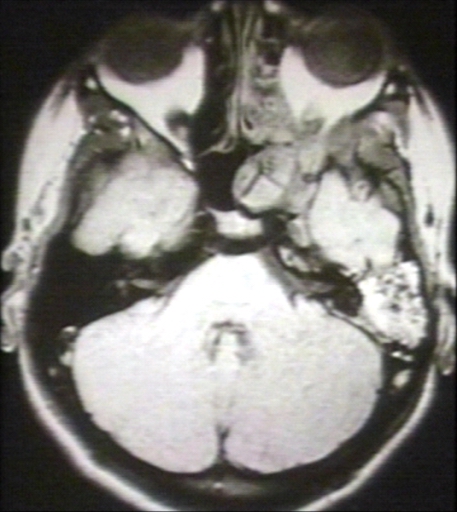
MRI (T1): Nasopharyngeal angiofibroma Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology
-
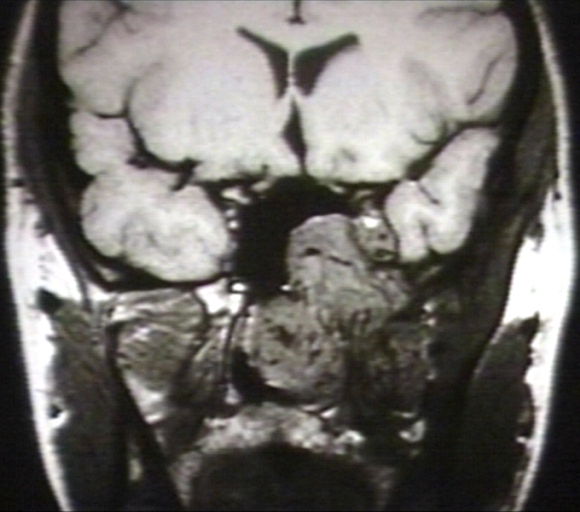
MRI (T1): Nasopharyngeal angiofibroma 3/3 Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology
-
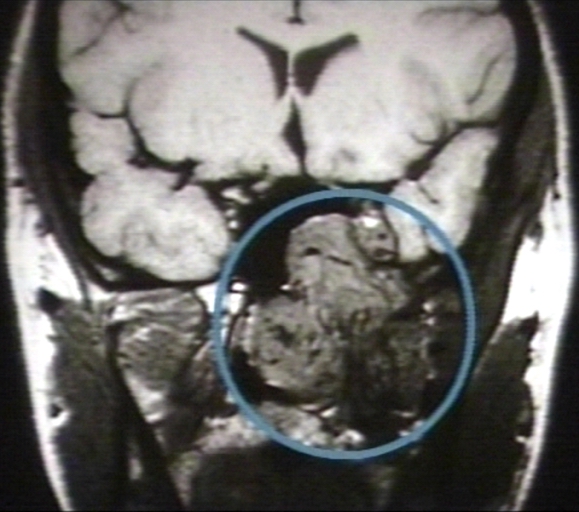
MRI (T1): Nasopharyngeal angiofibroma 3/3 (circled)Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology





Other Diagnostic Studies
- Nasopharyngeal angiofibroma may also be diagnosed using nasal endoscopy.
Treatment
Medical Therapy
- Medical therapy for nasopharyngeal angiofibroma is divided into 2 categories:[3]
- Hormonal therapy for nasopharyngeal angiofibroma includes:[3]
- Medical treatment is usually given before surgery to reduce the blood loss
- Radiotherapy for nasopharyngeal angiofibroma, include:
- Stereotactic radiotherapy
Surgery
- Surgery is the mainstay of therapy for nasopharyngeal angiofibroma.[3]
- Preoperative embolization is highly suggested for nasopharyngeal angiofibroma.
- Surgical approach for nasopharyngeal angiofibroma will depend on the stage.[3]
- The treatment of choice for early stage for nasopharyngeal angiofibroma is intranasal endoscopic surgery. Lateral rhinotomy is the preferred surgical approach.
- The treatment of choice for late stage for nasopharyngeal angiofibroma include the infratemporal fossa approach, and the mid-facial degloving approach.
Prevention
- There are no primary preventive measures available for nasopharyngeal angiofibroma.
- Once diagnosed and successfully treated, patients with nasopharyngeal angiofibroma are followed-up after surgery, and every 6 or 12 months, depending on the clinical progression.
References
- ↑ 1.0 1.1 1.2 1.3 Paris J, Guelfucci B, Moulin G, Zanaret M, Triglia JM (2001). "Diagnosis and treatment of juvenile nasopharyngeal angiofibroma". Eur Arch Otorhinolaryngol. 258 (3): 120–4. PMID 11374252.
- ↑ Coutinho-Camillo CM, Brentani MM, Nagai MA (2008). "Genetic alterations in juvenile nasopharyngeal angiofibromas". Head Neck. 30 (3): 390–400. doi:10.1002/hed.20775. PMID 18228521.
- ↑ 3.0 3.1 3.2 3.3 Nicolai P, Schreiber A, Bolzoni Villaret A (2012). "Juvenile angiofibroma: evolution of management". Int J Pediatr. 2012: 412545. doi:10.1155/2012/412545. PMC 3228400. PMID 22164185.