Ischemic stroke CT
|
Ischemic Stroke Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Ischemic stroke CT On the Web |
|
American Roentgen Ray Society Images of Ischemic stroke CT |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Aysha Anwar, M.B.B.S[2]
Overview
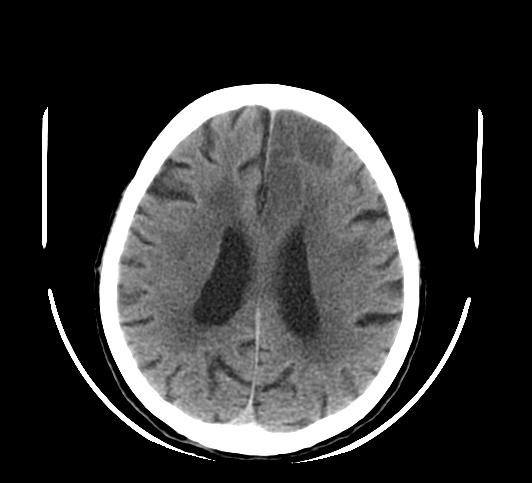
CT scan without contrast is the initial test performed to diagnose ischemic stroke and rule out hemorrhagic stroke. In the emergency setting, the sensitivity and specificity of CT scan without contrast is 16% and 96% respectively [1] The sensitivity and specificity for detection of early ischemia is enhanced with perfusion CT scan.
CT
CT scan without contrast is the initial test performed to diagnose ischemic stroke and rule out hemorrhagic stroke. In the emergency setting, the sensitivity and specificity of CT scan without contrast is 16% and 96% respectively [1] The sensitivity and specificity for detection of early ischemia is enhanced with perfusion CT scan. The main advantages of CT scan compared to MRI includes it being rapid, low cost, availability in acute setting, safe in patients with metallic implants such as pacemakers, implantable defibrillators. Some of the disadvantages which may limit its use include its decreased sensitivity and specificity to detect lacunar and posterior fossa infarcts. CT scan with contrast cannot be used in patients with renal failure.[2]
2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association[3]
Recommendations for Diagnostic Evaluation Referenced studies that support recommendations are summarized in online Data supplements 1 and 2
| Class I |
| 3. In patients with symptomatic anterior circulation cerebral infarction or TIA who are candidates for revascularization, noninvasive cervical carotid imaging with carotid ultrasonography, CT angiography (CTA), or magnetic resonance angiography (MRA) is recommended to screen for stenosis.(Level of Evidence: B-NR)
4. In patients suspected of having a stroke or TIA, CT or MRI of the brain is recommended to confirm the diagnosis of symptomatic ischemic cerebral vascular disease(Level of Evidence: B-NR) |
| Class IIa |
| 8. In patients suspected of having ischemic stroke, if CT or MRI does not demonstrate symptomatic cerebral infarct, follow-up CT or MRI of the brain is reasonable to confirm diagnosis.(Level of Evidence: B-NR)
11. In patients with ischemic stroke or TIA, noninvasive imaging of the intracranial large arteries and imaging of the extracranial vertebrobasilar arterial system with MRA or CTA can be effective to identify atherosclerotic disease, dissection, moyamoya, or other etiologically relevant vasculopathies(Level of Evidence: C-LD) |
| Class IIb |
| 12. In patients with ischemic stroke and a treatment plan that includes anticoagulant therapy, CT or MRI of the brain before therapy is started may be considered to assess for hemorrhagic transformation and final size of infarction.(Level of Evidence: B-NR) |
-
 CT
CT -
 CT
CT -
 CT
CT



References
- ↑ 1.0 1.1 Chalela, J (2007). "Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: a prospective comparison". Lancet. 369 (9558): 293–8. PMID 17258669. Retrieved 2008-01-22. Unknown parameter
|coauthors=ignored (help) - ↑ Wintermark M, Sanelli PC, Albers GW, Bello J, Derdeyn C, Hetts SW; et al. (2013). "Imaging recommendations for acute stroke and transient ischemic attack patients: A joint statement by the American Society of Neuroradiology, the American College of Radiology, and the Society of NeuroInterventional Surgery". AJNR Am J Neuroradiol. 34 (11): E117–27. doi:10.3174/ajnr.A3690. PMC 4072500. PMID 23907247.
- ↑ Kleindorfer DO, Towfighi A, Chaturvedi S, Cockroft KM, Gutierrez J, Lombardi-Hill D; et al. (2021). "2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association". Stroke. 52 (7): e364–e467. doi:10.1161/STR.0000000000000375. PMID 34024117 Check
|pmid=value (help).