Endocarditis pathophysiology
| https://https://www.youtube.com/watch?v=kW-85yk0ErQ%7C350}} |
|
Endocarditis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease |
|
Case Studies |
|
Endocarditis pathophysiology On the Web |
|
Risk calculators and risk factors for Endocarditis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1] Associate Editor(s)-in-Chief: Maliha Shakil, M.D. [2]
Overview
The pathogenesis of infective endocarditis includes valvular damage, altered and turbulent flow, bacteremia, and lack of blood supply to the valves.[1] Damaged endothelium becomes a site for attachment of infectious agents in infectious endocarditis. Nonbacterial thrombotic endocarditis is related to hypercoaguable states such as pregnancy or systemic bacterial infection.[2] The characteristic lesion of endocarditis is a vegetation. Vegetations are composed of fibrin, inflammatory cells, platelets, and microorganisms.[3]
Pathophysiology
Pathogenesis
Infective Endocarditis
The pathogenesis of infective endocarditis includes:[1][2]
| Pathogenic Factors | Mechanism |
|---|---|
|
|
|
|
|
|
Nonbacterial thrombotic endocarditis
- Nonbacterial thrombotic endocarditis (NBTE), also called marantic endocarditis is most commonly found on previously undamaged valves.
- The vegetations in NBTE are small, sterile, and tend to aggregate along the edges of the valve or the cusps.
- Unlike infective endocarditis, NBTE does not cause an inflammation response from the body.
- NBTE usually occurs due to hypercoaguable states such as systemic bacterial infection or pregnancy. NBTE may also occur in patients with cancer, particularly mucinous adenocarcinoma.
- Libman-Sacks endocarditis is another form of sterile endocarditis; this form occurs more often in patients with lupus erythematosus and is thought to be due to the deposition of immune complexes.
- Libman-Sacks endocarditis involves small vegetations, while infective endocarditis is composed of large vegetations. These immune complexes precipitate an inflammatory reaction, which helps to differentiate it from NBTE.
- Unlike NBTE, Libman-Sacks endocarditis does not seem to have a preferred location of deposition and may form on the undersurfaces of the valves or even on the endocardium.[2]
Gross and Microscopic Pathology
The characteristic lesion of endocarditis is a vegetation. Vegetations are composed of fibrin, inflammatory cells, platelets, and microorganisms.[3] Characteristic features of endocarditis on gross pathology and histopathological analysis include:[4]
| Endocarditis Subtype | Features on Gross Pathology | Features on Histopathological Microscopic Analysis |
| Infective Endocarditis |
|
|
| Nonbacterial Thrombotic Endocarditis |
|
|
Pathology
-
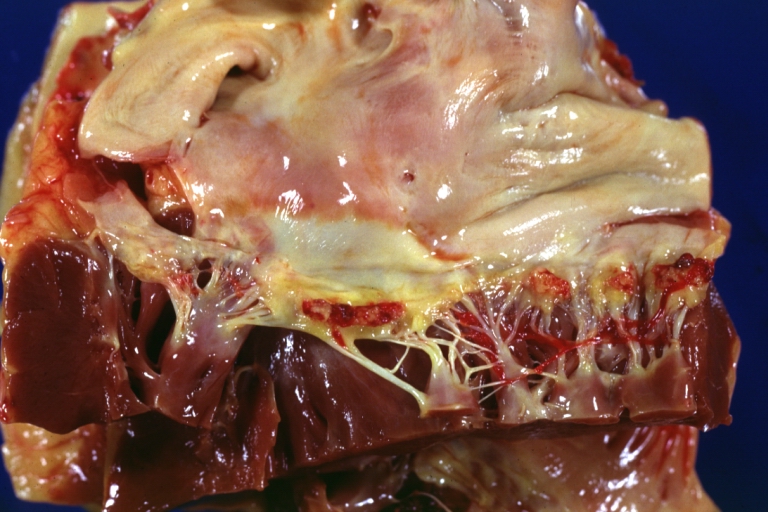
Heart; Breast intraductal papilloma metastasis. Thrombotic Nonbacterial Endocarditis (Infected): Gross mitral valve natural color vegetations well illustrated these were secondarily infected with staphylococcus case of 8 year survival breast intraductal papillary adenocarcinoma with extensive metastases. Aortic valve also involved.
-
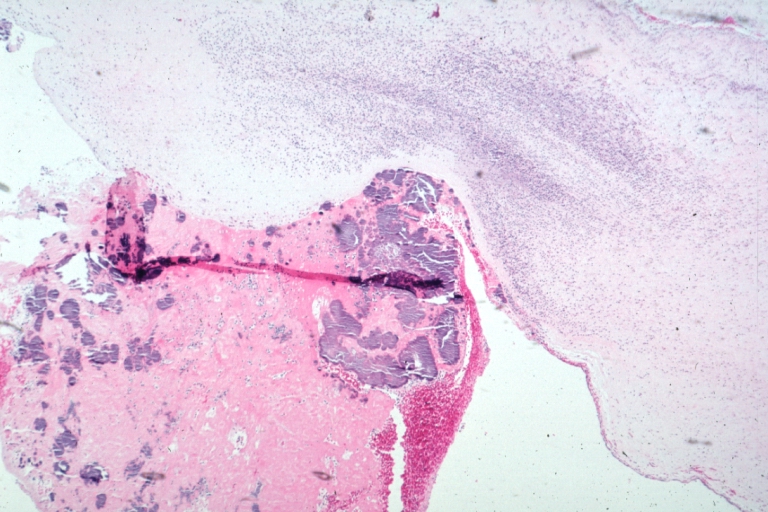
Nonbacterial Thrombotic Endocarditis Infected: Micro low mag H&E fibrin vegetation with masses of staphylococci and inflammatory cells in valve secondarily infected case 8 year survival breast papillary intraductal adenocarcinoma with extensive metastases gross is aortic valve lesions.


Videos
{{#ev:youtube|gk7cpP2ymOs}} {{#ev:youtube|BiNulEFh6rU}}
References
- ↑ 1.0 1.1 Infective endocarditis. Wikipedia (2015). https://en.wikipedia.org/wiki/Infective_endocarditis#Pathogenesis Accessed on September 21, 2015
- ↑ 2.0 2.1 2.2 Endocarditis. Wikipedia (2015). https://en.wikipedia.org/wiki/Endocarditis Accessed on September 21, 2015
- ↑ 3.0 3.1 Mylonakis E, Calderwood SB (2001). "Infective endocarditis in adults". N Engl J Med. 345 (18): 1318–30. doi:10.1056/NEJMra010082. PMID 11794152.
- ↑ Infective Endocarditis. Libre Pathology (2015). URL=http://librepathology.org/wiki/index.php/Infective_endocarditis Accessed on September 21, 2015