Umbilical vein
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
The umbilical vein is a blood vessel present during fetal development that carries oxygenated blood from the placenta to the growing fetus.
Circulation
Attached to the uterine lining, the placenta is the site of gas exchange between mother and fetus. The singular umbilical vein carries oxygenated blood from the placenta to the fetus, while two umbilical arteries return deoxygenated blood to the placenta. The three vessels coil around one another within the Wharton's jelly of the umbilical cord and enter the abdomen at the umbilicus.
Inside the fetus, the vein courses alongside the falciform ligament and then to the liver's underside. At the transverse fissure, the vein divides into two vessels, one larger than the other. The larger of the two is joined by the portal vein, and together they enter the right lobe of the liver. The smaller vessel, now called the ductus venosus, diverges away from the liver and joins with the inferior vena cava.
Closure
Within a week of birth, the infant's umbilical vein is completely obliterated and is replaced by a fibrous cord called the round ligament of the liver (also called the ligamentum teres hepatis, from the Latin meaning the same). It extends from the umbilicus to the transverse fissure, where it joins with the ligamentum venosum to separate the left and right lobes of the liver.
Closure of the umbilical vein usually occurs after the umbilical arteries have closed. This prolongs the communication between the placenta and fetal heart, allowing for a sort of autotransfusion of remaining blood from the placenta to the fetus.
Recanalization
Under extreme pressure, the round ligament may reopen to allow the passage of blood. Such recanalization is common in patients with cirrhosis and portal hypertension. Patients with cirrhosis experience rapid growth of scar tissue in and around the liver, often functionally obstructing nearby vessels. Vessel occlusion increases vascular resistance and therefore leads to hypertension. In portal hypertension, the vessels surrounding the liver are subjected to abnormally high blood pressure—so high, in fact, that the force of the blood pressing against the round ligament is sufficient to recanalize the structure.
Catheterization
A newborn baby has a patent umbilical vein for at least a few months. This umbilical vein may be catheterised for ready intravenous access. It may be used as a site for regular transfusion in cases of erythroblastosis or hemolytic disease.
Additional images
-
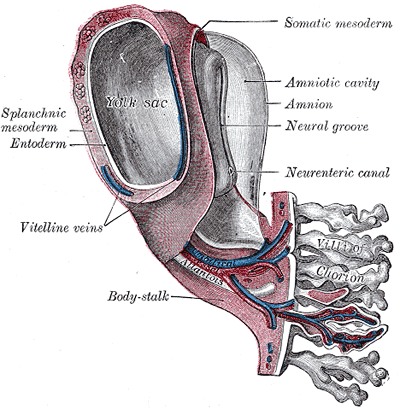 Model of human embryo 1.3 mm. long.
Model of human embryo 1.3 mm. long. -
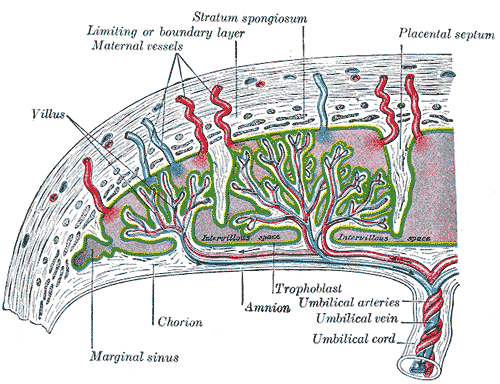 Scheme of placental circulation.
Scheme of placental circulation. -
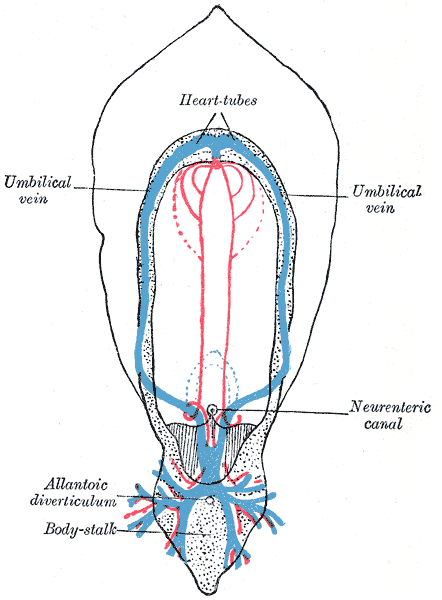 Diagram of the vascular channels in a human embryo of the second week.
Diagram of the vascular channels in a human embryo of the second week. -
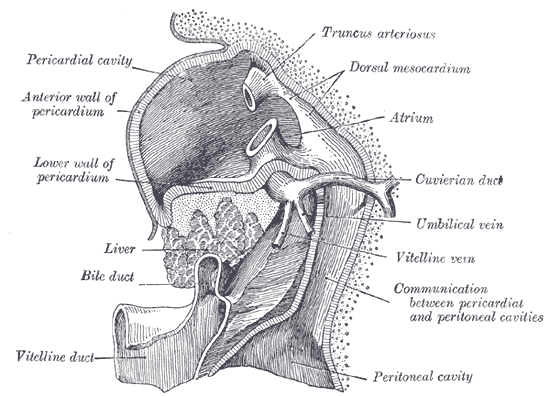
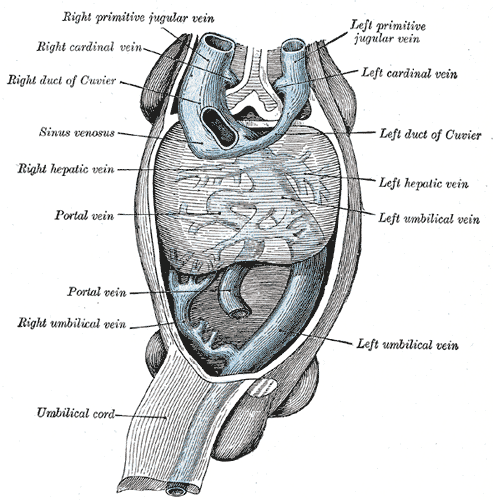 Human embryo with heart and anterior body-wall removed to show the sinus venosus and its tributaries.
Human embryo with heart and anterior body-wall removed to show the sinus venosus and its tributaries. -
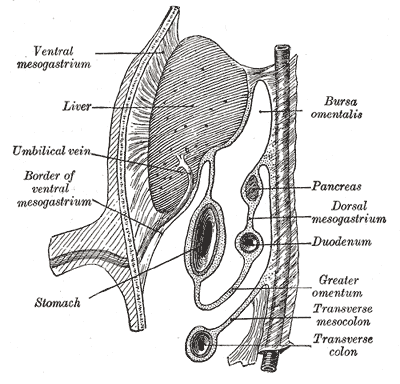 Schematic figure of the bursa omentalis, etc. Human embryo of eight weeks.
Schematic figure of the bursa omentalis, etc. Human embryo of eight weeks. -
 Liver with the septum transversum. Human embryo 3 mm. long.
Liver with the septum transversum. Human embryo 3 mm. long. -
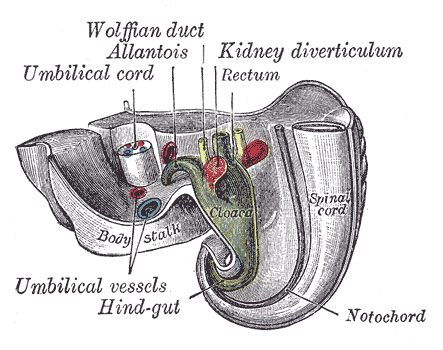 Tail end of human embryo twenty-five to twenty-nine days old.
Tail end of human embryo twenty-five to twenty-nine days old.







References
- Template:GraySubject - "Peculiarities in the vascular system of the fetus"
See also
Template:Veins Template:Embryology Template:Development of circulatory system