Mitral regurgitation
For patient information click here
Template:DiseaseDisorder infobox
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]
Please Take Over This Page and Apply to be Editor-In-Chief for this topic: There can be one or more than one Editor-In-Chief. You may also apply to be an Associate Editor-In-Chief of one of the subtopics below. Please mail us [3] to indicate your interest in serving either as an Editor-In-Chief of the entire topic or as an Associate Editor-In-Chief for a subtopic. Please be sure to attach your CV and or biographical sketch.
Mitral regurgitation (MR), a valvular heart disease also known as mitral insufficiency, is the abnormal leaking of blood through the mitral valve, from the left ventricle into the left atrium of the heart.
Etiology
The mitral valve is composed of the valve leaflets, the mitral valve annulus (which forms a ring around the valve leaflets), the papillary muscles (which tether the valve leaflets to the left ventricle, preventing them from prolapsing into the left atrium), and the chordae tendineae (which connect the valve leaflets to the papillary muscles). A dysfunction of any of these portions of the mitral valve apparatus can cause mitral regurgitation.
Primary mitral regurgitation is due to any disease process that affects the mitral valve apparatus itself. The causes of primary mitral regurgitation include:
- Myxomatous degeneration of the mitral valve
- Ischemic heart disease / Coronary artery disease
- Infective endocarditis
- Collagen vascular diseases (ie: SLE, Marfan's syndrome)
- Rheumatic heart disease
- Trauma
- Balloon valvulotomy of the mitral valve
- Certain forms of medication (e.g. fenfluramine)
The most common cause of primary mitral regurgitation in the United States (causing about 50% of primary mitral regurgitation) is myxomatous degeneration of the valve. Myxomatous degeneration of the mitral valve is more common in males, and is more common in advancing age. It is due to a genetic abnormality that results in a defect in the collagen that makes up the mitral valve. This causes a stretching out of the leaflets of the valve and the chordae tendineae. The elongation of the valve leaflets and the chordae tendineae prevent the valve leaflets from fully coapting when the valve is closed, causing the valve leaflets to prolapse into the left atrium, thereby causing mitral regurgitation.
Ischemic heart disease causes mitral regurgitation by the combination of ischemic dysfunction of the papillary muscles, and the dilatation of the left ventricle that is present in ischemic heart disease, with the subsequent displacement of the papillary muscles and the dilatation of the mitral valve annulus.
Secondary mitral regurgitation is due to the dilatation of the left ventricle, causing stretching of the mitral valve annulus and displacement of the papillary muscles. This dilatation of the left ventricle can be due to any cause of dilated cardiomyopathy, including aortic insufficiency, nonischemic dilated cardiomyopathy and Noncompaction Cardiomyopathy.
Mechanisms of Mitral Regurgitation
- Anterior Leaflet Prolapse
- Posterior Leaflet Prolapse
- Bileaflet Prolapse
- Restricted Leaflets
- Apical Tethering
- Papillary muscle rupture
- Ischemic Papillary Rupture
- Leaflet Perforation
Full Differential Diagnosis of Causes of Mitral Regurgitaion
- Coronary Heart Disease
- Congenital mitral regurgitation
- Ehlers-Danlos Syndrome
- Heart Failure
- Hypertrophic obstructive cardiomyopathy
- Infective endocarditis
- Left ventricular dilation
- Marfan Syndrome
- Mitral annular calcification
- Mitral valve prolapse
- Myocardial Infarction
- Myxomatous degeneration
- Osteogenesis imperfecta
- Prosthetic valve dysfunction
- Rheumatic Heart Disease
- Systemic Lupus Erythematosus
- Trauma
Pathophysiology
The pathophysiology of mitral regurgitation can be divided into three phases of the disease process: the acute phase, the chronic compensated phase, and the chronic decompensated phase.

During systole, contraction of the left ventricle causes abnormal backflow (arrow) into the left atrium.
1 Mitral valve
2 Left Ventricle
3 Left Atrium
4 Aorta
Acute phase
Acute mitral regurgitation (as may occur due to the sudden rupture of a chordae tendineae or papillary muscle) causes a sudden volume overload of both the left atrium and the left ventricle.
The left ventricle develops volume overload because with every contraction it now has to pump out not only the volume of blood that goes into the aorta (the forward cardiac output or forward stroke volume), but also the blood that regurgitates into the left atrium (the regurgitant volume).
The combination of the forward stroke volume and the regurgitant volume is known as the total stroke volume of the left ventricle.
In the acute setting, the stroke volume of the left ventricle is increased (increased ejection fraction), but the forward cardiac output is decreased. The mechanism by which the total stroke volume is increased is known as the Frank-Starling mechanism.
The regurgitant volume causes a volume overload and a pressure overload of the left atrium. The increased pressures in the left atrium inhibit drainage of blood from the lungs via the pulmonary veins. This causes pulmonary congestion.
Chronic compensated phase
If the mitral regurgitation develops slowly over months to years or if the acute phase can be managed with medical therapy, the individual will enter the chronic compensated phase of the disease. In this phase, the left ventricle develops eccentric hypertrophy in order to better manage the larger than normal stroke volume.
The eccentric hypertrophy and the increased diastolic volume combine to increase the stroke volume (to levels well above normal) so that the forward stroke volume (forward cardiac output) approaches the normal levels.
In the left atrium, the volume overload causes enlargement of the chamber of the left atrium, allowing the filling pressure in the left atrium to decrease. This improves the drainage from the pulmonary veins, and signs and symptoms of pulmonary congestion will decrease.
These changes in the left ventricle and left atrium improve the low forward cardiac output state and the pulmonary congestion that occur in the acute phase of the disease. Individuals in the chronic compensated phase may be asymptomatic and have normal exercise tolerances.
Chronic decompensated phase
An individual may be in the compensated phase of mitral regurgitation for years, but will eventually develop left ventricular dysfunction, the hallmark for the chronic decompensated phase of mitral regurgitation. It is currently unclear what causes an individual to enter the decompensated phase of this disease. However, the decompensated phase is characterized by calcium overload within the cardiac myocytes.
In this phase, the ventricular myocardium is no longer able to contract adequately to compensate for the volume overload of mitral regurgitation, and the stroke volume of the left ventricle will decrease. The decreased stroke volume causes a decreased forward cardiac output and an increase in the end-systolic volume. The increased end-systolic volume translates to increased filling pressures of the ventricular and increased pulmonary venous congestion. The individual may again have symptoms of congestive heart failure.
The left ventricle begins to dilate during this phase. This causes a dilatation of the mitral valve annulus, which may worsen the degree of mitral regurgitation. The dilated left ventricle causes an increase in the wall stress of the cardiac chamber as well.
While the ejection fraction is less in the chronic decompensated phase than in the acute phase or the chronic compensated phase of mitral regurgitation, it may still be in the normal range (i.e: > 50 percent), and may not decrease until late in the disease course. A decreased ejection fraction in an individual with mitral regurgitation and no other cardiac abnormality should alert the physician that the disease may be in its decompensated phase.
| Acute mitral regurgitation | Chronic mitral regurgitation | |
|---|---|---|
| Electrocardiogram | Normal | P mitrale, atrial fibrillation, left ventricular hypertrophy |
| Heart size | Normal | Cardiomegaly, left atrial enlargement |
| Systolic murmur | Heard at the base, radiates to the neck, spine, or top of head | Heard at the apex, radiates to the axilla |
| Apical thrill | May be absent | Present |
| Jugular venous distension | Present | Absent |
Symptoms
The symptoms associated with mitral regurgitation are dependent on which phase of the disease process the individual is in. Individuals with acute mitral regurgitation will have the signs and symptoms of decompensated congestive heart failure (ie: shortness of breath, pulmonary edema, orthopnea, paroxysmal nocturnal dyspnea), as well as symptoms suggestive of a low cardiac output state (ie: decreased exercise tolerance). Cardiovascular collapse with shock (cardiogenic shock) may be seen in individuals with acute mitral regurgitation due to papillary muscle rupture or rupture of a chordae tendineae.
Individuals with chronic compensated mitral regurgitation may be asymptomatic, with a normal exercise tolerance and no evidence of heart failure. These individuals may be sensitive to small shifts in their intravascular volume status, and are prone to develop volume overload (congestive heart failure).
Diagnostic studies
There are many diagnostic tests that have abnormal results in the presence of mitral regurgitation.
These tests suggest the diagnosis of mitral regurgitation and may indicate to the physician that further testing is warranted. For instance, the electrocardiogram (ECG) in long standing mitral regurgitation may show evidence of left atrial enlargement and left ventricular hypertrophy.
Atrial fibrillation may also be noted on the ECG in individuals with chronic mitral regurgitation.
The ECG may not show any of these finding in the setting of acute mitral regurgitation.
The quantification of mitral regurgitation usually employs imaging studies such as echocardiography or magnetic resonance angiography of the heart.
Chest x-ray

The chest x-ray in individuals with chronic mitral regurgitation is characterized by enlargement of the left atrium and the left ventricle. The pulmonary vascular markings are typically normal, since pulmonary venous pressures are usually not significantly elevated.
Calcification of the mitral annulus is not infrequent, seen in up to 35% of elderly patients on echocardiography which is more sensitive than CXR. It typically begins around the margins of the posterior leaflet forming a “C” (as in this case) - eventually with anterior leaflet involvement the “C” closes forming an “O”.
Although it is associated with mitral regurgitation this is of usually trivial amounts. As opposed to aortic valve calcification, calcification of the mitral annulus is not significantly associated with stenosis of the valve and contrary to previous thought, nor is it associated with strokes - when other factors are controlled for.
The calcification however can impede AV nodal conduction and therefore lead to varying degrees of heart block.
Pathologically it is important to distinguish annular calcification, which is not on the leaflet, and is covered with intact endothelium, from leaflet calcification in stenotic valves secondary to rheumatic fever.
Echocardiography

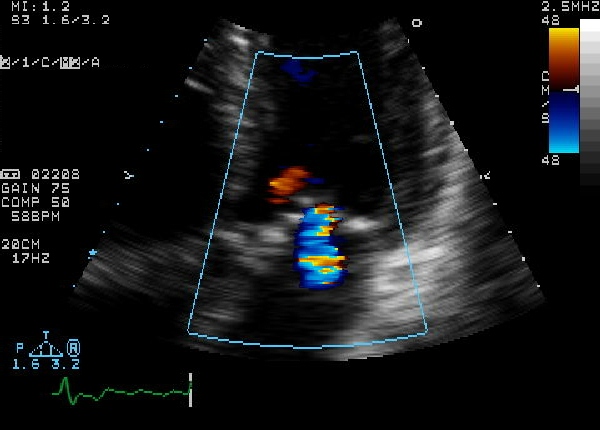
The echocardiogram is commonly used to confirm the diagnosis of mitral regurgitation. Color doppler flow on the transthoracic echocardiogram (TTE) will reveal a jet of blood flowing from the left ventricle into the left atrium during ventricular systole.
Because of the inability in getting accurate images of the left atrium and the pulmonary veins on the transthoracic echocardiogram, a transesophageal echocardiogram may be necessary to determine the severity of the mitral regurgitation in some cases.
Factors that suggest severe mitral regurgitation on echocardiography include systolic reversal of flow in the pulmonary veins and filling of the entire left atrial cavity by the regurgitant jet of MR.
 |
Aetiology and morphological features in 2-D Echocardiography
Rheumatic Mitral regurgitation
In rheumatic mitral regurgitation, there is some degree of commissural fusion and thickening of the tips visible in 2 dimensional echocardiography. The movement of the valve leaflets is restricted.
Myxomatous mitral valve
The leaflets and chordae are thick and reduntant. Reduced tensile strength leads to progressive elongation or rupture of chordae. Ruptured chordae appear as flail segments. To diagnose mitral valve prolapse, the following criteria should be fulfilled during echocardiography - Movement of any part of either leaflet more than 2mm behind the annular plane in parasternal long axis view and movement of point of co-aptation behind the annular plane in apical 4 chamber view.
Annular calcification
Mitral annulus is usually smaller in systole. The increased rigidity due to annular calcification impairs contraction. In 2D- echocardiography, there is increased echogenicity on the LV side immediately adjacent to the attachment of the posterior mitral valve leaflet. Region of anterior mitral leaflet is only rarely involved. This is common in elderly subjects and younger ones with chronic renal failure and hypertension.
Ischaemic mitral regurgitation
Mitral regurgitation can occur in ischaemia as a result of regional LV dysfunction with abnormal contraction of papillary muscle or underlying ventricular wall. Myocardial infarction can result in MR at rest while in ischaemia it is intermeitting. This characterised by restricted valve leaflet motion and tenting of mitral valve in systole.
Papillary muscle rupture
This is usually a complication of myocardial infarction. If entire papillary muscle is disconnected from the left ventricle severe MR results and few survive. Partial rupture is more common.
Functional mitral regurgitation
Functional MR results due to LV dilatation and systolic dysfunction in those with a structurally normal mitral valve apparatus.
Assessment of severity
Colour flow mapping
- Size of flow recruitment is noted
- Jet base width at the valve level
- Intra atrial jet area if it is a central jet
- Jet direction is usually away from a prolapsing leaflet and behind a restricted leaflet
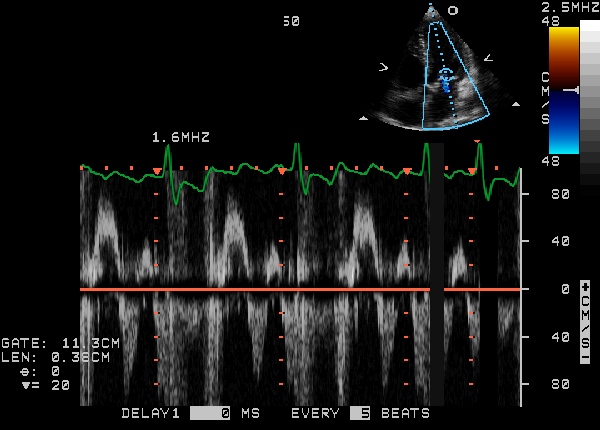
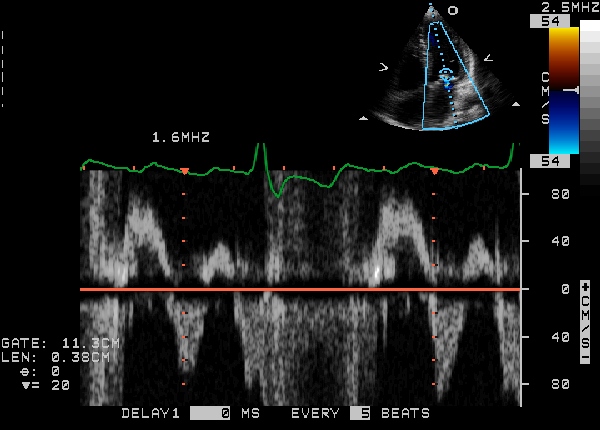
Continuous wave doppler
- Shape and density of signal - In severe Mitral regurgitation, the flow is dense and triangular
- If as dense as forward flow, it is severe.
Pulse wave doppler(PW)
- PW in apical-4-chamber view
- E wave more than 1.2m/s indicates severe MR
- Even minor mitral stenosis or hyperdynamic circulation can increase E wave
- If A-wave dominant, severe MR is virtually ruled out.
vena contracta
- vena contracta is the narrowest region of regurgitant jet (usually just below the valve in LA)
- >0.7 cm - severe MR
Pulmonary Venous Flow
- usually forward throughout cycle
- systolic dominant
- as MR worsens, there is a blunting of systolic flow
- If severe MR - systolic flow reversal.
Regurgitant volume
- Mitral regurgitant volume = Mitral inflow volume - LV outflow volume
- Mitral inflow volume = Vti * Cross sectional area of mitral valve
- LV outflow volume = Vti * Cross sectional area at LV outflow
- Regurtitant volume - <20% - mild , >50% severe
PISA (Proximal isovelocity surface area)
The radius of Proximal isovelocity surface area or flow convergence zone which is a 3-dimensional surface area proximal to a narrowed orifice at which all the blood velocities are equal, can be used to calculate the severity of mitral regurgitation. The principle is that if the mitral regurgitation is mild, only the blood nearer to the valve orifice accelerates towards the atrium while in severe regurgitation, blood farther away from the valve moves back.
PISA radius
A simple method to determine severity of mitral regurgitation is to measure the PISA radius. Regurgitation is mild if radius is <0.4 cm and severe if >1 cm.
Regurgitant flow (instantaneous)
The instantaneous regurgitant flow can be calculated from the PISA radius and can be used to assess the severity of mitral regurgitation.
Regurgitant flow = 2π * r2 * Valiasing
Effective regurgitant orifice area (EROA)
Effective regurgitant orifice area can be calculated using the instantaneous regurgitant flow. The formula can be derived from the following:
Valiasing * 2πr2 = Vmax * EROA
hence:
- EROA = PISA (2πr2) * Valiasing / Vmax
Mild = 0-20 cm2, moderate = 20 - 40 cm2, severe = >40 cm2
Regurgitant volume can be calculated from this.
- Regurgitant volume = Effective regurgitant orifice area * Vtime integrale
Diastolic Mitral Regurgitation Secondary to Severe Aortic Stenosis
Diastolic mitral regurgitation due to severe aortic stenosis

Diastolic mitral regurgitation due to severe aortic stenosis

Diastolic mitral regurgitation due to severe aortic stenosis

- <googlevideo>424719160215823743&hl=en</googlevideo>
- <googlevideo>-1316686479831791521&hl=en</googlevideo>
Quantification of mitral regurgitation
| Degree of mitral regurgitation | Regurgitant fraction | Regurgitant Orifice area |
|---|---|---|
| Mild mitral regurgitation | < 20 percent | |
| Moderate mitral regurgitation | 20 - 40 percent | |
| Moderate to severe mitral regurgitation | 40 - 60 percent | |
| Severe mitral regurgitation | > 60 percent | > 0.3 cm2 |
The degree of severity of mitral regurgitation can be quantified by the percentage of the left ventricular stroke volume that regurgitates into the left atrium (the regurgitant fraction).
Methods that have been used to assess the regurgitant fraction in mitral regurgitation include echocardiography, cardiac catheterization, fast CT scan, and cardiac MRI.
The echocardiographic technique to measure the regurgitant fraction is to determine the forward flow through the mitral valve (from the left atrium to the left ventricle) during ventricular diastole, and comparing it with the flow out of the left ventricle through the aortic valve in ventricular systole.
This method assumes that the aortic valve does not suffer from aortic insufficiency. The regurgitant fraction would be described as:
Another way to quantify the degree of mitral regurgitation is to determine the area of the regurgitant flow at the level of the valve. This is known as the regurgitant orifice area, and correlates with the size of the defect in the mitral valve.
One particular echocardiographic technique used to measure the orifice area is measurement of the proximal isovelocity surface area (PISA). The flaw of using PISA to determine the mitral valve regurgitant orifice area is that it measures the flow at one moment in time in the cardiac cycle, which may not reflect the average performance of the regurgitant jet.
Severity (Summary)
| Severity | mild | severe |
|---|---|---|
| Jet area | <4 cm2 | >8 cm2 |
| Jet width | thin | >0.6 |
| vena contracta | <0.3 | >0.7 |
| PISA radius | <0.4 | >1 |
| Pulmonary venous flow | systolic dominant | systolic flow reversal |
| Mitral inflow | can be A wave dominant | E wave dominant >1.2m/s |
| Continuous wave doppler | soft and parabolic | dense and triangular |
| LV and LA | normal size | enlarged (in chronic MR) |
| duration | can be short | holosystolic |
| Regurgitant volume | <30 ml | >60 ml |
| EROA | 0-20 cm2 | >40 cm2 |
Treatment
The treatment of mitral regurgitation depends on the acuteness of the disease and whether there are associated signs of hemodynamic compromise.
In acute mitral regurgitation secondary to a mechanical defect in the heart (ie: rupture of a papillary muscle or chrordae tendineae), the treatment of choice is urgent mitral valve replacement. If the patient is hypotensive prior to the surgical procedure, an intra-aortic balloon pump may be placed in order to improve perfusion of the organs and to decrease the degree of mitral regurgitation.
If the individual with acute mitral regurgitation is normotensive, vasodilators may be of use to decrease the afterload seen by the left ventricle and thereby decrease the regurgitant fraction. The vasodilator most commonly used is nitroprusside.
Individuals with chronic mitral regurgitation can be treated with vasodilators as well. In the chronic state, the most commonly used agents are ACE inhibitors and hydralazine. Studies have shown that the use of ACE inhibitors and hydralazine can delay surgical treatment of mitral regurgitation1,2. The current guidelines for treatment of mitral regurgitation limit the use of vasodilators to individuals with hypertension, however.
There are two surgical options for the treatment of mitral regurgitation: mitral valve replacement and mitral valve repair.
Indication for surgery
Indications for surgery for chronic mitral regurgitation include signs of left ventricular dysfunction.
These include an ejection fraction of less than 60 percent and a left ventricular end systolic dimension (LVESD) of greater than 45 mm.
| Symptoms | LV EF | LVESD |
|---|---|---|
| NYHA II - IV | > 60 percent | < 45 mm |
| Asymptomatic or symptomatic | 50 - 60 percent | ≥ 45 mm |
| Asymptomatic or symptomatic | < 50 percent or ≥ 45 mm | |
| Pulmonary artery systolic pressure ≥ 50 mmHg | ||
Echocardiographic Findings
- Mitral Ring dehiscence post repair with severe mitral regurgitation
<googlevideo>7246533519972889950&hl=en</googlevideo>
- Severe Mitral Regurgitation From Ring dehiscence Pulmonary Vein Pulsed Wave Doppler

- Severe Mitral Regurgitation Pulmonary Vein Pulsed Wave Doppler

Left Ventriculographic Evaluation of Mitral Regurgitation
Both the RAO and LAO/Cranial projections can be used to identify significant mitral regurgitation. Grading the amount of regurgitation is based on the amount of opacification of the atrium compared to the ventricular opacification, atrial size and the number of cycles required for maximal opacification. Elevation of left atrial pressure in acute regurgitation and dilation of the left atrium from chronic regurgitation can both interfere with the use of this grading system.
1+ Brief and incomplete atrial opacification over several cycles. Clears rapidly. No atrial enlargement.
<googlevideo>8237703398893439012&hl=en</googlevideo> 1+ MR
<googlevideo>-8044287213933915863&hl=en</googlevideo> 1+ MR LAO with SAM
2+ Moderate opacification of the atria with each cycle. Never greater than LV opacification. No significant LA enlargement.
<googlevideo>-3259427927007644054&hl=en</googlevideo> 2+ MR
3+ Atrial opacification equal to ventricular opacification. Delayed clearing of atria over several cycles. Significant enlargement of the LA.
<googlevideo>-8295323872088090226&hl=en</googlevideo> 3-4+ MR
<googlevideo>2584010676245016071&hl=en</googlevideo> 3+ MR
4+ Atrial Opacification immediate and greater than that of the ventricle. Severe enlagement of the LA. Opacification of the pulmonary veins.
<googlevideo>-5531059825466069834&hl=en</googlevideo> 4+ Paravalvular MR
<googlevideo>7527640933077169571&hl=en</googlevideo> 4+ MR
Severe Mitral Regurgitation by Ventriculogram
<youtube v=PWsyET0ZBL8/>
References
1. Greenberg BH, Massie BM, Brundage BH, Botvinick EH, Parmley WW, Chatterjee K. Beneficial effects of hydralazine in severe mitral regurgitation. Circulation. 1978 Aug;58(2):273-9. (Medline abstract)
2. Hoit BD. Medical treatment of valvular heart disease. Curr Opin Cardiol. 1991 Apr;6(2):207-11. (Medline abstract)
3. Bono w et al. ACC/AHA Guidelines for the Management of Patients With Valvular Heart Disease. ACC/AHA Task Force Report. JACC Vol. 32, No. 5, November 1998:1486-1588 (Full article)
See also
- Mitral valve
- Left ventricle
- Left atrium
- Systole (medicine)
- Diastole
- Cardiac output
- Mitral valve prolapse
- Cardiomyopathy
External Links
- Echo in context: Video lessons and slides of mitral regurgitation
- Yale atlas of echocardiography: Mitral regurgitation
- Mitral Regurgitation information from Seattle Children's Hospital Heart Center
- Mitral Valve Repair at The Mount Sinai Hospital
- NEW Investigational Treatment in the EVEREST II Clinical Research Study - Percutaneous Mitral Repair
Acknowledgements
The content on this page was first contributed by: C. Michael Gibson, M.S., M.D.
Template:Link FA de:Mitralklappeninsuffizienz