Vortioxetine
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Vignesh Ponnusamy, M.B.B.S. [2]
WikiDoc MAKES NO GUARANTEE OF VALIDITY. WikiDoc is not a professional health care provider, nor is it a suitable replacement for a licensed healthcare provider. WikiDoc is intended to be an educational tool, not a tool for any form of healthcare delivery. The educational content on WikiDoc drug pages is based upon the FDA package insert, National Library of Medicine content and practice guidelines / consensus statements. WikiDoc does not promote the administration of any medication or device that is not consistent with its labeling. Please read our full disclaimer here.
Black Box Warning
|
WARNING
See full prescribing information for complete Boxed Warning.
SUICIDAL THOUGHTS AND BEHAVIORS
|
Overview
Vortioxetine is an antidepressant that is FDA approved for the {{{indicationType}}} of major depressive disorder. There is a Black Box Warning for this drug as shown here. Common adverse reactions include nausea, constipation and vomiting.
Adult Indications and Dosage
FDA-Labeled Indications and Dosage (Adult)
Major Depressive Disorder
- The recommended starting dose is 10 mg administered orally once daily without regard to meals. Dosage should then be increased to 20 mg/day, as tolerated, because higher doses demonstrated better treatment effects in trials conducted in the United States. The efficacy and safety of doses above 20 mg/day have not been evaluated in controlled clinical trials. A dose decrease down to 5 mg/day may be considered for patients who do not tolerate higher doses.
- Maintenance/Continuation/Extended Treatment
- It is generally agreed that acute episodes of major depression should be followed by several months or longer of sustained pharmacologic therapy. A maintenance study of BRINTELLIX demonstrated that BRINTELLIX decreased the risk of recurrence of depressive episodes compared to placebo.
- Discontinuing Treatment
- Although BRINTELLIX can be abruptly discontinued, in placebo-controlled trials patients experienced transient adverse reactions such as headache and muscle tension following abrupt discontinuation of BRINTELLIX 15 mg/day or 20 mg/day. To avoid these adverse reactions, it is recommended that the dose be decreased to 10 mg/day for one week before full discontinuation of BRINTELLIX 15 mg/day or 20 mg/day.
- Switching a Patient To or From a Monoamine Oxidase Inhibitor (MAOI) Intended to Treat Psychiatric Disorders
- At least 14 days should elapse between discontinuation of a MAOI intended to treat psychiatric disorders and initiation of therapy with BRINTELLIX to avoid the risk of Serotonin Syndrome. Conversely, at least 21 days should be allowed after stopping BRINTELLIX before starting an MAOI intended to treat psychiatric disorders.
Off-Label Use and Dosage (Adult)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Vortioxetine in adult patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Vortioxetine in adult patients.
Pediatric Indications and Dosage
FDA-Labeled Indications and Dosage (Pediatric)
There is limited information regarding FDA-Labeled Use of Vortioxetine in pediatric patients.
Off-Label Use and Dosage (Pediatric)
Guideline-Supported Use
There is limited information regarding Off-Label Guideline-Supported Use of Vortioxetine in pediatric patients.
Non–Guideline-Supported Use
There is limited information regarding Off-Label Non–Guideline-Supported Use of Vortioxetine in pediatric patients.
Contraindications
- Hypersensitivity to vortioxetine or any components of the formulation. Angioedema has been reported in patients treated with BRINTELLIX.
- The use of MAOIs intended to treat psychiatric disorders with BRINTELLIX or within 21 days of stopping treatment with BRINTELLIX is contraindicated because of an increased risk of serotonin syndrome. The use of BRINTELLIX within 14 days of stopping an MAOI intended to treat psychiatric disorders is also contraindicated.
- Starting BRINTELLIX in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue is also contraindicated because of an increased risk of serotonin syndrome.
Warnings
|
WARNING
See full prescribing information for complete Boxed Warning.
SUICIDAL THOUGHTS AND BEHAVIORS
|
Precautions
- Clinical Worsening and Suicide Risk
- Patients with major depressive disorder (MDD), both adult and pediatric, may experience worsening of their depression and/or the emergence of suicidal ideation and behavior (suicidality) or unusual changes in behavior, whether or not they are taking antidepressant medications, and this risk may persist until significant remission occurs. Suicide is a known risk of depression and certain other psychiatric disorders, and these disorders themselves are the strongest predictors of suicide. There has been a long-standing concern, however, that antidepressants may have a role in inducing worsening of depression and the emergence of suicidality in certain patients during the early phases of treatment. Pooled analyses of short-term placebo-controlled studies of antidepressant drugs (selective serotonin reuptake inhibitors [SSRIs] and others) showed that these drugs increase the risk of suicidal thinking and behavior (suicidality) in children, adolescents, and young adults (ages 18 to 24) with MDD and other psychiatric disorders. Short-term studies did not show an increase in the risk of suicidality with antidepressants compared to placebo in adults beyond age 24; there was a trend toward reduction with antidepressants compared to placebo in adults aged 65 and older.
- The pooled analyses of placebo-controlled studies in children and adolescents with MDD, obsessive-compulsive disorder (OCD), or other psychiatric disorders included a total of 24 short-term studies of nine antidepressant drugs in over 4,400 patients. The pooled analyses of placebo-controlled studies in adults with MDD or other psychiatric disorders included a total of 295 short-term studies (median duration of two months) of 11 antidepressant drugs in over 77,000 patients. There was considerable variation in risk of suicidality among drugs, but a tendency toward an increase in the younger patients for almost all drugs studied. There were differences in absolute risk of suicidality across the different indications, with the highest incidence in MDD. The risk differences (drug vs. placebo), however, were relatively stable within age strata and across indications. These risk differences (drug-placebo difference in the number of cases of suicidality per 1000 patients treated) are provided in Table 1.

This image is provided by the National Library of Medicine.

- No suicides occurred in any of the pediatric studies. There were suicides in the adult studies, but the number was not sufficient to reach any conclusion about drug effect on suicide.
- It is unknown whether the suicidality risk extends to longer-term use, i.e., beyond several months. However, there is substantial evidence from placebo-controlled maintenance studies in adults with depression that the use of antidepressants can delay the recurrence of depression.
- All patients being treated with antidepressants for any indication should be monitored appropriately and observed closely for clinical worsening, suicidality, and unusual changes in behavior, especially during the initial few months of a course of drug therapy, or at times of dose changes, either increases or decreases.
- The following symptoms anxiety, agitation, panic attacks, insomnia, irritability, hostility, aggressiveness, impulsivity, akathisia (psychomotor restlessness), hypomania, and mania have been reported in adult and pediatric patients being treated with antidepressants for MDD as well as for other indications, both psychiatric and nonpsychiatric. Although a causal link between the emergence of such symptoms and either the worsening of depression and/or the emergence of suicidal impulses has not been established, there is concern that such symptoms may represent precursors to emerging suicidality.
- Consideration should be given to changing the therapeutic regimen, including possibly discontinuing the medication, in patients whose depression is persistently worse, or who are experiencing emergent suicidality or symptoms that might be precursors to worsening depression or suicidality, especially if these symptoms are severe, abrupt in onset, or were not part of the patient's presenting symptoms.
- Families and caregivers of patients being treated with antidepressants for MDD or other indications, both psychiatric and nonpsychiatric, should be alerted about the need to monitor patients for the emergence of agitation, irritability, unusual changes in behavior, and the other symptoms described above, as well as the emergence of suicidality, and to report such symptoms immediately to healthcare providers. Such monitoring should include daily observation by families and caregivers.
- Screening Patients for Bipolar Disorder
- A major depressive episode may be the initial presentation of bipolar disorder. It is generally believed (though not established in controlled studies) that treating such an episode with an antidepressant alone may increase the likelihood of precipitation of a mixed/manic episode in patients at risk for bipolar disorder. Whether any of the symptoms described above represent such a conversion is unknown. However, prior to initiating treatment with an antidepressant, patients with depressive symptoms should be adequately screened to determine if they are at risk for bipolar disorder; such screening should include a detailed psychiatric history, including a family history of suicide, bipolar disorder, and depression. It should be noted that BRINTELLIX is not approved for use in treating bipolar depression.
- Serotonin Syndrome
- The development of a potentially life-threatening serotonin syndrome has been reported with serotonergic antidepressants including BRINTELLIX, when used alone but more often when used concomitantly with other serotonergic drugs (including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, tryptophan, buspirone, and St. John’s Wort), and with drugs that impair metabolism of serotonin (in particular, MAOIs, both those intended to treat psychiatric disorders and also others, such as linezolid and intravenous methylene blue).
- Serotonin syndrome symptoms may include mental status changes (e.g., agitation, hallucinations, delirium, and coma), autonomic instability (e.g., tachycardia, labile blood pressure, dizziness, diaphoresis, flushing, hyperthermia), neuromuscular symptoms (e.g., tremor, rigidity, myoclonus, hyperreflexia, incoordination), seizures, and/or gastrointestinal symptoms (e.g., nausea, vomiting, diarrhea). Patients should be monitored for the emergence of serotonin syndrome.
- The concomitant use of BRINTELLIX with MAOIs intended to treat psychiatric disorders is contraindicated. BRINTELLIX should also not be started in a patient who is being treated with MAOIs such as linezolid or intravenous methylene blue. All reports with methylene blue that provided information on the route of administration involved intravenous administration in the dose range of 1 mg/kg to 8 mg/kg. No reports involved the administration of methylene blue by other routes (such as oral tablets or local tissue injection) or at lower doses. There may be circumstances when it is necessary to initiate treatment with a MAOI such as linezolid or intravenous methylene blue in a patient taking BRINTELLIX. BRINTELLIX should be discontinued before initiating treatment with the MAOI.
- If concomitant use of BRINTELLIX with other serotonergic drugs, including triptans, tricyclic antidepressants, fentanyl, lithium, tramadol, buspirone, tryptophan, and St. John’s Wort is clinically warranted, patients should be made aware of a potential increased risk for serotonin syndrome, particularly during treatment initiation and dose increases.
- Treatment with BRINTELLIX and any concomitant serotonergic agents should be discontinued immediately if the above events occur and supportive symptomatic treatment should be initiated.
- Abnormal Bleeding
- The use of drugs that interfere with serotonin reuptake inhibition, including BRINTELLIX, may increase the risk of bleeding events. Concomitant use of aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), warfarin, and other anticoagulants may add to this risk. Case reports and epidemiological studies (case-control and cohort design) have demonstrated an association between use of drugs that interfere with serotonin reuptake and the occurrence of gastrointestinal bleeding. Bleeding events related to drugs that inhibit serotonin reuptake have ranged from ecchymosis, hematoma, epistaxis, and petechiae to life-threatening hemorrhages.
- Patients should be cautioned about the increased risk of bleeding when BRINTELLIX is coadministered with NSAIDs, aspirin, or other drugs that affect coagulation or bleeding.
- Activation of Mania/Hypomania
- Symptoms of mania/hypomania were reported in <0.1% of patients treated with BRINTELLIX in pre-marketing clinical studies. Activation of mania/hypomania has been reported in a small proportion of patients with major affective disorder who were treated with other antidepressants. As with all antidepressants, use BRINTELLIX cautiously in patients with a history or family history of bipolar disorder, mania, or hypomania.
- Angle Closure Glaucoma
- Angle Closure Glaucoma: The pupillary dilation that occurs following use of many antidepressant drugs, including BRINTELLIX, may trigger an angle closure attack in a patient with anatomically narrow angles who does not have a patent iridectomy.
- Hyponatremia
- Hyponatremia has occurred as a result of treatment with serotonergic drugs. In many cases, hyponatremia appears to be the result of the syndrome of inappropriate antidiuretic hormone secretion (SIADH). One case with serum sodium lower than 110 mmol/L was reported in a subject treated with BRINTELLIX in a pre-marketing clinical study. Elderly patients may be at greater risk of developing hyponatremia with a serotonergic antidepressant. Also, patients taking diuretics or who are otherwise volume-depleted can be at greater risk. Discontinuation of BRINTELLIX in patients with symptomatic hyponatremia and appropriate medical intervention should be instituted. Signs and symptoms of hyponatremia include headache, difficulty concentrating, memory impairment, confusion, weakness, and unsteadiness, which can lead to falls. More severe and/or acute cases have included hallucination, syncope, seizure, coma, respiratory arrest, and death.
Adverse Reactions
Clinical Trials Experience
- Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical studies of another drug and may not reflect the rates observed in clinical practice.
- Patient Exposure
- BRINTELLIX was evaluated for safety in 4746 patients (18 years to 88 years of age) diagnosed with MDD who participated in pre-marketing clinical studies; 2616 of those patients were exposed to BRINTELLIX in 6 to 8 week, placebo-controlled studies at doses ranging from 5 mg to 20 mg once daily and 204 patients were exposed to BRINTELLIX in a 24 week to 64 week placebo-controlled maintenance study at doses of 5 mg to 10 mg once daily. Patients from the 6 to 8 week studies continued into 12‑month open-label studies. A total of 2586 patients were exposed to at least one dose of BRINTELLIX in open-label studies, 1727 were exposed to BRINTELLIX for six months and 885 were exposed for at least one year.
- Adverse Reactions Reported as Reasons for Discontinuation of Treatment
- In pooled 6 to 8 week placebo-controlled studies the incidence of patients who received BRINTELLIX 5 mg/day, 10 mg/day, 15 mg/day and 20 mg/day and discontinued treatment because of an adverse reaction was 5%, 6%, 8% and 8%, respectively, compared to 4% of placebo-treated patients. Nausea was the most common adverse reaction reported as a reason for discontinuation.
- Common Adverse Reactions in Placebo-Controlled MDD Studies
- The most commonly observed adverse reactions in MDD patients treated with BRINTELLIX in 6 to 8 week placebo-controlled studies (incidence ≥5% and at least twice the rate of placebo) were nausea, constipation and vomiting.
- Table 2 shows the incidence of common adverse reactions that occurred in ≥2% of MDD patients treated with any BRINTELLIX dose and at least 2% more frequently than in placebo-treated patients in the 6 to 8 week placebo-controlled studies.

This image is provided by the National Library of Medicine.

- Nausea
- Nausea was the most common adverse reaction and its frequency was dose-related (Table 2). It was usually considered mild or moderate in intensity and the median duration was 2 weeks. Nausea was more common in females than males. Nausea most commonly occurred in the first week of BRINTELLIX treatment with 15 to 20% of patients experiencing nausea after 1 to 2 days of treatment. Approximately 10% of patients taking BRINTELLIX 10 mg/day to 20 mg/day had nausea at the end of the 6 to 8 week placebo-controlled studies.
- Sexual Dysfunction
- Difficulties in sexual desire, sexual performance and sexual satisfaction often occur as manifestations of psychiatric disorders, but they may also be consequences of pharmacologic treatment.
- In the MDD 6 to 8 week controlled trials of BRINTELLIX, voluntarily reported adverse reactions related to sexual dysfunction were captured as individual event terms. These event terms have been aggregated and the overall incidence was as follows. In male patients the overall incidence was 3%, 4%, 4%, 5% in BRINTELLIX 5 mg/day, 10 mg/day, 15 mg/day, 20 mg/day, respectively, compared to 2% in placebo. In female patients, the overall incidence was <1%, 1%, <1%, 2% in BRINTELLIX 5 mg/day, 10 mg/day, 15 mg/day, 20 mg/day, respectively, compared to <1% in placebo.
- Because voluntarily reported adverse sexual reactions are known to be underreported, in part because patients and physicians may be reluctant to discuss them, the Arizona Sexual Experiences Scale (ASEX), a validated measure designed to identify sexual side effects, was used prospectively in seven placebo-controlled trials. The ASEX scale includes five questions that pertain to the following aspects of sexual function: 1) sex drive, 2) ease of arousal, 3) ability to achieve erection (men) or lubrication (women), 4) ease of reaching orgasm, and 5) orgasm satisfaction.
- The presence or absence of sexual dysfunction among patients entering clinical studies was based on their ASEX scores. For patients without sexual dysfunction at baseline (approximately 1/3 of the population across all treatment groups in each study), Table 3 shows the incidence of patients that developed treatment-emergent sexual dysfunction when treated with BRINTELLIX or placebo in any fixed dose group. Physicians should routinely inquire about possible sexual side effects.
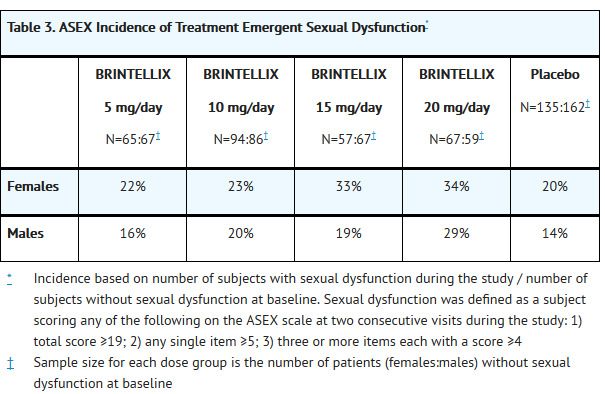
This image is provided by the National Library of Medicine.

- Adverse Reactions Following Abrupt Discontinuation of BRINTELLIX Treatment
- Discontinuation symptoms have been prospectively evaluated in patients taking BRINTELLIX 10 mg/day, 15 mg/day, and 20 mg/day using the Discontinuation-Emergent Signs and Symptoms (DESS) scale in clinical trials. Some patients experienced discontinuation symptoms such as headache, muscle tension, mood swings, sudden outbursts of anger, dizziness, and runny nose in the first week of abrupt discontinuation of BRINTELLIX 15 mg/day and 20 mg/day.
- Laboratory Tests
- BRINTELLIX has not been associated with any clinically important changes in laboratory test parameters in serum chemistry (except sodium), hematology and urinalysis as measured in the 6 to 8 week placebo-controlled studies. Hyponatremia has been reported with the treatment of BRINTELLIX. In the 6-month, double-blind, placebo-controlled phase of a long-term study in patients who had responded to BRINTELLIX during the initial 12-week, open-label phase, there were no clinically important changes in lab test parameters between BRINTELLIX and placebo-treated patients.
- Weight
- BRINTELLIX had no significant effect on body weight as measured by the mean change from baseline in the 6 to 8 week placebo-controlled studies. In the 6-month, double-blind, placebo-controlled phase of a long-term study in patients who had responded to BRINTELLIX during the initial 12-week, open-label phase, there was no significant effect on body weight between BRINTELLIX and placebo-treated patients.
- Vital Signs
- BRINTELLIX has not been associated with any clinically significant effects on vital signs, including systolic and diastolic blood pressure and heart rate, as measured in placebo-controlled studies.
- Other Adverse Reactions Observed in Clinical Studies
- The following listing does not include reactions: 1) already listed in previous tables or elsewhere in labeling, 2) for which a drug cause was remote, 3) which were so general as to be uninformative, 4) which were not considered to have significant clinical implications, or 5) which occurred at a rate equal to or less than placebo.
Ear and labyrinth disorders
Gastrointestinal disorders
Nervous system disorders
Vascular disorders
Postmarketing Experience
There is limited information regarding Postmarketing Experience of Vortioxetine in the drug label.
Drug Interactions
- Monoamine Oxidase Inhibitors
- Adverse reactions, some of which are serious or fatal, can develop in patients who use MAOIs or who have recently been discontinued from an MAOI and started on a serotonergic antidepressant(s) or who have recently had SSRI or SNRI therapy discontinued prior to initiation of an MAOI.
- Serotonergic Drugs
- Based on the mechanism of action of BRINTELLIX and the potential for serotonin toxicity, serotonin syndrome may occur when BRINTELLIX is coadministered with other drugs that may affect the serotonergic neurotransmitter systems (e.g., SSRIs, SNRIs, triptans, buspirone, tramadol, and tryptophan products etc.). Closely monitor symptoms of serotonin syndrome if BRINTELLIX is co-administered with other serotonergic drugs. Treatment with BRINTELLIX and any concomitant serotonergic agents should be discontinued immediately if serotonin syndrome occurs.
- Other CNS Active Agents
- No clinically relevant effect was observed on steady state lithium exposure following coadministration with multiple daily doses of BRINTELLIX. Multiple doses of BRINTELLIX did not affect the pharmacokinetics or pharmacodynamics (composite cognitive score) of diazepam. A clinical study has shown that BRINTELLIX (single dose of 20 or 40 mg) did not increase the impairment of mental and motor skills caused by alcohol (single dose of 0.6 g/kg). Details on the potential pharmacokinetic interactions between BRINTELLIX and bupropion can be found in Section 7.3.
- Drugs that Interfere with Hemostasis (e.g., NSAIDs, Aspirin, and Warfarin)
- Serotonin release by platelets plays an important role in hemostasis. Epidemiological studies of case-control and cohort design have demonstrated an association between use of psychotropic drugs that interfere with serotonin reuptake and the occurrence of upper gastrointestinal bleeding. These studies have also shown that concurrent use of an NSAID or aspirin may potentiate this risk of bleeding. Altered anticoagulant effects, including increased bleeding, have been reported when SSRIs and SNRIs are coadministered with warfarin.
- Following coadministration of stable doses of warfarin (1 to 10 mg/day) with multiple daily doses of BRINTELLIX, no significant effects were observed in INR, prothrombin values or total warfarin (protein bound plus free drug) pharmacokinetics for both R- and S-warfarin. Coadministration of aspirin 150 mg/day with multiple daily doses of BRINTELLIX had no significant inhibitory effect on platelet aggregation or pharmacokinetics of aspirin and salicylic acid. Patients receiving other drugs that interfere with hemostasis should be carefully monitored when BRINTELLIX is initiated or discontinued.
- Potential for Other Drugs to Affect BRINTELLIX
- Reduce BRINTELLIX dose by half when a strong CYP2D6 inhibitor (e.g., bupropion, fluoxetine, paroxetine, quinidine) is coadministered. Consider increasing the BRINTELLIX dose when a strong CYP inducer (e.g., rifampicin, carbamazepine, phenytoin) is coadministered. The maximum dose is not recommended to exceed three times the original dose (Figure 1).

This image is provided by the National Library of Medicine.

- Potential for BRINTELLIX to Affect Other Drugs
- No dose adjustment for the comedications is needed when BRINTELLIX is coadministered with a substrate of CYP1A2 (e.g., duloxetine), CYP2A6, CYP2B6 (e.g., bupropion), CYP2C8 (e.g., repaglinide), CYP2C9 (e.g., S-warfarin), CYP2C19 (e.g., diazepam), CYP2D6 (e.g., venlafaxine), CYP3A4/5 (e.g., budesonide), and P-gp (e.g., digoxin). In addition, no dose adjustment for lithium, aspirin, and warfarin is necessary.
- Vortioxetine and its metabolites are unlikely to inhibit the following CYP enzymes and transporter based on in vitro data: CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, CYP2D6, CYP2E1, CYP3A4/5, and P-gp. As such, no clinically relevant interactions with drugs metabolized by these CYP enzymes would be expected.
- In addition, vortioxetine did not induce CYP1A2, CYP2A6, CYP2B6, CYP2C8, CYP2C9, CYP2C19, and CYP3A4/5 in an in vitro study in cultured human hepatocytes. Chronic administration of BRINTELLIX is unlikely to induce the metabolism of drugs metabolized by these CYP isoforms. Furthermore, in a series of clinical drug interaction studies, coadministration of BRINTELLIX with substrates for CYP2B6 (e.g., bupropion), CYP2C9 (e.g., warfarin), and CYP2C19 (e.g., diazepam), had no clinical meaningful effect on the pharmacokinetics of these substrates (Figure 2).
- Because vortioxetine is highly bound to plasma protein, coadministration of BRINTELLIX with another drug that is highly protein bound may increase free concentrations of the other drug. However, in a clinical study with coadministration of BRINTELLIX (10 mg/day) and warfarin (1 mg/day to 10 mg/day), a highly protein-bound drug, no significant change in INR was observed.

This image is provided by the National Library of Medicine.

Use in Specific Populations
Pregnancy
- Pregnancy Category C
- Risk Summary
- There are no adequate and well-controlled studies of BRINTELLIX in pregnant women. Vortioxetine caused developmental delays when administered during pregnancy to rats and rabbits at doses 15 and 10 times the maximum recommended human dose (MRHD) of 20 mg, respectively. Developmental delays were also seen after birth in rats at doses 20 times the MRHD of vortioxetine given during pregnancy and through lactation. There were no teratogenic effects in rats or rabbits at doses up to 77 and 58 times, the MRHD of vortioxetine, respectively, given during organogenesis. The incidence of malformations in human pregnancies has not been established for BRINTELLIX. All human pregnancies, regardless of drug exposure, have a background rate of 2 to 4% for major malformations, and 15 to 20% for pregnancy loss. BRINTELLIX should be used during pregnancy only if the potential benefit justifies the potential risk to the fetus.
- Clinical Considerations
- Neonates exposed to SSRIs or SNRIs, late in the third trimester have developed complications requiring prolonged hospitalization, respiratory support and tube feeding. Such complications can arise immediately upon delivery. Reported clinical findings have included respiratory distress, cyanosis, apnea, seizures, temperature instability, feeding difficulty, vomiting, hypoglycemia, hypotonia, hypertonia, hyperreflexia, tremor, jitteriness, irritability and constant crying. These features are consistent with either a direct toxic effect of these classes of drugs or possibly, a drug discontinuation syndrome. It should be noted that in some cases, the clinical picture is consistent with serotonin syndrome. When treating a pregnant woman with BRINTELLIX during the third trimester, the physician should carefully consider the potential risks and benefits of treatment.
- Neonates exposed to SSRIs in pregnancy may have an increased risk for persistent pulmonary hypertension of the newborn (PPHN). PPHN occurs in one to two per 1,000 live births in the general population and is associated with substantial neonatal morbidity and mortality. Several recent epidemiologic studies suggest a positive statistical association between SSRI use in pregnancy and PPHN. Other studies do not show a significant statistical association.
- A prospective longitudinal study was conducted of 201 pregnant women with a history of major depression, who were either on antidepressants or had received antidepressants less than 12 weeks prior to their last menstrual period, and were in remission. Women who discontinued antidepressant medication during pregnancy showed a significant increase in relapse of their major depression compared to those women who remained on antidepressant medication throughout pregnancy. When treating a pregnant woman with BRINTELLIX, the physician should carefully consider both the potential risks of taking a serotonergic antidepressant, along with the established benefits of treating depression with an antidepressant.
- Animal Data
- In pregnant rats and rabbits, no teratogenic effects were seen when vortioxetine was given during the period of organogenesis at oral doses up to 160 and 60 mg/kg/day, respectively. These doses are 77 and 58 times, in rats and rabbits, respectively, the maximum recommended human dose (MRHD) of 20 mg on a mg/m2 basis. Developmental delay, seen as decreased fetal body weight and delayed ossification, occurred in rats and rabbits at doses equal to and greater than 30 and 10 mg/kg (15 and 10 times the MRHD, respectively) in the presence of maternal toxicity (decreased food consumption and decreased body weight gain). When vortioxetine was administered to pregnant rats at oral doses up to 120 mg/kg (58 times the MRHD) throughout pregnancy and lactation, the number of live-born pups was decreased and early postnatal pup mortality was increased at 40 and 120 mg/kg. Additionally, pup weights were decreased at birth to weaning at 120 mg/kg and development (specifically eye opening) was slightly delayed at 40 and 120 mg/kg. These effects were not seen at 10 mg/kg (5 times the MRHD).
- Australian Drug Evaluation Committee (ADEC) Pregnancy Category
There is no Australian Drug Evaluation Committee (ADEC) guidance on usage of Vortioxetine in women who are pregnant.
Labor and Delivery
There is no FDA guidance on use of Vortioxetine during labor and delivery.
Nursing Mothers
- It is not known whether vortioxetine is present in human milk. Vortioxetine is present in the milk of lactating rats. Because many drugs are present in human milk and because of the potential for serious adverse reactions in nursing infants from BRINTELLIX, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother.
Pediatric Use
- Clinical studies on the use of BRINTELLIX in pediatric patients have not been conducted; therefore, the safety and effectiveness of BRINTELLIX in the pediatric population have not been established.
Geriatic Use
- No dose adjustment is recommended on the basis of age (Figure 3). Results from a single-dose pharmacokinetic study in elderly (>65 years old) vs. young (24 to 45 years old) subjects demonstrated that the pharmacokinetics were generally similar between the two age groups.
- Of the 2616 subjects in clinical studies of BRINTELLIX, 11% (286) were 65 and over, which included subjects from a placebo-controlled study specifically in elderly patients. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identified differences in responses between the elderly and younger patients.
- Serotonergic antidepressants have been associated with cases of clinically significant hyponatremia in elderly patients, who may be at greater risk for this adverse event.
Gender
There is no FDA guidance on the use of Vortioxetine with respect to specific gender populations.
Race
There is no FDA guidance on the use of Vortioxetine with respect to specific racial populations.
Renal Impairment
There is no FDA guidance on the use of Vortioxetine in patients with renal impairment.
Hepatic Impairment
There is no FDA guidance on the use of Vortioxetine in patients with hepatic impairment.
Females of Reproductive Potential and Males
There is no FDA guidance on the use of Vortioxetine in women of reproductive potentials and males.
Immunocompromised Patients
There is no FDA guidance one the use of Vortioxetine in patients who are immunocompromised.
Administration and Monitoring
Administration
- Oral
Monitoring
There is limited information regarding Monitoring of Vortioxetine in the drug label.
IV Compatibility
There is limited information regarding IV Compatibility of Vortioxetine in the drug label.
Overdosage
Acute Overdose
Signs and Symptoms
- There is limited clinical trial experience regarding human overdosage with BRINTELLIX. In pre-marketing clinical studies, cases of overdose were limited to patients who accidentally or intentionally consumed up to a maximum dose of 40 mg of BRINTELLIX. The maximum single dose tested was 75 mg in men. Ingestion of BRINTELLIX in the dose range of 40 to 75 mg was associated with increased rates of nausea, dizziness, diarrhea, abdominal discomfort, generalized pruritus, somnolence, and flushing.
Management
- No specific antidotes for BRINTELLIX are known. In managing over dosage, consider the possibility of multiple drug involvement. In case of overdose, call Poison Control Center at 1-800-222-1222 for latest recommendations.
Chronic Overdose
There is limited information regarding Chronic Overdose of Vortioxetine in the drug label.
Pharmacology


Mechanism of Action
- The mechanism of the antidepressant effect of vortioxetine is not fully understood, but is thought to be related to its enhancement of serotonergic activity in the CNS through inhibition of the reuptake of serotonin (5-HT). It also has several other activities including 5-HT3 receptor antagonism and 5-HT1A receptor agonism. The contribution of these activities to vortioxetine’s antidepressant effect has not been established.
Structure
- BRINTELLIX is an immediate-release tablet for oral administration that contains the beta (β) polymorph of vortioxetine hydrobromide (HBr), an antidepressant. Vortioxetine HBr is known chemically as 1-[2-(2,4-Dimethyl-phenylsulfanyl)-phenyl]-piperazine, hydrobromide. The empirical formula is C18 H22 N2 S, HBr with a molecular weight of 379.36 g/mol. The structural formula is:

This image is provided by the National Library of Medicine.

- Vortioxetine HBr is a white to very slightly beige powder that is slightly soluble in water.
- Each BRINTELLIX tablet contains 6.355 mg, 12.71 mg, 19.065 mg, or 25.42 mg of vortioxetine HBr equivalent to 5 mg, 10 mg, 15 mg, or 20 mg of vortioxetine, respectively. The inactive ingredients in BRINTELLIX tablets include mannitol, microcrystalline cellulose, hydroxypropyl cellulose, sodium starch glycolate, magnesium stearate and film coating which consists of hypromellose, titanium dioxide, polyethylene glycol 400, iron oxide red (5 mg, 15 mg, and 20 mg) and iron oxide yellow (10 mg and 15 mg).
Pharmacodynamics
- Vortioxetine binds with high affinity to the human serotonin transporter (Ki=1.6 nM), but not to the norepinephrine (Ki=113 nM) or dopamine (Ki>1000 nM) transporters. Vortioxetine potently and selectively inhibits reuptake of serotonin (IC50=5.4 nM). Vortioxetine binds to 5-HT3 (Ki=3.7 nM), 5-HT1A (Ki=15 nM), 5-HT7 (Ki=19 nM), 5-HT1D (Ki=54 nM), and 5-HT1B (Ki=33 nM), receptors and is a 5-HT3, 5-HT1D, and 5-HT7 receptor antagonist, 5-HT1B receptor partial agonist, and 5-HT1A receptor agonist.
- In humans, the mean 5-HT transporter occupancy, based on the results from 2 clinical PET studies using 5-HTT ligands ([11C]-MADAM or [11C]-DASB), was approximately 50% at 5 mg/day, 65% at 10 mg/day and approximately 80% at 20 mg/day in the regions of interest.
- Effect on Cardiac Repolarization
- The effect of vortioxetine 10 mg and 40 mg administered once daily on QTc interval was evaluated in a randomized, double-blind, placebo-, and active-controlled (moxifloxacin 400 mg), four-treatment-arm parallel study in 340 male subjects. In the study the upper bound of the one-sided 95% confidence interval for the QTc was below 10 ms, the threshold for regulatory concern. The oral dose of 40 mg is sufficient to assess the effect of metabolic inhibition.
- Effect on Driving Performance
- In a clinical study in healthy subjects, BRINTELLIX did not impair driving performance, or have adverse psychomotor or cognitive effects following single and multiple doses of 10 mg/day. Because any psychoactive drug may impair judgment, thinking, or motor skills, however, patients should be cautioned about operating hazardous machinery, including automobiles, until they are reasonably certain that BRINTELLIX therapy does not affect their ability to engage in such activities.
Pharmacokinetics
- Vortioxetine pharmacological activity is due to the parent drug. The pharmacokinetics of vortioxetine (2.5 mg to 60 mg) are linear and dose-proportional when vortioxetine is administered once daily. The mean terminal half-life is approximately 66 hours, and steady-state plasma concentrations are typically achieved within two weeks of dosing.
- Absorption
- The maximal plasma vortioxetine concentration (Cmax) after dosing is reached within 7 to 11 hours postdose (Tmax). Steady-state mean Cmax values were 9, 18, and 33 ng/mL following doses of 5, 10, and 20 mg/day. Absolute bioavailability is 75%. No effect of food on the pharmacokinetics was observed.
- Distribution
- The apparent volume of distribution of vortioxetine is approximately 2600 L, indicating extensive extravascular distribution. The plasma protein binding of vortioxetine in humans is 98%, independent of plasma concentrations. No apparent difference in the plasma protein binding between healthy subjects and subjects with hepatic (mild, moderate) or renal (mild, moderate, severe, ESRD) impairment is observed.
- Metabolism and Elimination
- Vortioxetine is extensively metabolized primarily through oxidation via cytochrome P450 isozymes CYP2D6, CYP3A4/5, CYP2C19, CYP2C9, CYP2A6, CYP2C8 and CYP2B6 and subsequent glucuronic acid conjugation. CYP2D6 is the primary enzyme catalyzing the metabolism of vortioxetine to its major, pharmacologically inactive, carboxylic acid metabolite, and poor metabolizers of CYP2D6 have approximately twice the vortioxetine plasma concentration of extensive metabolizers.
- Following a single oral dose of [14C]-labeled vortioxetine, approximately 59% and 26% of the administered radioactivity was recovered in the urine and feces, respectively as metabolites. Negligible amounts of unchanged vortioxetine were excreted in the urine up to 48 hours. The presence of hepatic (mild or moderate) or renal impairment (mild, moderate, severe and ESRD) did not affect the apparent clearance of vortioxetine.
Nonclinical Toxicology
- Carcinogenesis
- Carcinogenicity studies were conducted in which CD-1 mice and Wistar rats were given oral doses of vortioxetine up to 50 and 100 mg/kg/day for male and female mice, respectively, and 40 and 80 mg/kg/day for male and female rats, respectively, for 2 years. The doses in the two species were approximately 12, 24, 20, and 39 times, respectively, the maximum recommended human dose (MRHD) of 20 mg on a mg/m2 basis.
- In rats, the incidence of benign polypoid adenomas of the rectum was statistically significantly increased in females at doses 39 times the MRHD, but not at 15 times the MRHD. These were considered related to inflammation and hyperplasia and possibly caused by an interaction with a vehicle component of the formulation used for the study. The finding did not occur in male rats at 20 times the MRHD.
- In mice, vortioxetine was not carcinogenic in males or females at doses up to 12 and 24 times, respectively, the MRHD.
- Mutagenicity
- Vortioxetine was not genotoxic in the in vitro bacterial reverse mutation assay (Ames test), an in vitro chromosome aberration assay in cultured human lymphocytes, and an in vivo rat bone marrow micronucleus assay.
- Impairment of Fertility
- Treatment of rats with vortioxetine at doses up to 120 mg/kg/day had no effect on male or female fertility, which is 58 times the maximum recommended human dose (MRHD) of 20 mg on a mg/m2 basis.
Clinical Studies
- The efficacy of BRINTELLIX in treatment for MDD was established in six 6 to 8 week randomized, double-blind, placebo-controlled, fixed-dose studies (including one study in the elderly) and one maintenance study in adult inpatients and outpatients who met the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV-TR) criteria for MDD.
- Adults (aged 18 years to 75 years)
- The efficacy of BRINTELLIX in patients aged 18 years to 75 years was demonstrated in five 6 to 8 week, placebo-controlled studies (Studies 1 to 5 in Table 4). In these studies, patients were randomized to BRINTELLIX 5 mg, 10 mg, 15 mg or 20 mg or placebo once daily. For patients who were randomized to BRINTELLIX 15 mg/day or 20 mg/day, the final doses were titrated up from 10 mg/day after the first week.
- The primary efficacy measures were the Hamilton Depression Scale (HAMD-24) total score in Study 2 and the Montgomery-Asberg Depression Rating Scale (MADRS) total score in all other studies. In each of these studies, at least one dose group of BRINTELLIX was superior to placebo in improvement of depressive symptoms as measured by mean change from baseline to endpoint visit on the primary efficacy measurement (see Table 4). Subgroup analysis by age, gender or race did not suggest any clear evidence of differential responsiveness. Two studies of the 5 mg dose in the U.S. (not represented in Table 4) failed to show effectiveness.
- Elderly Study (aged 64 years to 88 years)
- The efficacy of BRINTELLIX for the treatment of MDD was also demonstrated in a randomized, double-blind, placebo-controlled, fixed-dose study of BRINTELLIX in elderly patients (aged 64 years to 88 years) with MDD (Study 6 in Table 4). Patients meeting the diagnostic criteria for recurrent MDD with at least one previous major depressive episode before the age of 60 years and without comorbid cognitive impairment (Mini Mental State Examination score <24) received BRINTELLIX 5 mg or placebo.

This image is provided by the National Library of Medicine.

- Time Course of Treatment Response
- In the 6 to 8 week placebo-controlled studies, an effect of BRINTELLIX based on the primary efficacy measure was generally observed starting at Week 2 and increased in subsequent weeks with the full antidepressant effect of BRINTELLIX generally not seen until Study Week 4 or later. Figure 4 depicts time course of response in U.S. based on the primary efficacy measure (MADRS) in Study 5.

This image is provided by the National Library of Medicine.


This image is provided by the National Library of Medicine.

- Maintenance Study
- In a non-US maintenance study (Study 7 in Figure 6), 639 patients meeting DSM-IV-TR criteria for MDD received flexible doses of BRINTELLIX (5 mg or 10 mg) once daily during an initial 12 week open-label treatment phase; the dose of BRINTELLIX was fixed during Weeks 8 to 12. Three hundred ninety six (396) patients who were in remission (MADRS total score ≤10 at both Weeks 10 and 12) after open-label treatment were randomly assigned to continuation of a fixed dose of BRINTELLIX at the final dose they responded to (about 75% of patients were on 10 mg/day) during the open-label phase or to placebo for 24 to 64 weeks. Approximately 61% of randomized patients satisfied remission criterion (MADRS total score ≤10) for at least 4 weeks (since Week 8), and 15% for at least 8 weeks (since Week 4). Patients on BRINTELLIX experienced a statistically significantly longer time to have recurrence of depressive episodes than did patients on placebo. Recurrence of depressive episode was defined as a MADRS total score ≥22 or lack of efficacy as judged by the investigator.

This image is provided by the National Library of Medicine.

How Supplied
- BRINTELLIX tablets are available as follows:

This image is provided by the National Library of Medicine.

- Storage: Store at 77°F (25°C); excursions permitted to 59°F to 86°F (15°C to 30°C).
Storage
There is limited information regarding Vortioxetine Storage in the drug label.
Images
Drug Images
{{#ask: Page Name::Vortioxetine |?Pill Name |?Drug Name |?Pill Ingred |?Pill Imprint |?Pill Dosage |?Pill Color |?Pill Shape |?Pill Size (mm) |?Pill Scoring |?NDC |?Drug Author |format=template |template=DrugPageImages |mainlabel=- |sort=Pill Name }}
Package and Label Display Panel
{{#ask: Label Page::Vortioxetine |?Label Name |format=template |template=DrugLabelImages |mainlabel=- |sort=Label Page }}
Patient Counseling Information
- Advise patients and their caregivers about the benefits and risks associated with treatment with BRINTELLIX and counsel them in its appropriate use. Advise patients and their caregivers to read the Medication Guide and assist them in understanding its contents. The complete text of the Medication Guide is reprinted at the end of this document.
- Suicide Risk
- Advise patients and caregivers to look for the emergence of suicidal ideation and behavior, especially early during treatment and when the dose is adjusted up or down.
- Discontinuation of Treatment
- Patients who are on BRINTELLIX 15 mg/day or 20 mg/day may experience headache, muscle tension, mood swings, sudden outburst of anger, dizziness and runny nose if they abruptly stop their medicine. Advise patients not stopping BRINTELLIX without talking to their healthcare provider.
- Concomitant Medication
- Advise patients to inform their physicians if they are taking, or plan to take, any prescription or over-the-counter medications because of a potential for interactions. Instruct patients not to take BRINTELLIX with an MAOI or within 14 days of stopping an MAOI and to allow 21 days after stopping BRINTELLIX before starting an MAOI.
- Serotonin Syndrome
- Caution patients about the risk of serotonin syndrome, particularly with the concomitant use of BRINTELLIX and triptans, tricyclic antidepressants, fentanyl, Lithium, tramadol, tryptophan supplements, and St. John’s Wort supplements.
- Abnormal Bleeding
- Caution patients about the increased risk of abnormal bleeding when BRINTELLIX is given with NSAIDs, aspirin, warfarin, or other drugs that affect coagulation.
- Activation of Mania/Hypomania
- Advise patients and their caregivers to look for signs of activation of mania/hypomania.
- Angle Closure Glaucoma
- Patients should be advised that taking BRINTELLIX can cause mild pupillary dilation, which in susceptible individuals, can lead to an episode of angle closure glaucoma. Pre-existing glaucoma is almost always open-angle glaucoma because angle closure glaucoma, when diagnosed, can be treated definitively with iridectomy. Open-angle glaucoma is not a risk factor for angle closure glaucoma. Patients may wish to be examined to determine whether they are susceptible to angle closure, and have a prophylactic procedure (e.g., iridectomy), if they are susceptible.
- Hyponatremia
- Advise patients that if they are treated with diuretics, or are otherwise volume depleted, or are elderly, they may be at greater risk of developing hyponatremia while taking BRINTELLIX.
- Nausea
- Advise patients that nausea is the most common adverse reaction, and is dose related. Nausea commonly occurs within the first week of treatment, then decreases in frequency but can persist in some patients.
- Alcohol
- A clinical study has shown that BRINTELLIX (single dose of 20 or 40 mg/day) did not increase the impairment of mental and motor skills caused by alcohol.
- Allergic Reactions
- Advise patients to notify their healthcare provider if they develop an allergic reaction such as rash, hives, swelling, or difficulty breathing.
- Pregnancy
- Advise patients to notify their healthcare provider if they become pregnant or intend to become pregnant during therapy with BRINTELLIX.
- Nursing Mothers
- Advise patients to notify their healthcare provider if they are breast-feeding an infant and would like to continue or start BRINTELLIX.

This image is provided by the National Library of Medicine.

Precautions with Alcohol
- Alcohol-Vortioxetine interaction has not been established. Talk to your doctor about the effects of taking alcohol with this medication.
Brand Names
- BRINTELLIX®[1]
Look-Alike Drug Names
There is limited information regarding Vortioxetine Look-Alike Drug Names in the drug label.
Price
References
The contents of this FDA label are provided by the National Library of Medicine.
{{#subobject:
|Page Name=Vortioxetine |Pill Name=No image.jpg |Drug Name= |Pill Ingred=|+sep=; |Pill Imprint= |Pill Dosage= |Pill Color=|+sep=; |Pill Shape= |Pill Size (mm)= |Pill Scoring= |Pill Image= |Drug Author= |NDC=
}}
{{#subobject:
|Label Page=Vortioxetine |Label Name=Vortioxetine07.png
}}
{{#subobject:
|Label Page=Vortioxetine |Label Name=Vortioxetine08.png
}}
{{#subobject:
|Label Page=Vortioxetine |Label Name=Vortioxetine09.png
}}
{{#subobject:
|Label Page=Vortioxetine |Label Name=Vortioxetine10.png
}}
{{#subobject:
|Label Page=Vortioxetine |Label Name=Vortioxetine11.png
}}