Multiple sclerosis history and symptoms: Difference between revisions
No edit summary |
No edit summary |
||
| Line 6: | Line 6: | ||
== History and Symptoms == | == History and Symptoms == | ||
The hallmark of MS disease is Variability in symptoms. | |||
First common symptoms of MS disease are optic neuritis, diplopia, sensory or motor loss, vertigo and balance problems. In young adult eye and sensory problems are prominent while in older patients we see motor problems more often.<ref name="pmid2917275">{{cite journal |vauthors=Weinshenker BG, Bass B, Rice GP, Noseworthy J, Carriere W, Baskerville J, Ebers GC |title=The natural history of multiple sclerosis: a geographically based study. I. Clinical course and disability |journal=Brain |volume=112 ( Pt 1) |issue= |pages=133–46 |date=February 1989 |pmid=2917275 |doi= |url=}}</ref> | First common symptoms of MS disease are optic neuritis, diplopia, sensory or motor loss, vertigo and balance problems. In young adult eye and sensory problems are prominent while in older patients we see motor problems more often.<ref name="pmid2917275">{{cite journal |vauthors=Weinshenker BG, Bass B, Rice GP, Noseworthy J, Carriere W, Baskerville J, Ebers GC |title=The natural history of multiple sclerosis: a geographically based study. I. Clinical course and disability |journal=Brain |volume=112 ( Pt 1) |issue= |pages=133–46 |date=February 1989 |pmid=2917275 |doi= |url=}}</ref> | ||
=== common symptoms === | |||
==== fatigue: ==== | |||
Fatigue is seen in almost 80% of MS patient. They commonly feel exhausted and out of energy. The etiology of this symptom is poorly understood. | |||
=== Eye Symptoms === | === Eye Symptoms === | ||
Revision as of 18:23, 28 February 2018
|
Multiple sclerosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Multiple sclerosis history and symptoms On the Web |
|
American Roentgen Ray Society Images of Multiple sclerosis history and symptoms |
|
Risk calculators and risk factors for Multiple sclerosis history and symptoms |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
History and Symptoms
The hallmark of MS disease is Variability in symptoms.
First common symptoms of MS disease are optic neuritis, diplopia, sensory or motor loss, vertigo and balance problems. In young adult eye and sensory problems are prominent while in older patients we see motor problems more often.[1]
common symptoms
fatigue:
Fatigue is seen in almost 80% of MS patient. They commonly feel exhausted and out of energy. The etiology of this symptom is poorly understood.
Eye Symptoms
Individuals experience rapid onset of pain in one eye, followed by blurry vision in part or all of the visual field of that eye. Inflammation of the optic nerve causes loss of vision usually due to the swelling and destruction of the myelin sheath covering the optic nerve. This condition is called optic neuritis.
The blurred vision usually resolves within ten weeks, but individuals are often left with less vivid color vision (especially red) in the affected eye.
Bladder
Bladder problems which can be seen in vast majority of MS patients include: incontinency, frequency, urine retention, hesitation and leaking. These symptoms have negative effect on patient life. [2][3][4]
Cognitive
Cognitive impairments are common. Neuropsychological studies suggest that 40 to 60 percent of patients have cognitive deficits;[5] with the lowest percentages usually from community-based studies and the highest ones from hospital-based.
Cognitive impairment, sometimes referred to as brain fog, is already present in the beginnings of the disease.[6] Even in probable MS (after the first attack but before a second confirmatory one) up to 50% of patients have mild impairment.[7]
Some of the most common declines are in recent memory, attention, processing speed, visual-spatial abilities and executive functions.[8] Other cognitive-related symptoms are emotional instability, and fatigue, including purely neurological fatigue. The cognitive impairments in MS are usually mild; and only in 5% of patients can we speak of dementia. Nevertheless they are related with unemployment and reduced social interactions.[9] They are also related with driving difficulties.[10]
Emotional
Emotional symptoms are also common and are thought to be both the normal response to having a debilitating disease and the result of damage to specific areas of the cental nervous system that generate and control emotions.
Clinical depression is the most common neuropsychiatric condition: lifetime depression prevalence rates of 40-50% and 12 month prevalence rates around 20% have been typically reported for samples of people with MS; these figures are considerably higher than those for the general population or for people with other chronic illnesses.[11][12]
Other feelings such as anger, anxiety, frustration, and hopelessness also appear frequently, and suicide is a very real threat since 15% of deaths in MS sufferers are due to this cause.[13]. Many brain-imaging studies have tried to relate depression to lesions in different brain regions with variable success. On balance the evidence seems to favour an association with neuropathology in the left anterior temporal/parietal regions.[14]
Fatigue
Fatigue is very common and disabling in MS. At the same time it has a close relationship with depressive symptomatology.[15] When depression is reduced fatigue also tends to improve, so patients should be evaluated for depression before other therapeutic approaches are used.[16]. In a similar way other factors like disturbed sleep, chronic pain, poor nutrition, or even some medications can contribute to fatigue; and therefore medical professionals are encouraged to identify and modify them.[17]
Mobility Restrictions
Restrictions in mobility (walking, transfers, bed mobility) are common in individuals suffering from multiple sclerosis. Within 10 years after the onset of MS one-third of patients reach a score of 6 on the Expanded Disability Status Scale (requiring the use of a unilateral walking aid),and by 30 years the proportion increases to 83%. Within 5 years the Expanded Disability Status Score is 6 in 50% of those with the progressive form of MS.[18]
In MS a wide range of impairments may exist which can act either alone or in combination to impact directly on a person's balance, function and mobility. Such impairments include fatigue, weakness, hypertonicity, low exercise tolerance, impaired balance, ataxia and tremor.[19]
Pain
Pain is a common symptom in MS; appearing in 55% of patients at some point of their disease process; specially as time passes.[20]. It is strong and debilitating and has a profound effect in the quality of life and mental health of the sufferer.[21] It usually appears after a lesion to the ascending or descending tracts that control the transmission of painful stimulus. such as the anterolateral system, but many other causes are also possible.[22] Most frequent pains reported are headaches (40%), dysesthetic limb pain (19%), back pain (17%), and painful spasms (11%).[23]
Acute pain is mainly due to optic neuritis.[24] Subacute pain is usually secondary to the disease and can be consequence of being too much time in the same position, urinary retention, infected skin ulcers and many others. Chronic pain is very common and the harder to treat being its most common cause dysesthesias.
Trigeminal Neuralgia
Trigeminal neuralgia or "tic douloureux", is a disorder of the trigeminal nerve that causes episodes of intense pain in the eyes, lips, nose, scalp, forehead, and jaw. It affects 1 to 2% of MS patients during their disease.[25][26] The episodes of pain occur paroxysmally, or suddenly; and the patients describe it as trigger area on the face, so sensitive that touching or even air currents can bring an episode of pain.
Dysesthesias
Dysesthesias are disagreeable sensations produced by ordinary stimuli. The abnormal sensations are often described as painful feelings such as burning, wetness, itching, electric shock or pins and needles; and are caused by lesions of the peripheral or central sensory pathways.
Sexual
Sexual dysfunction (SD) is one of many symptoms affecting persons with a diagnosis of multiple sclerosis (MS) and other neurological disease. SD in men encompasses both erectile and ejaculatory disorder. The prevalence of SD in men with MS ranges from 75 to 91% (O'Leary et al., 2007). Erectile dysfunction appears to be the most common form of SD documented in MS. SD may be due to alteration of the ejaculatory reflex which may be affected by neurological conditions such as MS [27]
Spasticity
Spasticity is characterised by increased stiffness and slowness in limb movement, the development of certain postures, an association with weakness of voluntary muscle power, and with involuntary and sometimes painful spasms of limbs.[17]
Transverse Myelitis
Some MS patients develop rapid onset of numbness, weakness, bowel or bladder dysfunction, and/or loss of muscle function, typically in the lower half of the body. This is the result of MS attacking the spinal cord. The symptoms and signs depend upon the level of the spinal cord involved and the extent of the involvement.
Prognosis for complete recovery is generally poor. Recovery from transverse myelitis usually begins between weeks 2 and 12 following onset and may continue for up to 2 years in some patients and as many as 80% of individuals with transverse myelitis are left with lasting disabilities.
Tremor and Ataxia
Tremor is an unintentional, somewhat rhythmic, muscle movement involving to-and-fro movements (oscillations) of one or more parts of the body. It is the most common of all involuntary movements and can affect the hands, arms, head, face, vocal cords, trunk, and legs.
Ataxia is an unsteady and clumsy motion of the limbs or torso due to a failure of the gross coordination of muscle movements. People with ataxia experience a failure of muscle control in their arms and legs, resulting in a lack of balance and coordination or a disturbance of gait.
Tremor and ataxia are frequent in MS. They present in 25 to 60% of patients. They can be very disabling and embarrassing, and are difficult to manage.[28] The origin of tremor in MS is difficult to precise but it can be due to a mixture of different factors such as damage to the cerebellar connections, weakness, spasticity, etc.
Factors Triggering a Relapse
-
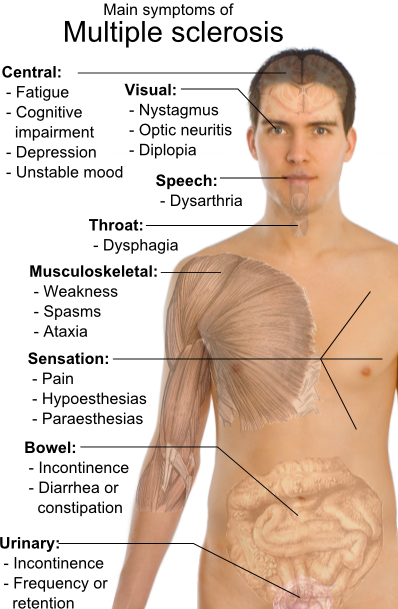
Main symptoms of multiple sclerosis.

Multiple sclerosis relapses are often unpredictable and can occur without warning with no obvious inciting factors. Some attacks, however, are preceded by common triggers. In general, relapses occur more frequently during spring and summer than during autumn and winter. Infections, such as the common cold, influenza, and gastroenteritis, increase the risk for a relapse.[29]
Emotional and physical stress may also trigger an attack,[30][31][32] as can severe illness of any kind. Statistically, there is no good evidence that either trauma or surgery trigger relapses.[33] People with MS can participate in sports, but they should probably avoid extremely strenuous exertion, such as marathon running. Heat can transiently increase symptoms, which is known as Uhthoff's phenomenon. This is why some people with MS avoid saunas or even hot showers. However, heat is not an established trigger of relapses.[34]
Pregnancy can directly affect the susceptibility for relapse. The last three months of pregnancy offer a natural protection against relapses. However, during the first few months after delivery, the risk for a relapse is increased 20%–40%. Pregnancy does not seem to influence long-term disability. Children born to mothers with MS are not at increased risk for birth defects or other problems.[35]
Many potential triggers have been examined and found not to influence relapse rates in MS. Influenza vaccination is safe, does not trigger relapses, and can therefore be recommended for people with MS. There is also no evidence that vaccines for hepatitis B, varicella, tetanus, or Bacille Calmette-Guerin (BCG—immunization for tuberculosis) increases the risk for relapse.[36]
References
- ↑ Weinshenker BG, Bass B, Rice GP, Noseworthy J, Carriere W, Baskerville J, Ebers GC (February 1989). "The natural history of multiple sclerosis: a geographically based study. I. Clinical course and disability". Brain. 112 ( Pt 1): 133–46. PMID 2917275.
- ↑ Hennessey A, Robertson NP, Swingler R, Compston DA (1999). "Urinary, faecal and sexual dysfunction in patients with multiple sclerosis". J. Neurol. 246 (11): 1027–32. PMID 10631634.
- ↑ Burguera-Hernández JA (2000). "[Urinary alterations in multiple sclerosis]". Revista de neurologia (in Spanish; Castilian). 30 (10): 989–92. PMID 10919202.
- ↑ Nour S, Svarer C, Kristensen JK, Paulson OB, Law I (2000). "Cerebral activation during micturition in normal men". Brain. 123 ( Pt 4): 781–9. PMID 10734009.
- ↑ Rao S, Leo G, Bernardin L, Unverzagt F (1991). "Cognitive dysfunction in multiple sclerosis. I. Frequency, patterns, and prediction". Neurology. 41 (5): 685–91. PMID 2027484.
- ↑ "Attention impairment in recently diagnosed multiple sclerosis". Eur J Neurol. 5 (1): 61–66. 1998. PMID 10210813.
- ↑ Achiron A, Barak Y (2003). "Cognitive impairment in probable multiple sclerosis". J Neurol Neurosurg Psychiatry. 74 (4): 443–6. PMID 12640060.
- ↑ Bobholz J, Rao S (2003). "Cognitive dysfunction in multiple sclerosis: a review of recent developments". Curr Opin Neurol. 16 (3): 283–8. PMID 12858063.
- ↑ Amato M, Ponziani G, Siracusa G, Sorbi S (2001). "Cognitive dysfunction in early-onset multiple sclerosis: a reappraisal after 10 years". Arch Neurol. 58 (10): 1602–6. PMID 11594918.
- ↑ Shawaryn M, Schultheis M, Garay E, Deluca J (2002). "Assessing functional status: exploring the relationship between the multiple sclerosis functional composite and driving". Arch Phys Med Rehabil. 83 (8): 1123–9. PMID 12161835.
- ↑ Sadovnick A, Remick R, Allen J, Swartz E, Yee I, Eisen K, Farquhar R, Hashimoto S, Hooge J, Kastrukoff L, Morrison W, Nelson J, Oger J, Paty D (1996). "Depression and multiple sclerosis". Neurology. 46 (3): 628–32. PMID 8618657.
- ↑ Patten S, Beck C, Williams J, Barbui C, Metz L (2003). "Major depression in multiple sclerosis: a population-based perspective". Neurology. 61 (11): 1524–7. PMID 14663036.
- ↑ Sadovnick A, Eisen K, Ebers G, Paty D (1991). "Cause of death in patients attending multiple sclerosis clinics". Neurology. 41 (8): 1193–6. PMID 1866003.
- ↑ Siegert R, Abernethy D (2005). "Depression in multiple sclerosis: a review". J. Neurol. Neurosurg. Psychiatr. 76 (4): 469–75. PMID 15774430.
- ↑ Bakshi R (2003). "Fatigue associated with multiple sclerosis: diagnosis, impact and management". Mult. Scler. 9 (3): 219–27. PMID 12814166.
- ↑ Mohr DC, Hart SL, Goldberg A (2003). "Effects of treatment for depression on fatigue in multiple sclerosis". Psychosomatic medicine. 65 (4): 542–7. PMID 12883103.
- ↑ 17.0 17.1 The Royal College of Physicians (2004). Multiple Sclerosis. National clinical guideline for diagnosis and management in primary and secondary care. Salisbury, Wiltshire: Sarum ColourView Group. ISBN 1 86016 182 0.Free full text(2004-08-13). Retrieved on 2007-10-01.
- ↑ Weinshenker BG, Bass B, Rice GP; et al. (1989). "The natural history of multiple sclerosis: a geographically based study. I. Clinical course and disability". Brain. 112 ( Pt 1): 133–46. PMID 2917275.
- ↑ Freeman JA (2001). "Improving mobility and functional independence in persons with multiple sclerosis". J. Neurol. 248 (4): 255–9. PMID 11374088.
- ↑ Stenager E, Knudsen L, Jensen K (1995). "Acute and chronic pain syndromes in multiple sclerosis. A 5-year follow-up study". Italian journal of neurological sciences. 16 (9): 629–32. PMID 8838789.
- ↑ Archibald CJ, McGrath PJ, Ritvo PG; et al. (1994). "Pain prevalence, severity and impact in a clinic sample of multiple sclerosis patients". Pain. 58 (1): 89–93. PMID 7970843.
- ↑ Clanet MG, Brassat D (2000). "The management of multiple sclerosis patients". Curr. Opin. Neurol. 13 (3): 263–70. PMID 10871249.
- ↑ Pöllmann W, Feneberg W, Erasmus LP (2004). "[Pain in multiple sclerosis--a still underestimated problem. The 1 year prevalence of pain syndromes, significance and quality of care of multiple sclerosis inpatients]". Der Nervenarzt (in German). 75 (2): 135–40. doi:10.1007/s00115-003-1656-5. PMID 14770283.
- ↑ Kerns RD, Kassirer M, Otis J (2002). "Pain in multiple sclerosis: a biopsychosocial perspective". Journal of rehabilitation research and development. 39 (2): 225–32. PMID 12051466.
- ↑ Brisman R (1987). "Trigeminal neuralgia and multiple sclerosis". Arch. Neurol. 44 (4): 379–81. PMID 3493757.
- ↑ Bayer DB, Stenger TG (1979). "Trigeminal neuralgia: an overview". Oral Surg. Oral Med. Oral Pathol. 48 (5): 393–9. PMID 226915.
- ↑ O'Leary, M., Heyman, R., Erickson, J., Chancellor, M.B.: Premature ejaculation and MS: A Review, Consortium of MS Centers, http://www.mscare.org, June 2007
- ↑ Koch M, Mostert J, Heersema D, De Keyser J (2007). "Tremor in multiple sclerosis". J. Neurol. 254 (2): 133–45. doi:10.1007/s00415-006-0296-7. PMID 17318714.
- ↑ Confavreux C (2002). "Infections and the risk of relapse in multiple sclerosis". Brain. 125 (Pt 5): 933–4. PMID 11960883.
- ↑ Buljevac D, Hop WC, Reedeker W; et al. (2003). "Self reported stressful life events and exacerbations in multiple sclerosis: prospective study". BMJ. 327 (7416): 646. doi:10.1136/bmj.327.7416.646. PMID 14500435.
- ↑ Brown RF, Tennant CC, Sharrock M, Hodgkinson S, Dunn SM, Pollard JD (2006). "Relationship between stress and relapse in multiple sclerosis: Part I. Important features". Mult. Scler. 12 (4): 453–64. PMID 16900759.
- ↑ Brown RF, Tennant CC, Sharrock M, Hodgkinson S, Dunn SM, Pollard JD (2006). "Relationship between stress and relapse in multiple sclerosis: Part II. Direct and indirect relationships". Mult. Scler. 12 (4): 465–75. PMID 16900760.
- ↑ Martinelli V (2000). "Trauma, stress and multiple sclerosis". Neurol. Sci. 21 (4 suppl 2): S849–52. PMID 11205361.
- ↑ Tataru N, Vidal C, Decavel P, Berger E, Rumbach L (2006). "Limited impact of the summer heat wave in France (2003) on hospital admissions and relapses for multiple sclerosis". Neuroepidemiology. 27 (1): 28–32. doi:10.1159/000094233. PMID 16804331.
- ↑ Worthington J, Jones R, Crawford M, Forti A (1994). "Pregnancy and multiple sclerosis--a 3-year prospective study". J. Neurol. 241 (4): 228–33. PMID 8195822.
- ↑ Confavreux C, Suissa S, Saddier P, Bourdès V, Vukusic S (2001). "Vaccinations and the risk of relapse in multiple sclerosis. Vaccines in Multiple Sclerosis Study Group". N. Engl. J. Med. 344 (5): 319–26. PMID 11172162.