Foreign body
Template:DiseaseDisorder infobox
|
WikiDoc Resources for Foreign body |
|
Articles |
|---|
|
Most recent articles on Foreign body Most cited articles on Foreign body |
|
Media |
|
Powerpoint slides on Foreign body |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on Foreign body at Clinical Trials.gov Clinical Trials on Foreign body at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on Foreign body
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on Foreign body Discussion groups on Foreign body Patient Handouts on Foreign body Directions to Hospitals Treating Foreign body Risk calculators and risk factors for Foreign body
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for Foreign body |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
In physiology, a foreign body (Latin: corpus alienum) is any object originating outside the body. In machinery, it can mean any unwanted intruding object.
In Man
Foreign bodies typically become lodged in the eyes, ears, nose, airways, and rectum which are the main orifices of human beings. Foreign bodies can be in hollow organs (like swallowed batteries) or in tissues (like bullets). They can be inert or irritating. If they irritate they will cause inflammation and scarring. They can bring infection into the body or acquire infectious agents and protect them from the body's immune defenses. They can obstruct passageways either by their size or by the scarring they cause. Some can be toxic.
Both children and adults experience problems caused by foreign objects getting stuck in their bodies. Young children, in particular, are naturally curious and may intentionally put shiny objects, such as coins or button batteries, into their mouths. They also like to stick things in their ears and up their noses.[1] Adults may accidentally swallow a non-food object or inhale a foreign body that gets stuck in the throat. Airborne particles can lodge in the eyes of people at any age. These foreign bodies often result in allergies which are either temporary or even turn into a chronic allergy. This is especially evident in the case of dust particles.
Most objects that are swallowed will, if they have passed the pharynx, pass all the way through the gastrointestinal tract. Rarely an object becomes arrested (usually in the terminal ileum or the rectum) or a sharp object penetrates the bowel wall. If the person who swallowed the foreign body is doing well, usually a x-ray image will be taken which will show any metal objects, and this will be repeated a few days later to confirm that the object has passed all the way through the digestive system. Also it needs to be confirmed that the object is not stuck in the airways, in the bronchial tree. If the foreign body causes problems like pain, vomiting or bleeding it must be removed. Also swallowed mercury batteries should be removed as soon as possible as they are very dangerous especially to small children.
Examples
-
 Coin in esophagus
Coin in esophagus

-
 Chest X-ray showing a coin in the esophagus of a young child
Chest X-ray showing a coin in the esophagus of a young child -

-

-

-
 A screwdriver with a plastic handle. (Dr. A.K. Sharma, Agra, India
A screwdriver with a plastic handle. (Dr. A.K. Sharma, Agra, India -

-
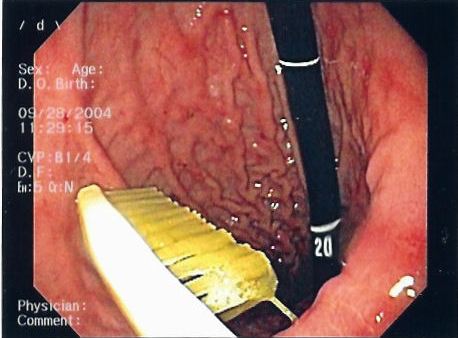 Gastric foreign body (toothbrush)
Gastric foreign body (toothbrush) -

-

-

-
 Gastric foreign body (toothbrush)
Gastric foreign body (toothbrush) -
 Rectal foreign body (Image courtesy of Dr Frank Gaillard)
Rectal foreign body (Image courtesy of Dr Frank Gaillard) -
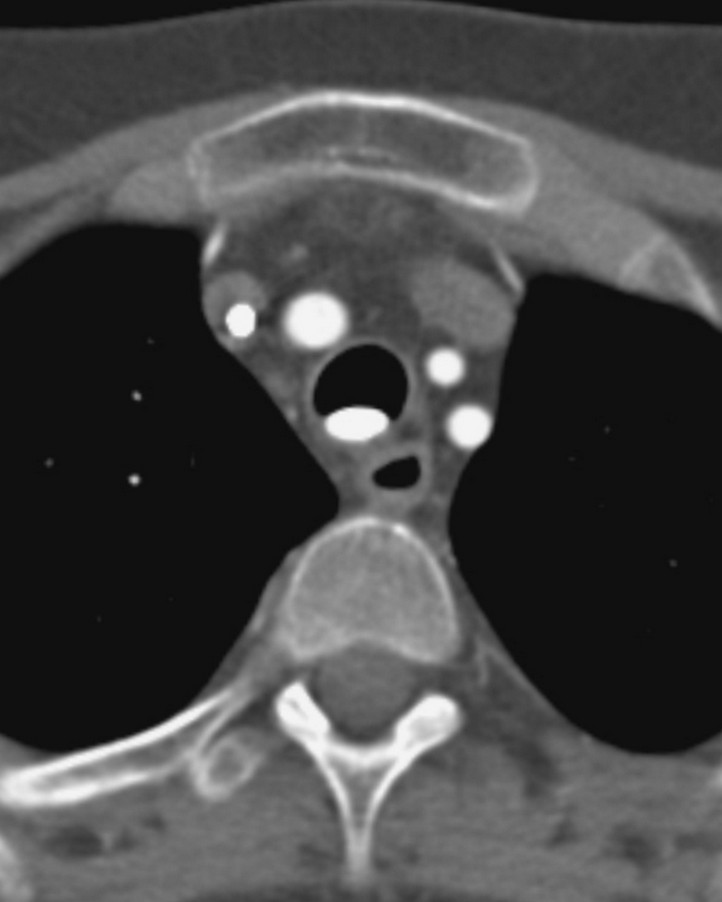
 This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard)
This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard) -
 This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard)
This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard) -
 This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard)
This patient collapsed on the ward and was thought to have had a pulmonary embolus. A CTPA revealed a tablet lying dependently in the patient's trachea, with changes of aspiration in both lower lobes (not shown). A second tablet was visible in the stomach... the tablet was removed via a bronchoscope and confirmed to be a Slow K (potassium). (Image courtesy of Dr Frank Gaillard) -
 Rectal foreign body (Image courtesy of Dr Frank Gaillard)
Rectal foreign body (Image courtesy of Dr Frank Gaillard) -
 Vaginal foreign body (Image courtesy of Dr Donna D'Souza)
Vaginal foreign body (Image courtesy of Dr Donna D'Souza) -
 This patient presented with a self-harm injury. The axial CT scan shows a ball-point pen in-situ. The pen missed optic nerve, middle cerebral artery and any eloquent brain. A cerebral angiogram was performed which was normal except for truncation of the ophthalmic artery. The pen was removed under flouroscopic guidance. Upon removal, there was brisk bleeding from the ophthalmic artery. Endovascular embolisation of the bleeding vessel was performed with coils, with good result. The patient’s pupil remains reactive, suggesting a good prognosis for the optic nerve and the patient’s vision. (Image courtesy of Dr Laughlin Dawes)
This patient presented with a self-harm injury. The axial CT scan shows a ball-point pen in-situ. The pen missed optic nerve, middle cerebral artery and any eloquent brain. A cerebral angiogram was performed which was normal except for truncation of the ophthalmic artery. The pen was removed under flouroscopic guidance. Upon removal, there was brisk bleeding from the ophthalmic artery. Endovascular embolisation of the bleeding vessel was performed with coils, with good result. The patient’s pupil remains reactive, suggesting a good prognosis for the optic nerve and the patient’s vision. (Image courtesy of Dr Laughlin Dawes) -
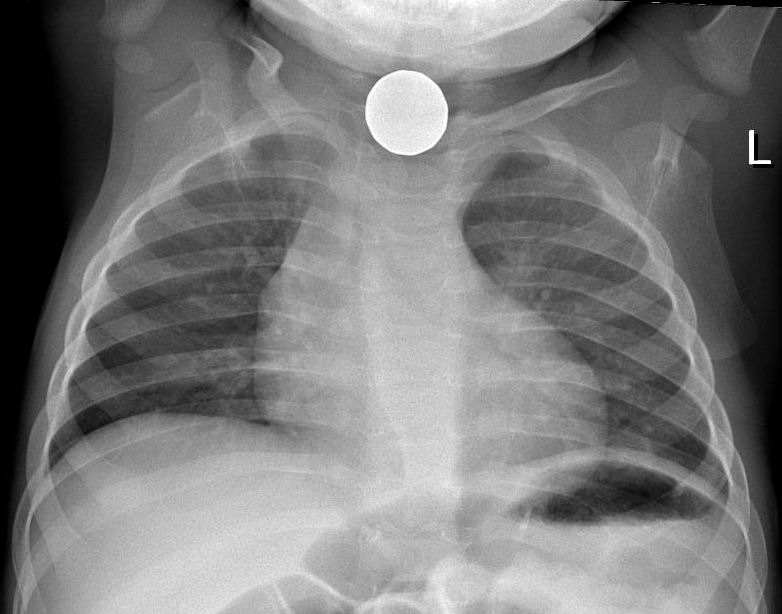
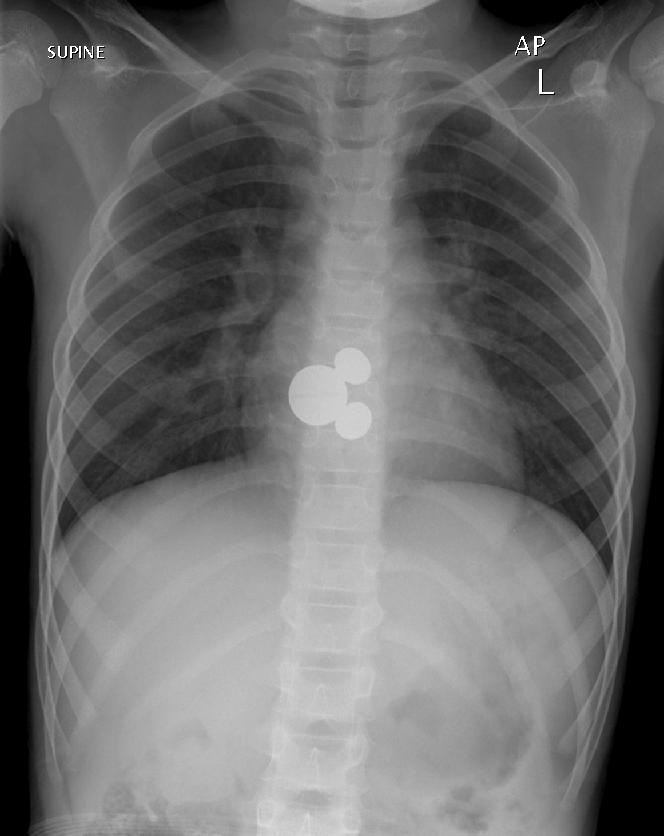 A 7 year old girl presented to ED after swallowing a foreign body. Initial CXR shows a foreign body at the level of T8. There was no change in the position of the Mickey Mouse key ring after 8 hours. No pneumomediastinum or pneumothorax. The airway is patent. It was finally retrieved with oesophagoscopy. (Image courtesy of Dr Lily Wang)
A 7 year old girl presented to ED after swallowing a foreign body. Initial CXR shows a foreign body at the level of T8. There was no change in the position of the Mickey Mouse key ring after 8 hours. No pneumomediastinum or pneumothorax. The airway is patent. It was finally retrieved with oesophagoscopy. (Image courtesy of Dr Lily Wang) -
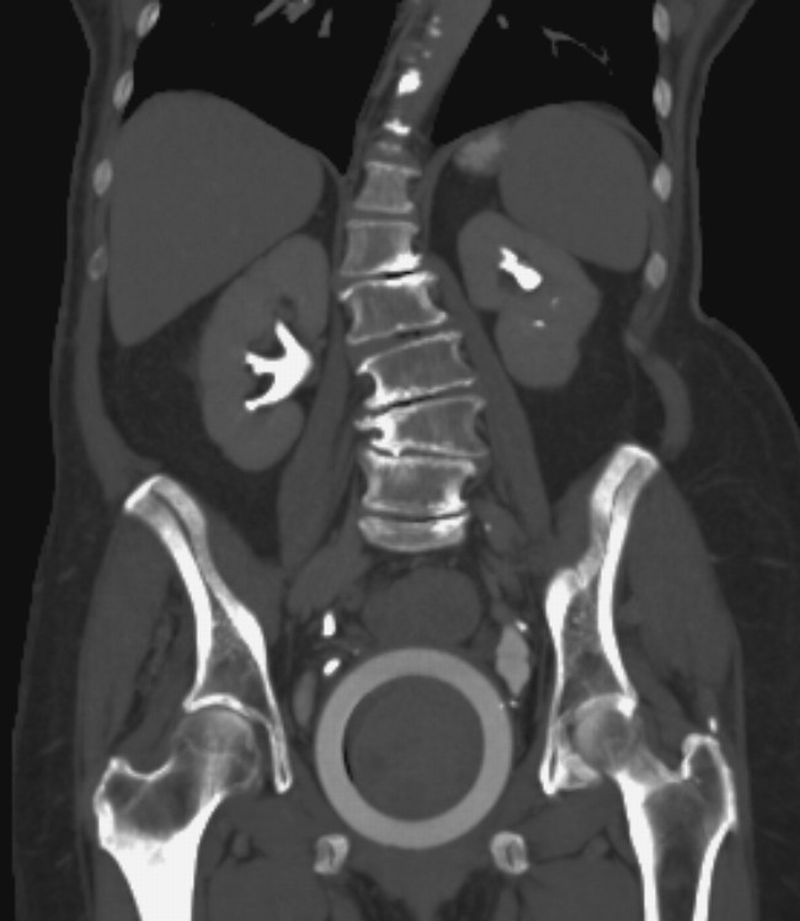
 A middle-aged male presented to the emergency department with abdominal discomfort. An abdominal radiograph was performed as shown. There is no evidence of perforation or obstruction. The patient was taken to operating room within 12 hours of presentation, with consent for colostomy. Under general anaesthesia in the lithotomy position, dilatation of anal sphincter was performed and per rectum retrieval successful. These patients typically have a delayed presentation to the emergency department because of embarrassment and after multiple attempts at self removal. Respect for their privacy is a key factor in the patient’s care plan. ED physicians need to decide if removal of foreign body can be performed in the emergency department or surgical team to be notified. Operating room procedures include anal dilatation under GA, transrectal manipulation, bimanual palpation if necessary and withdrawal of foreign body. Laparotomy or laparoscopy are occasionally necessary. (Image courtesy of Andrew Roshan)
A middle-aged male presented to the emergency department with abdominal discomfort. An abdominal radiograph was performed as shown. There is no evidence of perforation or obstruction. The patient was taken to operating room within 12 hours of presentation, with consent for colostomy. Under general anaesthesia in the lithotomy position, dilatation of anal sphincter was performed and per rectum retrieval successful. These patients typically have a delayed presentation to the emergency department because of embarrassment and after multiple attempts at self removal. Respect for their privacy is a key factor in the patient’s care plan. ED physicians need to decide if removal of foreign body can be performed in the emergency department or surgical team to be notified. Operating room procedures include anal dilatation under GA, transrectal manipulation, bimanual palpation if necessary and withdrawal of foreign body. Laparotomy or laparoscopy are occasionally necessary. (Image courtesy of Andrew Roshan) -
 Rectal foreign body. Body packer. (Image courtesy of Dr Frank Gaillard)
Rectal foreign body. Body packer. (Image courtesy of Dr Frank Gaillard) -
 Rectal foreign body (Image courtesy of Dr Frank Gaillard)
Rectal foreign body (Image courtesy of Dr Frank Gaillard) -
 Rectal foreign body (Image courtesy of Dr Frank Gaillard)
Rectal foreign body (Image courtesy of Dr Frank Gaillard) -
 Rectal foreign body (Image courtesy of Dr Frank Gaillard)
Rectal foreign body (Image courtesy of Dr Frank Gaillard) -
 (Image courtesy of Simon Pilgrim and Laughlin Dawes)
(Image courtesy of Simon Pilgrim and Laughlin Dawes) -
 Vaginal pessary for treatment of uterine prolapse (Image courtesy of Dr Frank Gaillard)
Vaginal pessary for treatment of uterine prolapse (Image courtesy of Dr Frank Gaillard) -
 This building-site worker inadvertently stapled-gunned his hand, neatly sitting in his interosseous space. (Image courtesy of Dr Frank Gaillard)
This building-site worker inadvertently stapled-gunned his hand, neatly sitting in his interosseous space. (Image courtesy of Dr Frank Gaillard) -
 This trauma patient had significant craniofacial injuries and aspirated a tooth. It lodged in the right lower lobe bronchus, causing post-obstructive consolidation. Inhaled foreign bodies may be complicated by haemoptysis, air trapping, post-obstructive collapse, pneumonia or bronchiectasis. Removal of the foreign body is usually performed via bronchoscopy. (Image courtesy of Dr Donna D'Souza)
This trauma patient had significant craniofacial injuries and aspirated a tooth. It lodged in the right lower lobe bronchus, causing post-obstructive consolidation. Inhaled foreign bodies may be complicated by haemoptysis, air trapping, post-obstructive collapse, pneumonia or bronchiectasis. Removal of the foreign body is usually performed via bronchoscopy. (Image courtesy of Dr Donna D'Souza) -
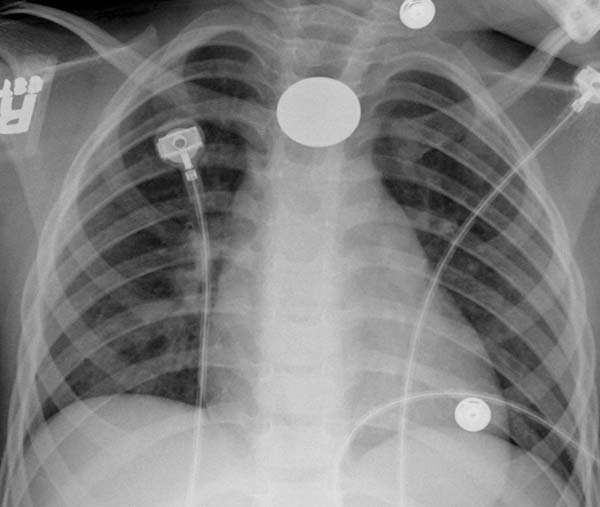
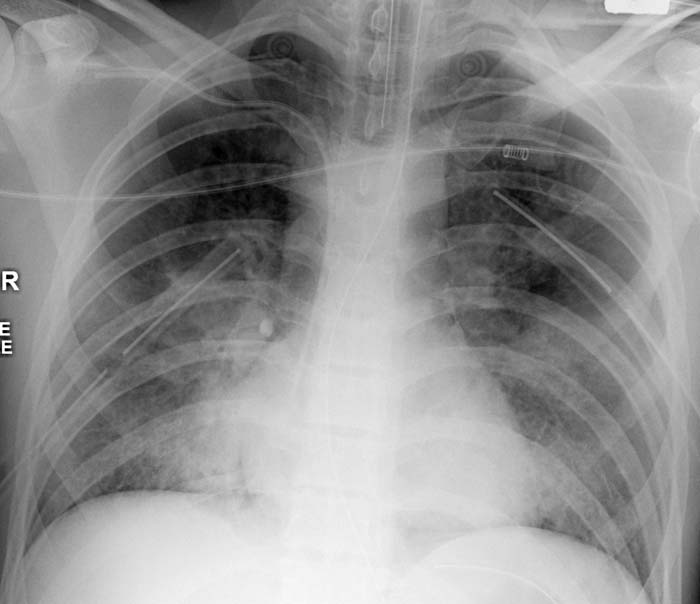
 This patient was transfered to ICU from another hospital. On examination of their abdomen a wire was noted to project through the right atrium, down the IVC to end in the right iliac vein. The J-shaped tip gave the game away... a right jugular CVC had been placed, and the wire used for the insertion pushed in with the catheter. This guide wire was successfully retrieved from the groin, without complication. (Image courtesy of Dr Frank Gaillard)
This patient was transfered to ICU from another hospital. On examination of their abdomen a wire was noted to project through the right atrium, down the IVC to end in the right iliac vein. The J-shaped tip gave the game away... a right jugular CVC had been placed, and the wire used for the insertion pushed in with the catheter. This guide wire was successfully retrieved from the groin, without complication. (Image courtesy of Dr Frank Gaillard) -
 This patient was transfered to ICU from another hospital. On examination of their abdomen a wire was noted to project through the right atrium, down the IVC to end in the right iliac vein. The J-shaped tip gave the game away... a right jugular CVC had been placed, and the wire used for the insertion pushed in with the catheter. This guide wire was successfully retrieved from the groin, without complication. (Image courtesy of Dr Frank Gaillard)
This patient was transfered to ICU from another hospital. On examination of their abdomen a wire was noted to project through the right atrium, down the IVC to end in the right iliac vein. The J-shaped tip gave the game away... a right jugular CVC had been placed, and the wire used for the insertion pushed in with the catheter. This guide wire was successfully retrieved from the groin, without complication. (Image courtesy of Dr Frank Gaillard)






























External Links
- Case report of Foreign Body Ingestion. Clinical Cases and Images.
Template:Consequences of external causes
References
- ↑ MERCK MANUAL, Professional edition, Ear, Nose, Throat, and Dental Disorders.