Tooth impaction
|
WikiDoc Resources for Tooth impaction |
|
Articles |
|---|
|
Most recent articles on Tooth impaction Most cited articles on Tooth impaction |
|
Media |
|
Powerpoint slides on Tooth impaction |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Tooth impaction at Clinical Trials.gov Trial results on Tooth impaction Clinical Trials on Tooth impaction at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Tooth impaction NICE Guidance on Tooth impaction
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Tooth impaction Discussion groups on Tooth impaction Patient Handouts on Tooth impaction Directions to Hospitals Treating Tooth impaction Risk calculators and risk factors for Tooth impaction
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Tooth impaction |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Jaspinder Kaur, MBBS[2]
Overview
Tooth impaction can be defined as the interosseous position of the tooth which is completely or partially covered by mucosa and bone for more than 2 years following physiological eruption time. It can be readily confused with embedded and/or displaced teeth. Impacted teeth result from a situation in which an unerupted tooth is wedged against another tooth or teeth or located in a place where it cannot be erupted normally due to the palatal displacement. In contrast, an embedded tooth is an unerupted tooth that is covered usually completely with bone due to the lack of eruptive forces. The prevalent order of frequency of tooth impaction in the clinical practice includes mandibular and maxillary third molars, maxillary canines, mandibular premolars, mandibular canines, maxillary premolars, maxillary central incisors, maxillary lateral incisors, and mandibular second molars. Mandibular third molars are the most commonly found unerupted teeth, while maxillary third molars is the second most common. A diagnosis of impacted teeth is based on clinical symptoms, physical and radiographical examinations done by panoramic, occlusal, and periapical radiographs including cone-beam CT (CBCT) scans. The treatment plan should be based on clinical symptoms, location of the teeth, and a comprehensive examination of the impact of these teeth on neighboring teeth. Good orthodontic mechanics, surgical planning, and patient education are the mainstay of treatment. Surgical planning includes local anatomic concerns, anesthesia method, flap design, bone removal/coronal exposure, surgical instrumentation, bonding material characteristics, tooth ankylosis, and minimization of surgical complications. Additionally, all the potential complications should be explained to the patients before planned surgical and orthodontic interventions which might be sensory nerve damage leading to paresthesia, dry socket, infection, hemorrhage, bone loss, root resorption, and gingival recession around the treated teeth.
Classification
- Winter’s and Pell & Gregory’s systems proposed classifications based on the inclinations and positions of the third molars in relation to the dental longitudinal axis, occlusal plane, and ascending mandibular ramus.
Table 1: Winter’s and Pell & Gregory’s criteria[1] [2]
| Classification | Clinical description | Type |
|---|---|---|
| Pell and Gregory classification | Impaction depth: A relation of the cementoenamel junction (CEJ) of the third molar with the bone level is graded |
|
| Pell and Gregory classification | Ramus relationship: A position of the third molar crown's distal surface in relation to the anterior border of the ascending ramus is categorized |
|
| Winter’s classification | Impaction angulation: An angle between the longitudinal axis of the second and third molars is measured |
|
| Nature of overlying tissue | Clinical practice-based: It is used by most dental insurance companies by which surgeon charges for their services.[3] |
|
Pathophysiology
- Normal physiological process: Tooth eruption process involves complex interaction between osteoblasts, osteoclasts and dental follicular cell lines associated with the tooth germ which result in coordinated alveolar bone resorption and emergence of tooth within the oral cavity. Moreover, the normal development of the occlusion and craniofacial complex is largely dependent on the normal physiological eruption of teeth. Therefore, an eruption is the process by which a tooth moves axially from its follicle position in the bone into its final functional position in the oral cavity. Following clinical and radiographic assessment, if a tooth is not expected to erupt due to various underlying etiologies; it results in an impacted tooth which can be classified as entirely or partially unerupted teeth. [4] [5] [6]
- Pathological factors: Teeth may fail to erupt due to the lack of space, mechanical obstruction (idiopathic or pathological origin) or disruption to the eruptive mechanism itself. The most common impacted teeth are the third molars (wisdom teeth) as they are the last to erupt due to the inadequate space between the distal of the second mandibular molar and the anterior border of the ascending ramus of the mandible. In addition to it, dental caries and endodontic illnesses are more frequently observed in comparison to entirely unerupted teeth due to difficulties in reaching partially erupted teeth during oral hygiene.[4] [7]
- Ectopic tooth eruption: An impacted tooth is unable to fully erupt in its proper location because it is blocked by tissue, bone, or another tooth. However, sometimes an impacted tooth manages to erupt in the position of another tooth and causes developmental disturbance in the eruption pattern of permanent dentition. A tooth that erupts in this manner is called ectopic teeth which are displaced or incorrectly positioned. It is frequently caused by trauma, larger width of the permanent tooth, abnormal angulation of eruption of a molar, or delayed calcification of affected molars. The affected permanent molar may erupt at an angle to the normal eruption path, and thereby ceasing the eruption and causing the resorption of the neighboring deciduous tooth. [5] [8]
- Impacted canine: Shafer et al. suggested the following sequelae for canine impaction:[9]
- Labial or lingual malpositioning of the impacted tooth,
- Migration of the neighboring teeth and loss of arch length,
- Internal resorption,
- Dentigerous cyst formation,
- External root resorption of the impacted tooth, as well as the neighboring teeth,
- Infection particularly with partial eruption, and
- Referred pain and combinations of the above sequelae.
Etiology
- Various etiologies in the form of eruption pathway barrier or an ectopic position of the tooth results in the cessation of tooth eruption; and can be detected clinically or radiographically are elaborated in Table 2.
Table 2: Enlist the etiologic factors causing an impacted tooth[10]
| Localized |
|
| Systemic |
|
| Genetic |
- Impacted canines:
- The exact etiology of palatally displaced maxillary canines is unknown. Jacoby’s study showed that 85% of palatally impacted canines had sufficient space for eruption; and only 17% of labially impacted canines had enough space. Therefore, arch length discrepancy is thought to be a primary etiologic factor for labially impacted canines.[12] [13]
- Two major proposed theories associated with palatally displaced maxillary canines are as follows:[14]
- Guidance theory: It proposes that the canine erupts along the root of the lateral incisor serving as a guide, and the canine will not erupt in case of absent or malformed lateral incisor root. [15]
- Genetic theory: Genetic factors are considered as a primary origin of palatally displaced maxillary canines including other associated dental anomalies such as missing or small lateral incisors, enamel hypoplasia, infraocclusion of primary molars, aplasia of second premolars, and small maxillary lateral incisors.[16]
- Second molar: Andreasen and Kurol has classified the failure of the second molar eruption into three events etiologically, clinically and radiographically as explained in Table 3.[17]
Table 3: Events resulting in the failure of the second molar eruption
| Impaction[17] |
|
| Primary retention (unerupted and embedded teeth) [18] |
|
| Secondary retention (submerged, reimpaction, ankylosis) [19] [20] |
|
Differentiating Tooth Impaction from other Diseases
Table 4: Enlist the differential diagnosis for tooth impaction[21]
| Differential conditions | Characteristic features |
|---|---|
| Cleidocranial dysostosis[22] |
|
| Gardners syndrome[23] |
|
| Gorlin–Sedano syndrome |
|
| Yunis–Varon Syndrome |
|
| Osteogenesis Imperfecta |
|
Epidemiology and Demographics
- Impacted molars:
- Mandibular third molars (wisdom tooth) is the most commonly found unerupted teeth, while maxillary third molars are second most common.
- They have been more commonly found in the unilateral form than the bilateral; and more frequently seen in the mandible than the maxilla. [24]
- Prevalence: The incidence of impacted wisdom teeth is high with about 73% of the young adults in Europe which usually erupts between the ages of 17 and 21 years; and 72% of Swedish people aged 20 to 30 years having at least one impacted wisdom tooth. [25] [26] [27]
- Race predisposition: It has been reported that the third molar eruption varies with races; such as, in Nigeria mandibular third molars may erupt as early as 14 years; and in Europe it may erupt up to the age of 26 years.[28] [29]
- The impaction of other permanent teeth is also frequently reported with a prevalence ranging from 2.9% to 13.7%. The most commonly impacted teeth are the canines and second premolars in both jaws with different incidence rates. [30] [31]
- Impacted canines:
- Maxillary canines are the most commonly impacted teeth, second only to third molars. [32]
- Gender predilection: It is twice as common in females than males.
- Prevalence: Maxillary canine impaction occurs in approximately 2% of the population, and it's incidence in the maxilla is more than twice that of the mandible.
- Laterality: About 8% have bilateral impacted maxillary canines. [33]
- Location: Approximately one-third of impacted maxillary canines are located labially and two-thirds are located palatally. [13]
Risk Factors
- Age: An angle of the impacted tooth might increase in severity as the age progresses; and hence, an early diagnosis and treatment are recommended especially for the maxillary canines.
- Gender: Females have a higher predisposition to suffer from more severe teeth impaction especially of the maxillary canines because it is proposed that teeth erupt a little earlier in females than males. Thus, it is advised to diagnose impaction in females at an earlier stage to carry out any necessary preventive or interceptive orthodontic procedures.
- Microdontia: The maxillary lateral incisor microdontia is significantly associated with more severe tooth impaction, and emphasizes the tooth size investigations in patients especially with small laterals.
- Modern diet: It tends to be softer and does not offer a decided effort in mastication which subsequently results in the loss of growth stimulation of jaws and higher susceptibility of developing impacted and unerupted teeth. In addition to it, artificial feeding of babies and more consumption of sweet food by the children and youth further produces disproportion in the jaws and thus an impacted tooth.[25]
Natural history and Prognosis
- Whether the surgical removal of impacted tooth is for prophylactic, orthodontic and prosthetic reasons or for the diagnosis of several associated pathologies, it is one of the most performed dentoalveolar procedures in oral and maxillofacial surgery. In the United States, approximately 3 billion dollars are spent yearly on the extraction of impacted third molars. [34][35]
- However, the surgical removal might present with the complications in up to 15% of cases such as nerve injuries, post-operative infections, and iatrogenic mandibular fractures.[36]
- Hence, the surgical interventions among asymptomatic cases should weigh the risks of removal and benefits of tooth preservation.
Pericoronitis
- Pericoronitis: It is an inflammatory condition involving the soft tissue around a vertically positioned partially erupted third molar at or near the level of the occlusal plane; and among orthodontically treated cases with mesioangular position of the lower third molars. Similarly, the eruption process also causes minor gingivitis; and its symptoms may coincides with pericoronitis which creates the diagnosis issues for the dentists when it comes to lower impacted third molars.[37]
- Clinical signs and symptoms: The gingival tissues may be exquisitely tender and purulent causing significant discomfort and limits the jaw opening and chewing function. Most commonly, it presents with an acute and recurrent presentation; however, in some cases it may be chronic and painless with only intermittent symptoms. [38]
- Treatment:
- It is managed by the subgingival curettage to remove the plaque and foreign bodies followed by an irrigation with antimicrobials such as chlorhexidine or antibiotic therapy.
- In cases where the erupted or partially erupted upper third molar impinges on a lower operculum, extraction of the upper third molar may aid pain control and speed the healing process.
- Extraction of the lower third molar tooth is advised once infection and swelling have resolved, especially in the recurrent cases.[39]
Dental caries
- It is the most common hard-tissue disorder associated with third molar teeth.
- Risk factors: Its prevalence appears to increase over time due to the malposition of teeth which might never achieve complete eruption; and thus, making it difficult for dental restoration. [40]
- Treatment: Extraction is considered as the most efficacious treatment which involves an impacted third molar itself and/or the distal surface of the second molar in cases with third molar angulation. [41]
Odontogenic cysts and tumors
- Impacted teeth were found associated with lesions such as dentigerous cysts, unicystic ameloblastomas, ameloblastomas, ameloblastic fibromas, calcifying odontogenic cysts, adenomatoid odontogenic tumors, calcifying epithelial odontogenic tumors, ameloblastic fibro‑odontomas, keratocystic odontogenic tumors, central giant cell granuloma, odontomas, etc. [42]
- Dentigerous cyst, unicystic ameloblastoma, ameloblastoma, and ameloblastic fibroma are most frequent with the mandibular third molar teeth. [42]
- The incidence of large cysts and tumors occurring around impacted third molars is relatively rare showing a wide range from 0.001% on a biopsy to 11% when the diagnosis was clinically established. This wide variation indicates that the presence of a cyst is a weak indication for prophylactic extraction of impacted third molars.[43]
- However, in some cases the presence of odontogenic cysts and tumors in the third molar region can cause severe consequences such as pathological mandibular fracture and facial asymmetry. Hence, the surgical interventions among asymptomatic cases should weigh the risks of removal and benefits of tooth preservation.
Periodontitis
- Asymptomatic third molar teeth, especially lower third molar teeth, are frequently associated with pathologic periodontal conditions. The gingivae around these teeth harbor bacteria which serves as a reservoir for the development of the generalized periodontal disease. [44]
- The incidence of periodontitis has been reported to vary from 1% to 5% on the distal surface of the second molar which increases with age irrespective of the presence or absence of the third molars; and thus, a higher incidence of periodontitis has been observed among the older patients in relation to the impacted wisdom teeth. [43]
- Treatment: A periodontal probing should be an integral part of clinical assessment to adequately advise the patient about retention or extraction of third molars. However, the removal of third molars reduces the presence of periodontopathic bacteria at second molar sites and thus, further prevent or delay the onset of adult periodontitis. [45]
Root resorption
- It has been found that an impacted third molar left in-situ may cause resorption of the distal root of the adjacent second molar.[37]
- Some studies have also reported an association between root resorption at the apex and increasing age.
Miscellaneous
- Pain: It is the one of the most commonly reported complaint associated with impacted third molar whose prevalence varies greatly from 5% to 53%.[46]
- Cellulitis and osteomyelitis: Its incidence has been reported to be around 5%.
- Others: Functional disorders such as occlusal interference, cheek biting, mastication disorders, trismus and temporomandibular joint problems. [37]
Diagnosis
- Impacted teeth may remain asymptomatic and be incidentally diagnosed by routine dental radiography.
- It may be diagnosed via symptoms such as pressure, pain, or swelling; by physical examination with probing or direct visualization; or various associated pathologies such as caries, pericoronitis, cysts, tumors, and root resorption of the adjacent tooth.
- Clinical signs and symptoms: Caries, pain, swelling, paresthesia, periodontal pocket and pericoronitis.[46]
- Physical exam: Inspection and palpation of the temporomandibular joint and movement of the mandible, determination of mobility characteristics of lips and cheeks, size and contours of the tongue, and appearance of soft tissue overlying the impacted teeth.
- Radiographic evaluation: The most common radiographic methods in the diagnosis of tooth impaction are periapical or panoramic radiographs (OPG) which assess the root morphology, size of follicular sac, density of the surrounding bone, contact with the second molar, nature of overlying tissues, inferior alveolar nerve and vessels, relationship to body and ramus of mandible, relation with adjacent teeth and buccal to lingual position of the third molar.[47]

Source: Case courtesy of Dr Bruno Di Muzio, Radiopaedia.org, rID: 55220 - Impacted canine: Several radiographic exposures including occlusal films, panoramic views, and lateral cephalograms can help in evaluating the position of the canines; however, periapical films are considered most reliable in such cases. [33] [48] [49]
- Periapical films: It provides the clinician with a two-dimensional representation of the dentition and relates the canine to the neighboring teeth both mesiodistally and superoinferiorly. To evaluate the position of the canine buccolingually, a second periapical film should be obtained by the Tube-shift technique or Clark’s rule or (SLOB) or Buccal-object rule.
- Occlusal films: It helps to determine the buccolingual position of the impacted canine in conjunction with the periapical films provided that the image of the impacted canine is not superimposed on the other teeth.
- Extraoral films:
- Frontal and lateral cephalograms: These helps in determining the position of the impacted canine and its relationship with other facial structures such as the maxillary sinus and the floor of the nose.
- Panoramic films: These are employed as the primary imaging technique for the evaluation of impacted teeth and involved lesions in all the three planes of space and thus, helpful for diagnosis, follow‑up of tooth eruption, and treatment results. It is quite similar to the two periapical films in the tube-shift method with the source of radiation coming from behind the patient; and thus, the movements are reversed for the position. [42]
- Cone beam computed tomography (CBCT): It provides precise and accurate information better than conventional radiographs in terms of relation of the impacted tooth with the adjacent tooth, nasal floor, maxillary sinus, and mandibular canal in three dimensions. However, increased cost, time, radiation exposure, and medicolegal issues associated with using CBCT limit its routine use. [50]
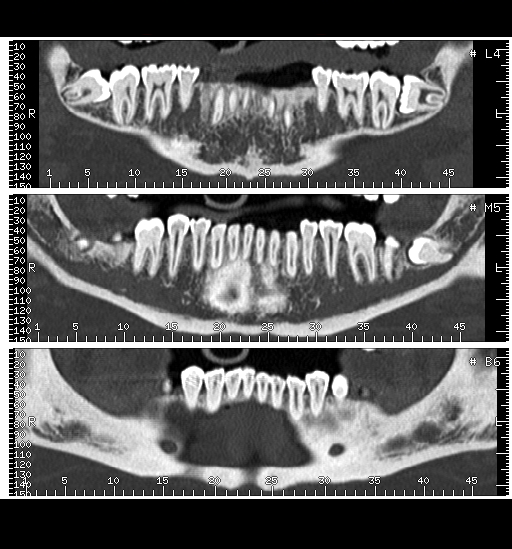
Source: Case courtesy of Dr Matthew Lukies, Radiopaedia.org, rID: 46588
- Impacted canine: Several radiographic exposures including occlusal films, panoramic views, and lateral cephalograms can help in evaluating the position of the canines; however, periapical films are considered most reliable in such cases. [33] [48] [49]
- Radiological changes:[46]
- Noninflammatory: Caries; Root resorption (internal or external); Interdental bone loss; Hyperplastic dental follicle
- Mild inflammatory: Pericoronal radiolucent areas suggesting pericoronitis; Periapical radiolucent areas suggesting abscess
- Severe inflammatory: Osteomyelitis


Treatment
- The management plan is based upon the presenting complaint and the history of the patient, the physical evaluation, radiographic assessment, the diagnosis, and the prognosis, which can be decided on the basis of etiology as a following: [5]
- Impaction: An early removal of physical barrier improves the chances of spontaneous eruption followed by orthodontic up righting if required.
- Primary retention: Unerupted tooth can be surgically repositioned following segment alveolar osteotomy. An involved teeth tend to ankylose if orthodontic force is applied. Prosthetic replacement of missing and unerupted tooth is the last resort. [51]
- Secondary retention: An immediate removal of affected molar followed by orthodontic alignment of neighboring teeth can be done in case secondary retention develops prior to growth spurt. An exposed tooth may be luxated to promotes eruption. Autotransplantation of third molar into the space created by missing teeth can be done.[52]
- Treatment difficulty index predicts an earlier the diagnosis and treatment of the impacted tooth, the less complicated and shorter the treatment duration; and further suggests that a severely impacted tooth can migrate and cross the midline with time indicating importance of an early diagnosis and treatment planning.
- The higher the rank of the position of the impacted tooth, the more difficult it is to align.
Modes of treatment
- Observation:
- A long‑term observation is recommended in an impacted mandibular the third molar embedded in bone with no perceptible to the follicle which might be seen in an older individual with no history and signs of associated pathology.[46]
- Most impacted teeth retain an erupting potential, and annual/biannual evaluation would be recommended if no indications for direct surgical management seen.
- Exposure: It is considered if the probability of eruption into useful occlusion is higher but obstructed by follicle, sclerotic bone, hypertrophic soft tissue, or odontoma. An exposure of a blocked third molar may be considered in absent second molar cases.
- Transplantation of a mandibular third molar: The variety of crown and root shape on the impacted third molar make them suitable for transplantation to other molar sites, bicuspid and even the cuspid locations depending on the anatomy of the coronal and radicular surface.
- Removal: The primary reason to remove a tooth is to correct associated pathology and to intercept reasonably expected pathological process. There are 3 main surgical options in the management of impacted teeth: [43] [53]
- Extraction of an impacted tooth
- Extraction of an adjacent tooth
- Non-extraction treatment: It involves an orthodontic space opening in order to align the teeth, to open the space for the impacted tooth and to enhance the natural eruption process followed by the surgical exposure.
Indications for Mandibular Third Molar Extraction
- Various conditions are indications for the removal of impacted third molars which are as follows in Table 5:
Table 5: List of indications for impacted tooth extraction[54]
| Indications for extraction of impacted third molars |
|---|
|
Impacted canine
- The management of impacted canines is important in terms of esthetics, function, and to reduce the frequency of ectopic eruption with subsequent impaction of the maxillary canine.[49]
- Firstly, the simplest interceptive procedure to prevent impaction of permanent canines in the early diagnosis and timely extraction of the primary canines which allows the permanent canines to become upright and erupt properly into the dental arch provided sufficient space is available to accommodate them.
- Secondly, in the absence of prevention, dentists should consider orthodontic treatment followed by surgical exposure of the canine to bring it into occlusion. The most common methods used to bring palatally impacted canines into occlusion are surgically exposing the teeth and allowing them to erupt naturally during early or late mixed dentition and surgically exposing the teeth and placing a bonded attachment to and using orthodontic forces to move the tooth. [55]
- Orthodontists have recommended to first create adequate space in the dental arch to accommodate the impacted canine and then surgically expose the tooth to give them access so that they can apply mechanical force to erupt the tooth.
- The most efficient way to make impacted canines erupt is to use closed-coil springs with eyelets as long as no obstacles impede the path of the canine.
- Orthodontists may consider treatment alternatives such as autotransplantation or restoration in collaboration with other specialists such as oral surgeons, periodontists, and prosthodontists.
Post extraction risks and complications
- Several local and general factors which include tooth position, age of the patient, health status, knowledge and experience of the dental surgeon, and surgical equipment used can lead to the various post-extraction risks and complications enlisted in the following Table 6:
Table 6: Enlists post extraction risks and complications [54]
| Post extraction risks and complications |
|---|
|
References
- ↑ Pell GJ, Gregory GT. Impacted mandibular third molars: Classification and Impacted mandibular third molars: Classification and modified technique for removal. Dent Dig 1933;39:330‑8.
- ↑ Almendros-Marqués, Nieves; Berini-Aytés, Leonardo; Gay-Escoda, Cosme (2006). "Influence of lower third molar position on the incidence of preoperative complications". Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 102 (6): 725–732. doi:10.1016/j.tripleo.2006.01.006. ISSN 1079-2104.
- ↑ Gbotolorun, OM; Olojede, ACO; Arotiba, GT; Ladeinde, AL; Akinwande, JA; Bamgbose, BO (2007). "Impacted mandibular third molars: Presentationn and postoperative complications at the Lagos University Teaching Hospital". Nigerian Quarterly Journal of Hospital Medicine. 17 (1). doi:10.4314/nqjhm.v17i1.12537. ISSN 0189-2657.
- ↑ 4.0 4.1 Raghoebar, G. M.; Boering, G.; Vissink, A.; Stegenga, B. (1991). "Eruption disturbances of permanent molars: a review". Journal of Oral Pathology and Medicine. 20 (4): 159–66. doi:10.1111/j.1600-0714.1991.tb00913.x. ISSN 0904-2512.
- ↑ 5.0 5.1 5.2 Kaur M, Shefali S. Molar Impactions: Etiology, Implications and Treatment Modalities with Presentation of an Unusual Case. J Orofac Res 2012;2(3):171-173.
- ↑ Laganà, G; Venza, N; Borzabadi-Farahani, A; Fabi, F; Danesi, C; Cozza, P (2017). "Dental anomalies: prevalence and associations between them in a large sample of non-orthodontic subjects, a cross-sectional study". BMC Oral Health. 17 (1). doi:10.1186/s12903-017-0352-y. ISSN 1472-6831.
- ↑ 7.0 7.1 Kaczor-Urbanowicz, Karolina; Zadurska, Małgorzata; Czochrowska, Ewa (2016). "Impacted Teeth: An Interdisciplinary Perspective". Advances in Clinical and Experimental Medicine. 25 (3): 575–585. doi:10.17219/acem/37451. ISSN 1899-5276.
- ↑ Yaseen, SyedMohammed; Naik, Saraswati; Uloopi, KS (2011). "Ectopic eruption - A review and case report". Contemporary Clinical Dentistry. 2 (1): 3. doi:10.4103/0976-237X.79289. ISSN 0976-237X.
- ↑ Shafer WG, Hine MK, Levy BM, editors. A textbook of oral pathology. 2nd ed. Philadelphia: WB Saunders; 1963. p. 2-75
- ↑ Power, Susan M.; Short, Mary B. E. (2019). "An Investigation into the Response of Palatally Displaced Canines to the Removal of Deciduous Canines and an Assessment of Factors Contributing to Favourable Eruption". British Journal of Orthodontics. 20 (3): 215–223. doi:10.1179/bjo.20.3.215. ISSN 0301-228X.
- ↑ Gecgelen M, Aksoy A. Etiology, diagnosis and treatment of impacted teeth. Smyrna Med J 2012;2:64‑8.
- ↑ Jacoby, Harry (1983). "The etiology of maxillary canine impactions". American Journal of Orthodontics. 84 (2): 125–132. doi:10.1016/0002-9416(83)90176-8. ISSN 0002-9416.
- ↑ 13.0 13.1 Mitchell, Laura. An Introduction to orthodontics. Oxford New York: Oxford University Press, 2007. Print.
- ↑ Richardson G, Russell KA (2000). "A review of impacted permanent maxillary cuspids--diagnosis and prevention". J Can Dent Assoc. 66 (9): 497–501. PMID 11070629.
- ↑ Becker, Adrian. The orthodontic treatment of impacted teeth. Abingdon, Oxon New York: Informa Healthcare Distributed in US and Canada by Thieme New York, 2007. Print.
- ↑ Peck S, Peck L, Kataja M (1994). "The palatally displaced canine as a dental anomaly of genetic origin". Angle Orthod. 64 (4): 249–56. doi:10.1043/0003-3219(1994)064<0249:WNID>2.0.CO;2. PMID 7978519.
- ↑ 17.0 17.1 Andreasen JO, Kurol J. The impacted first and second molar. In: Andreasen JO, Petersen JK LD (Eds). Textbook and color atlas of tooth impactions. Copenhage: Munksgaard 1977;197-218.
- ↑ Oliver RG, Richmond S, Hunter B. Submerged permanent molars: Four case reports. Br Dent J 1986;160:128-30.
- ↑ Raghoebar, G. M.; Boering, G.; Jansen, H.W.B.; Vissink, A. (1989). "Secondary retention of permanent molars: a histologic study". Journal of Oral Pathology and Medicine. 18 (8): 427–431. doi:10.1111/j.1600-0714.1989.tb01338.x. ISSN 0904-2512.
- ↑ Reid DJ. Incomplete eruption of the first permanent molar in two generations of the same family. Br Dent J 1954;96:272-73.
- ↑ Sujatha, G; Sivapathasundharam, B; Sivakumar, G; Nalinkumar, S; Ramasamy, M; Prasad, TSrinivasa (2012). "Idiopathic multiple impacted unerupted teeth: Case report and discussion". Journal of Oral and Maxillofacial Pathology. 16 (1): 125. doi:10.4103/0973-029X.92989. ISSN 0973-029X.
- ↑ Kirson, Lyle E.; Scheiber, Robert E.; Tomaro, A.J. (1982). "Multiple impacted teeth in cleidocranial dysostosis". Oral Surgery, Oral Medicine, Oral Pathology. 54 (5): 604. doi:10.1016/0030-4220(82)90204-3. ISSN 0030-4220.
- ↑ Bradley JF, Orlowski WA (1977). "Multiple osteomas, impacted teeth and odontomas--a case report of Gardner's Syndrome". J N J Dent Assoc. 48 (2): 32–3. PMID 275470.
- ↑ Varpio M, Wellfelt B (1988). "Disturbed eruption of the lower second molar: clinical appearance, prevalence, and etiology". ASDC J Dent Child. 55 (2): 114–8. PMID 3162471.
- ↑ 25.0 25.1 Matsuyama, Junko; Kinoshita-Kawano, Shoko; Hayashi-Sakai, Sachiko; Mitomi, Tomoe; Sano-Asahito, Tomiko (2015). "Severe Impaction of the Primary Mandibular Second Molar Accompanied by Displacement of the Permanent Second Premolar". Case Reports in Dentistry. 2015: 1–5. doi:10.1155/2015/582462. ISSN 2090-6447.
- ↑ Bouloux, Gary F.; Steed, Martin B.; Perciaccante, Vincent J. (2007). "Complications of Third Molar Surgery". Oral and Maxillofacial Surgery Clinics of North America. 19 (1): 117–128. doi:10.1016/j.coms.2006.11.013. ISSN 1042-3699.
- ↑ Hugoson A, Kugelberg CF (1988). "The prevalence of third molars in a Swedish population. An epidemiological study". Community Dent Health. 5 (2): 121–38. PMID 3165039.
- ↑ Carvalho, Ricardo Wathson F.; do Egito Vasconcelos, Belmiro Cavalcanti (2011). "Assessment of Factors Associated With Surgical Difficulty During Removal of Impacted Lower Third Molars". Journal of Oral and Maxillofacial Surgery. 69 (11): 2714–2721. doi:10.1016/j.joms.2011.02.097. ISSN 0278-2391.
- ↑ Pahkala, Riitta; Pahkala, Ari; Laine, Tellervo (2009). "Eruption pattern of permanent teeth in a rural community in northeastern Finland". Acta Odontologica Scandinavica. 49 (6): 341–349. doi:10.3109/00016359109005930. ISSN 0001-6357.
- ↑ Uslu, Ozge; Akcam, M. Okan; Evirgen, Sehrazat; Cebeci, Ilker (2009). "Prevalence of dental anomalies in various malocclusions". American Journal of Orthodontics and Dentofacial Orthopedics. 135 (3): 328–335. doi:10.1016/j.ajodo.2007.03.030. ISSN 0889-5406.
- ↑ Fardi, A.; Kondylidou-Sidira, A.; Bachour, Z.; Parisis, N.; Tsirlis, A. (2011). "Incidence of impacted and supernumerary teeth-a radiographicStudy in a North Greek population". Medicina Oral Patología Oral y Cirugia Bucal: e56–e61. doi:10.4317/medoral.16.e56. ISSN 1698-6946.
- ↑ Litsas, George (2011). "A Review of Early Displaced Maxillary Canines: Etiology, Diagnosis and Interceptive Treatment". The Open Dentistry Journal. 5 (1): 39–47. doi:10.2174/1874210601105010039. ISSN 1874-2106.
- ↑ 33.0 33.1 33.2 Bishara, Samir E.; Ortho., D. (1992). "Impacted maxillary canines: A review". American Journal of Orthodontics and Dentofacial Orthopedics. 101 (2): 159–171. doi:10.1016/0889-5406(92)70008-X. ISSN 0889-5406.
- ↑ Fuster Torres MA, Gargallo Albiol J, Berini Aytés L, Gay Escoda C (2008). "Evaluation of the indication for surgical extraction of third molars according to the oral surgeon and the primary care dentist. Experience in the Master of Oral Surgery and Implantology at Barcelona University Dental School". Med Oral Patol Oral Cir Bucal. 13 (8): E499–504. PMID 18667984.
- ↑ Friedman, Jay W. (2007). "The Prophylactic Extraction of Third Molars: A Public Health Hazard". American Journal of Public Health. 97 (9): 1554–1559. doi:10.2105/AJPH.2006.100271. ISSN 0090-0036.
- ↑ Gbotolorun, Olalekan Micah; Arotiba, Godwin Toyin; Ladeinde, Akinola Ladipo (2007). "Assessment of Factors Associated With Surgical Difficulty in Impacted Mandibular Third Molar Extraction". Journal of Oral and Maxillofacial Surgery. 65 (10): 1977–1983. doi:10.1016/j.joms.2006.11.030. ISSN 0278-2391.
- ↑ 37.0 37.1 37.2 Song, F; Landes, D P; Glenny, A M; Sheldon, T A (1997). "Prophylactic removal of impacted third molars: an assessment of published reviews". British Dental Journal. 182 (9): 339–346. doi:10.1038/sj.bdj.4809378. ISSN 0007-0610.
- ↑ Laine, Mikael; Ventä, Irja; Hyrkäs, Tapio; Ma, Jian; Konttinen, Yrjö T. (2003). "Chronic inflammation around painless partially erupted third molars". Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 95 (3): 277–282. doi:10.1067/moe.2003.86. ISSN 1079-2104.
- ↑ https://www.nice.org.uk/guidance/ta1/resources/guidance-on-the-extraction-of-wisdom-teeth-pdf-63732983749
- ↑ Fisher, Elda L.; Garaas, Rachel; Blakey, George H.; Offenbacher, Steven; Shugars, Daniel A.; Phillips, Ceib; White, Raymond P. (2012). "Changes Over Time in the Prevalence of Caries Experience or Periodontal Pathology on Third Molars in Young Adults". Journal of Oral and Maxillofacial Surgery. 70 (5): 1016–1022. doi:10.1016/j.joms.2011.10.016. ISSN 0278-2391.
- ↑ Campbell, John H. (2013). "Pathology Associated with the Third Molar". Oral and Maxillofacial Surgery Clinics of North America. 25 (1): 1–10. doi:10.1016/j.coms.2012.11.005. ISSN 1042-3699.
- ↑ 42.0 42.1 42.2 Mortazavi, Hamed; Baharvand, Maryam (2016). "Jaw lesions associated with impacted tooth: A radiographic diagnostic guide". Imaging Science in Dentistry. 46 (3): 147. doi:10.5624/isd.2016.46.3.147. ISSN 2233-7822.
- ↑ 43.0 43.1 43.2 Lytle JJ (1995). "Etiology and indications for the management of impacted teeth". Northwest Dent. 74 (6): 23–32. PMID 9462087.
- ↑ White, Raymond P.; Madianos, Phoebus N.; Offenbacher, Steven; Phillips, Ceib; Blakey, George H.; Haug, Richard H.; Marciani, Robert D. (2002). "Microbial complexes detected in the second/third molar region in patients with asymptomatic third molars". Journal of Oral and Maxillofacial Surgery. 60 (11): 1234–1240. doi:10.1053/joms.2002.35718. ISSN 0278-2391.
- ↑ Rajasuo, Ari; Meurmarr, Jukka H.; Murtomaa, Heikki (1993). "Periodontopathic bacteria and salivary microbes before and after extraction of partly erupted third molars". European Journal of Oral Sciences. 101 (2): 87–91. doi:10.1111/j.1600-0722.1993.tb01094.x. ISSN 0909-8836.
- ↑ 46.0 46.1 46.2 46.3 Santosh, P (2015). "Impacted mandibular third molars: Review of literature and a proposal of a combined clinical and radiological classification". Annals of Medical and Health Sciences Research. 5 (4): 229. doi:10.4103/2141-9248.160177. ISSN 2141-9248.
- ↑ Khan, Imran; Halli, Rajshekhar; Gadre, Pushkar; Gadre, Kiran S. (2011). "Correlation of Panoramic Radiographs and Spiral CT Scan in the Preoperative Assessment of Intimacy of the Inferior Alveolar Canal to Impacted Mandibular Third Molars". Journal of Craniofacial Surgery. 22 (2): 566–570. doi:10.1097/SCS.0b013e3182077ac4. ISSN 1049-2275.
- ↑ Ericson, Sune; Kurol, Jüri (1987). "Radiographic examination of ectopically erupting maxillary canines". American Journal of Orthodontics and Dentofacial Orthopedics. 91 (6): 483–492. doi:10.1016/0889-5406(87)90005-9. ISSN 0889-5406.
- ↑ 49.0 49.1 Juvvadi, ShubhakerRao; Medapati Rama, Haranath Reddy; Anche, Sampath; Manne, Ranjit; Gandikota, ChandraSekhar (2012). "Impacted canines: Etiology, diagnosis, and orthodontic management". Journal of Pharmacy and Bioallied Sciences. 4 (6): 234. doi:10.4103/0975-7406.100216. ISSN 0975-7406.
- ↑ Chandak, Shruti (2014). "Comparative Study of Dentascan and Radiography for Radiological Evaluation of Impacted Teeth". JOURNAL OF CLINICAL AND DIAGNOSTIC RESEARCH. doi:10.7860/JCDR/2014/7997.4618. ISSN 2249-782X.
- ↑ Proffit, William R.; Vig, Katherine W.L. (1981). "Primary failure of eruption: A possible cause of posterior open-bite". American Journal of Orthodontics. 80 (2): 173–190. doi:10.1016/0002-9416(81)90217-7. ISSN 0002-9416.
- ↑ Kaban, Leonard B.; Needleman, Howard L.; Hertzberg, Jack (1976). "Idiopathic failure of eruption of permanent molar teeth". Oral Surgery, Oral Medicine, Oral Pathology. 42 (2): 155–163. doi:10.1016/0030-4220(76)90118-3. ISSN 0030-4220.
- ↑ Becker, Adrian. Orthodontic treatment of impacted teeth. Chichester, West Sussex, UK Ames, Iowa: Wiley-Blackwell, 2012. Print
- ↑ 54.0 54.1 Dodson TB, Susarla SM (2010). "Impacted wisdom teeth". BMJ Clin Evid. 2010. PMC 2907590. PMID 21729337.
- ↑ Bedoya, Marisela M.; Park, Jae Hyun (2009). "A Review of the Diagnosis and Management of Impacted Maxillary Canines". The Journal of the American Dental Association. 140 (12): 1485–1493. doi:10.14219/jada.archive.2009.0099. ISSN 0002-8177.