Osteosarcoma pathophysiology: Difference between revisions
No edit summary |
|||
| Line 32: | Line 32: | ||
*Characteristic features on microscopic analysis are variable depending on the osteosarcoma subtype: | *Characteristic features on microscopic analysis are variable depending on the osteosarcoma subtype: | ||
{| style="border: 0px; font-size: 90%; margin: 3px; width: 1000px" align=center | |||
|valign=top| | |||
|+ | |||
! style="background: #4479BA; width: 200px;" | {{fontcolor|#FFF|Subtype}} | |||
! style="background: #4479BA; width: 400px;" | {{fontcolor|#FFF|X-Ray findings}} | |||
|- | |||
| style="padding: 5px 5px; background: #DCDCDC; font-weight: bold" | | |||
:Telangiectatic osteosarcoma | |||
| style="padding: 5px 5px; background: #F5F5F5;" | | |||
*Most osteosarcomas have a small telangiectatic component but in order to classify as a telangiectatic osteosarcoma the telangiectatic component should comprise more than 90%.<ref name=radio2> Osteosarcoma. Dr Yuranga Weerakkody◉ et al. Radiopaedia.org 2015. http://radiopaedia.org/articles/telangiectatic-osteosarcoma</ref> | |||
*Most of the tumor comprises of large blood filled spaces separated by thin bony septations. | |||
*Microscopically, the tumor consist of vascular sinusoids surrounded by thin septae, osteoid matrix and cells with significant pleomorphism and high mitotic rate. | |||
|- | |||
| style="padding: 5px 5px; background: #DCDCDC;font-weight: bold" | | |||
:Low grade osteosarcoma | |||
| style="padding: 5px 5px; background: #F5F5F5;" | | |||
*Histologically it is a low grade tumor which occurs in medullary canal of long bones.<ref name=radio2> Osteosarcoma.Dr Yuranga Weerakkody◉ and Dr Prashant Mudgal et al. Radiopaedia.org 2015. http://radiopaedia.org/articles/low-grade-osteosarcoma</ref> | |||
*It contains osseous matrix with blend fibrous stroma and there is variable amount of bone production. | |||
*Histologic pattern is similar to [[fibrous dysplasia]] and low grade parosteal osteosarcoma. | |||
|- | |||
| style="padding: 5px 5px; background: #DCDCDC;font-weight: bold" | | |||
:Periosteal osteosarcoma | |||
| style="padding: 5px 5px; background: #F5F5F5;" | | |||
*Periosteal osteosarcoma arise from the inner germinative layer of [[periosteum]].<ref name=radio2> Osteosarcoma. Dr Henry Knipe◉ and Dr Sam Kyle et al.Radiopaedia.org 2015. http://radiopaedia.org/articles/periosteal-osteosarcoma</ref> | |||
*Cytologic grade of this tumor is higher than parosteal osteosarcoma and lower than conventional osteosarcomas, so it is considered as intermediate grade osteosarcoma (grade 2). | |||
*It predominantly contains chondroid matrix. | |||
|- | |||
| style="padding: 5px 5px; background: #DCDCDC;font-weight: bold" | | |||
:Intracortical osteosarcoma | |||
| style="padding: 5px 5px; background: #F5F5F5;" | | |||
*Intracortical osteosarcoma is a low grade tumor of cortical bones and it typically does not extend into [[medullary canal]] and surrounding soft tissue until late stage of the disease.<ref name=radio2> Osteosarcoma. Dr Prashant Mudgal et al. Radiopaedia.org 2015. http://radiopaedia.org/articles/intracortical-osteosarcoma</ref> | |||
*Histologically characterazied as a sclerosing variant of the osteosarcoma contains [[osteoid]] matrix with few fibroblastic foci within and mild degree of cellular atypia. | |||
|- | |||
| style="padding: 5px 5px; background: #DCDCDC;font-weight: bold" | | |||
:Parosteal osteosarcoma | |||
| style="padding: 5px 5px; background: #F5F5F5;" | | |||
*Parosteal osteosarcoma originates from the outer fibrous layer of [[periosteum]].<ref name=radio2> Osteosarcoma.Dr Frank Gaillard◉ et al.Radiopaedia.org 2015. http://radiopaedia.org/articles/parosteal-osteosarcoma-1</ref> | |||
*They are composed of a dense osteoid component attached to the outer cortex over a narrow zone. | |||
*It exhibits extensive bone matrix and minimal fibroblastic cellular atypia, and as such is considered to be a low grade tumor. | |||
|- | |||
| style="padding: 5px 5px; background: #DCDCDC;font-weight: bold" | | |||
:Extraskeletal osteosarcoma | |||
| style="padding: 5px 5px; background: #F5F5F5;" | | |||
*Grossly, it is a well defined lesion with hemorrhagic and necrotic areas within.<ref name=radio2> Osteosarcoma.Dr Amir Rezaee◉ and Dr Prashant Mudgal et al. Radiopaedia.org 2015. http://radiopaedia.org/articles/extra-skeletal-osteosarcoma-1</ref> | |||
*Microscopically, it is typically a high grade [[spindle cell]] malignancy with [[osteoid]] and chondroid matrix. | |||
*The histologic appearance of extraskeletal osteosarcoma resembles malignant [[fibrous histiocytoma]], osteoblastic osteosarcoma and chondroblastic osteosarcoma. | |||
|- | |||
|} | |||
===Telanagiectatic osteosarcoma=== | ===Telanagiectatic osteosarcoma=== | ||
Revision as of 14:40, 1 October 2015
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [2];Associate Editor(s)-in-Chief: Suveenkrishna Pothuru, M.B,B.S. [3]
|
Osteosarcoma Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Osteosarcoma pathophysiology On the Web |
|
American Roentgen Ray Society Images of Osteosarcoma pathophysiology |
|
Risk calculators and risk factors for Osteosarcoma pathophysiology |
Overview
The osteosarcomas may be localized at the end of the long bones (commonly in the metaphysis). Most often it affects the upper end of tibia, humerus, or lower end of femur. On gross pathology, areas of bone formation, hemorrhage, fibrosis, and cystic degeneration on cut surface are characteristic findings of osteosarcoma. On microscopic histopathological analysis, presence of osteoid within the tumor, pleomorphic cells, anaplastic cells, and atypical mitoses are characteristic findings of osteosarcoma. Osteosarcoma may be associated with hereditary syndromes such as Li-Fraumeni syndrome and Rothmund-Thomson Syndrome.
Pathophysiology
The osteosarcomas may be localized at the end of the long bones (commonly in the metaphysis). Most often it affects the upper end of tibia, humerus, or lower end of femur. Osteosarcomas tend to occur at the sites of bone growth, presumably because proliferation makes osteoblastic cells in this region prone to acquire mutations that could lead to transformation of cells (the RB gene and p53 gene are commonly involved).
Gross Pathology
- Macroscopically, osteosarcomas are solid, hard, and bulky tumors.
- Heterogeneous cut surface demonstrates areas of hemorrhage, fibrosis and cystic degeneration.
- Areas of bone formation are characteristic of osteosarcomas, with the degree of bone formation varying widely.
- The tumor is irregular ("fir-tree" or "sun-burst" appearance on X-ray examination) due to the tumor spicules of calcified bone radiating in right angles. These right angles form what is known as Codman's triangle, which is characteristic but not diagnostic of osteosarcoma. Surrounding tissues are infiltrated.
.jpg) |
Microscopic Pathology
- On microscopic histopathological analysis, characteric feature of osteosarcoma is presence of osteoid (bone formation) within the tumor.
- Tumor cells are very pleomorphic, anaplastic, some are giant, and numerous atypical mitoses.
- These cells produce osteoid describing irregular trabeculae (amorphous, eosinophilic/pink) with or without central calcification (hematoxylinophilic/blue, granular) - tumor bone.
- Tumor cells are included in the osteoid matrix. Depending on the features of the tumor cells present (whether they resemble bone cells, cartilage cells or fibroblast cells), the tumor can be subclassified. Presence of immature blood vessels (sarcomatous vessels lacking endothelial cells) favors the bloodstream metastasizing.
-
![Histology of conventional osteosarcoma[1]](/images/5/51/Osteosarcoma-conventional-histology_%281%29.jpg)
Histology of conventional osteosarcoma[1]
-
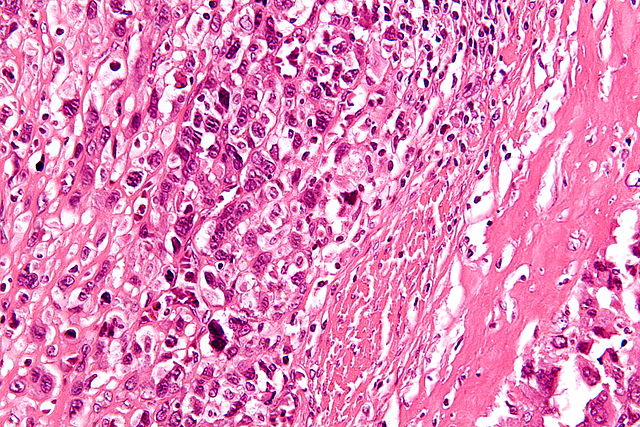
High-magnification micrograph showing osteoid formation in an osteosarcoma H&E stain
![Histology of conventional osteosarcoma[1]](/index.php/File:Osteosarcoma-conventional-histology_(1).jpg)

- Characteristic features on microscopic analysis are variable depending on the osteosarcoma subtype:
| Subtype | X-Ray findings |
|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
Telanagiectatic osteosarcoma
- Most osteosarcomas have a small telangiectatic component but in order to classify as a telangiectatic osteosarcoma the telangiectatic component should comprise more than 90%.[2]
- Most of the tumor comprises of large blood filled spaces separated by thin bony septations.
- Microscopically, the tumor consist of vascular sinusoids surrounded by thin septae, osteoid matrix and cells with significant pleomorphism and high mitotic rate.
Low grade osteosarcoma
- Histologically it is a low grade tumor which occurs in medullary canal of long bones.[2]
- It contains osseous matrix with blend fibrous stroma and there is variable amount of bone production.
- Histologic pattern is similar to fibrous dysplasia and low grade parosteal osteosarcoma.
Periosteal osteosarcoma
- Periosteal osteosarcoma arise from the inner germinative layer of periosteum.[2]
- Cytologic grade of this tumor is higher than parosteal osteosarcoma and lower than conventional osteosarcomas, so it is considered as intermediate grade osteosarcoma (grade 2).
- It predominantly contains chondroid matrix.
Intracortical osteosarcoma
- Intracortical osteosarcoma is a low grade tumor of cortical bones and it typically does not extend into medullary canal and surrounding soft tissue until late stage of the disease.[2]
- Histologically characterazied as a sclerosing variant of the osteosarcoma contains osteoid matrix with few fibroblastic foci within and mild degree of cellular atypia.
Parosteal osteosarcoma
- Parosteal osteosarcoma originates from the outer fibrous layer of periosteum.[2]
- They are composed of a dense osteoid component attached to the outer cortex over a narrow zone.
- It exhibits extensive bone matrix and minimal fibroblastic cellular atypia, and as such is considered to be a low grade tumor.
Extraskeletal osteosarcoma
- Grossly, it is a well defined lesion with hemorrhagic and necrotic areas within.[2]
- Microscopically, it is typically a high grade spindle cell malignancy with osteoid and chondroid matrix.
- The histologic appearance of extraskeletal osteosarcoma resembles malignant fibrous histiocytoma, osteoblastic osteosarcoma and chondroblastic osteosarcoma.
Genetics
Hereditary syndromes of osteosarcoma have been identified:[3]
- RECQL4 gene mutations
- RB1 gene mutations (also implicated in retinoblastoma)
- Li-Fraumeni syndrome
- Rothmund-Thomson Syndrome
These syndromes are extremely rare within the Osteosarcoma diagnosis, and probably represent less than 0.5% of those diagnosed.
-
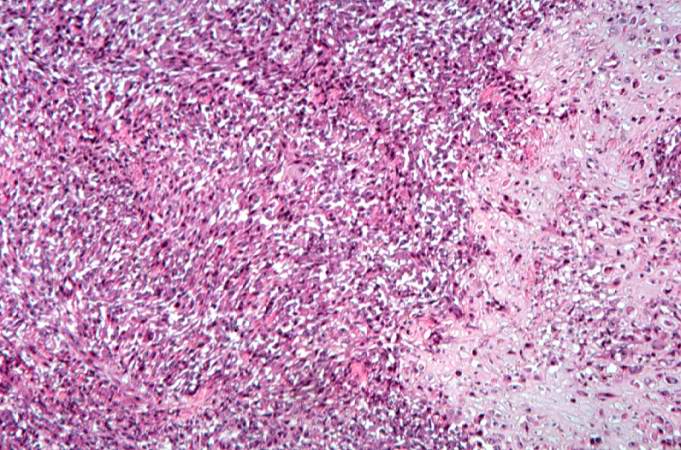
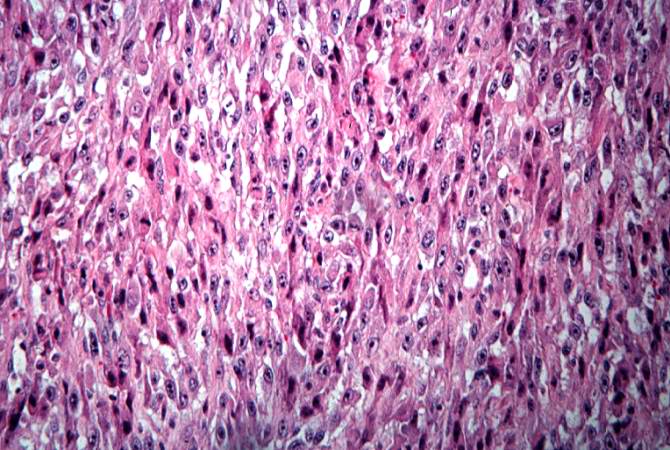
This high-power photomicrograph demonstrates the cellular growth pattern. Note that the cells are fusiform and they grow in sheets.
-
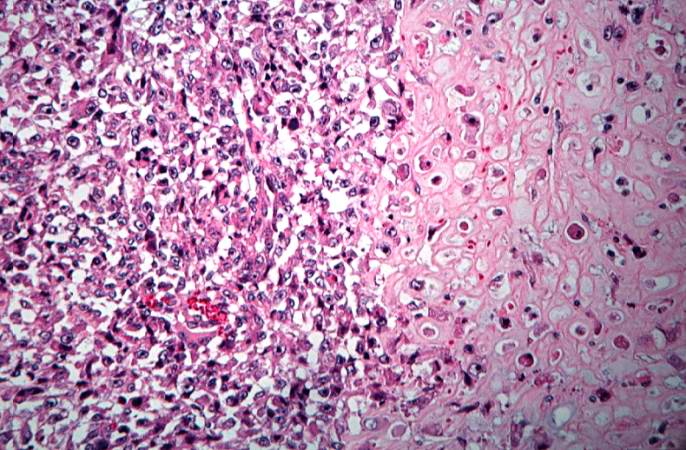
This high-power photomicrograph demonstrates the growth pattern and the cell morphology.
-
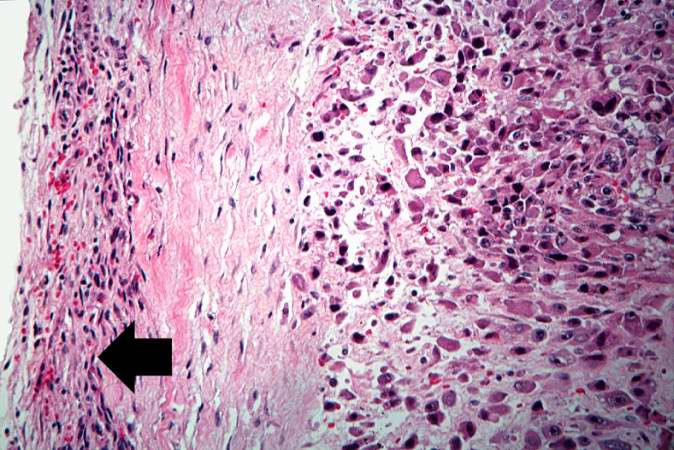
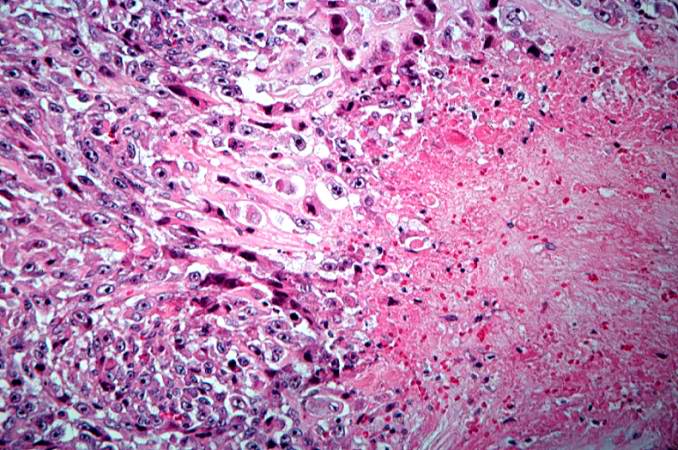
This is a high-power photomicrograph of the tumor cell morphology and the periosteum (arrow).
-
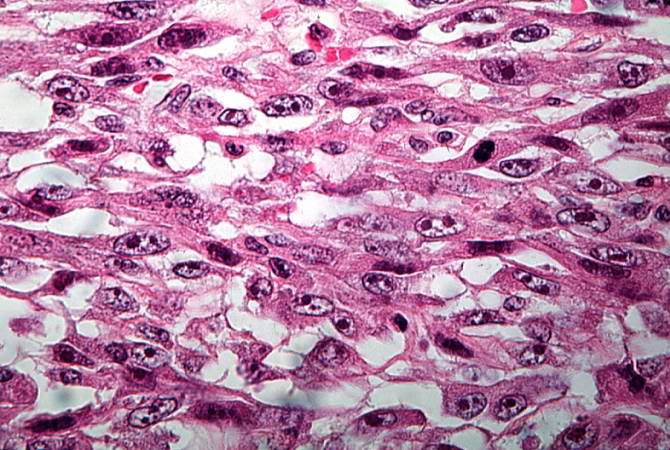
This high-power photomicrograph of the tumor demonstrates the fusiform morphology of the cells. Note the marked variability in size and staining intensity of the nuclei.
-
This is a high-power photomicrograph of the tumor demonstrating the anaplastic cell morphology.
-
This is a high-power photomicrograph of the tumor demonstrating the anaplastic cell morphology.
-
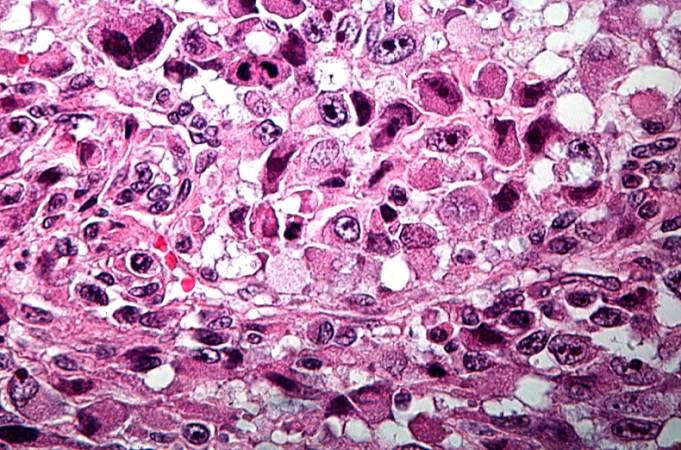
This is a high-power photomicrograph of the tumor demonstrating the anaplastic cell morphology and multiple mitotic figures (arrows).







References
- ↑ 1.0 1.1 Image courtesy of Dr Frank Gaillard. Radiopaedia (original file [1]). [http://radiopaedia.org/licence Creative Commons BY-SA-NC
- ↑ 2.00 2.01 2.02 2.03 2.04 2.05 2.06 2.07 2.08 2.09 2.10 2.11 Osteosarcoma. Dr Yuranga Weerakkody◉ et al. Radiopaedia.org 2015. http://radiopaedia.org/articles/telangiectatic-osteosarcoma
- ↑ Wang LL. Biology of osteogenic sarcoma. Cancer J 11:294-305, 2005.