Vertebral artery dissection: Difference between revisions
No edit summary |
(/* Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: Management of Atherosclerotic Risk Factors in Patients with Vertebral Artery Disease{{cite journal| author=Brott TG, Halperin JL, Abbara S, Bacharac...) |
||
| Line 93: | Line 93: | ||
|- | |- | ||
| bgcolor="LightGreen"|<nowiki>"</nowiki>'''3.''' Antiplatelet drug therapy is recommended as part of the initial management for patients who sustain ischemic stroke or TIA associated with extracranial vertebral atherosclerosis. Aspirin (81 to 325 mg daily), the combination of aspirin plus extended-release dipyridamole (25 and 200 mg twice daily, respectively), and clopidogrel (75 mg daily) are acceptable options. Selection of an antiplatelet regimen should be individualized on the basis of patient risk factor profiles, cost, tolerance, and other clinical characteristics, as well as guidance from regulatory agencies. (Level of Evidence: B)'' <nowiki>"</nowiki> | | bgcolor="LightGreen"|<nowiki>"</nowiki>'''3.''' Antiplatelet drug therapy is recommended as part of the initial management for patients who sustain ischemic stroke or TIA associated with extracranial vertebral atherosclerosis. Aspirin (81 to 325 mg daily), the combination of aspirin plus extended-release dipyridamole (25 and 200 mg twice daily, respectively), and clopidogrel (75 mg daily) are acceptable options. Selection of an antiplatelet regimen should be individualized on the basis of patient risk factor profiles, cost, tolerance, and other clinical characteristics, as well as guidance from regulatory agencies. (Level of Evidence: B)'' <nowiki>"</nowiki> | ||
|} | |||
{|class="wikitable" | |||
|- | |||
| colspan="1" style="text-align:center; background:LemonChiffon"|[[ACC AHA guidelines classification scheme#Classification of Recommendations|Class IIa]] | |||
|- | |||
|bgcolor="LemonChiffon"|<nowiki>"</nowiki>'''1.''' For patients with atherosclerosis of the extracranial vertebral arteries in whom aspirin is contraindicated by factors other than active bleeding, including those with allergy to aspirin, either clopidogrel (75 mg daily) or ticlopidine (250 mg twice daily) is a reasonable alternative. (Level of Evidence: C)'' <nowiki>"</nowiki> | |||
|} | |} | ||
Revision as of 20:34, 3 October 2012
| Vertebral artery dissection | |
 | |
|---|---|
| Arteries of the neck | |
| ICD-9 | 443.24 |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Vertebral artery dissection is the development of dissection (a flap-like tear) in the vertebral artery. It is commonly associated with physical trauma but may also develop spontaneously. It is a major cause of stroke in young people.
Presentation
Typical features are pain in the neck associated with stroke-like symptoms of the "posterior circulation": cranial nerve palsies, ataxia, and cortical visual loss.[1] It can also cause subarachnoid hemorrhage (bleeding into the area around the brain); dissecting aneurysms of the vertebral artery represent about 4% of all aneurysms.[2]
Incidence
The annual incidence is about 1 per 100,000 in America and 1.5 per 100,000 in France.[2]
Diagnosis
Diagnostic Guidelines
Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: Recommendations for Vascular Imaging in Patients with Vertebral Arterial Disease[3](DO NOT EDIT)
| Class I |
| "1. Noninvasive imaging by CTA or MRA for detection of vertebral artery disease should be part of the initial evaluation of patients with neurological symptoms referable to the posterior circulation and those with subclavian steal syndrome. (Level of Evidence: C) " |
| "2. Patients with asymptomatic bilateral carotid occlusions or unilateral carotid artery occlusion and incomplete circle of Willis should undergo noninvasive imaging for detection of vertebral artery obstructive disease. (Level of Evidence: C) " |
| "3. In patients whose symptoms suggest posterior cerebral or cerebellar ischemia, MRA or CTA is recommended rather than ultrasound imaging for evaluation of the vertebral arteries. (Level of Evidence: C) " |
| Class IIa |
| "1. In patients with symptoms of posterior cerebral or cerebellar ischemia, serial noninvasive imaging of the extracranial vertebral arteries is reasonable to assess the progression of atherosclerotic disease and exclude the development of new lesions. (Level of Evidence: C) " |
| "2. In patients with posterior cerebral or cerebellar ischemic symptoms who may be candidates for revascularization, catheter-based contrast angiography can be useful to define vertebral artery pathoanatomy when noninvasive imaging fails to define the location or severity of stenosis. (Level of Evidence: C) " |
| "3. In patients who have undergone vertebral artery revascularization, serial noninvasive imaging of the extracranial vertebral arteries is reasonable at intervals similar to those for carotid revascularization. (Level of Evidence: C) " |
CT
-
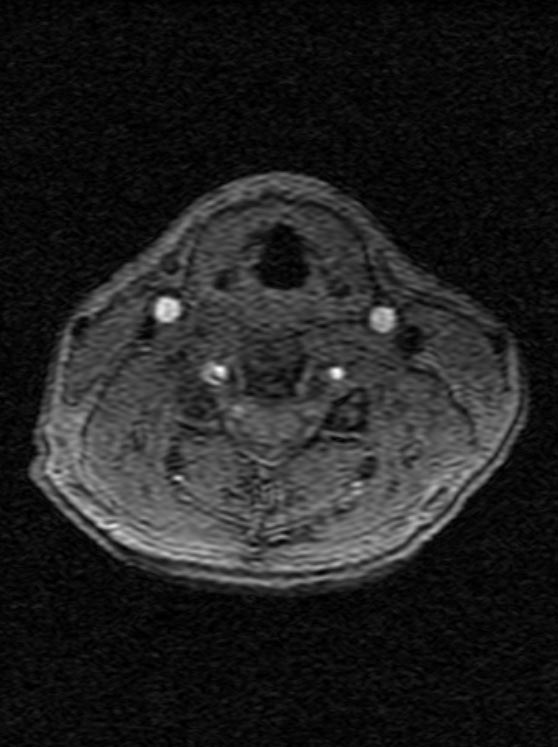
Vertebral artery dissection 1
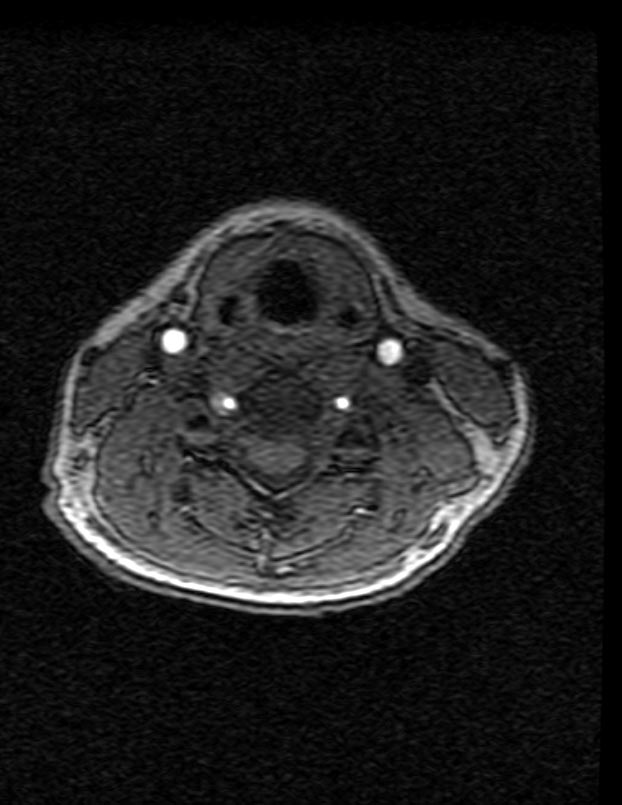
-

Vertebral artery dissection 2


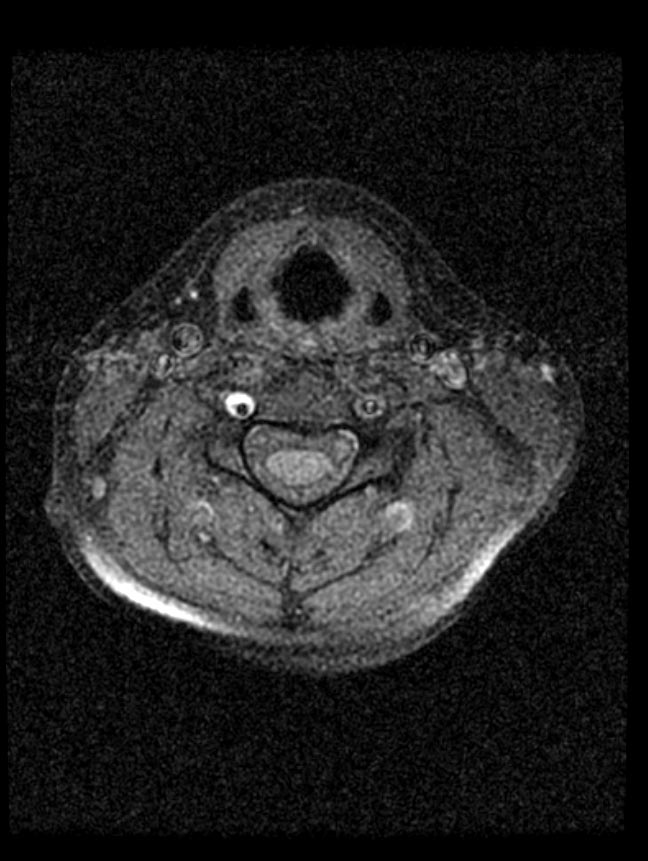
-
Vertebral artery dissection 3
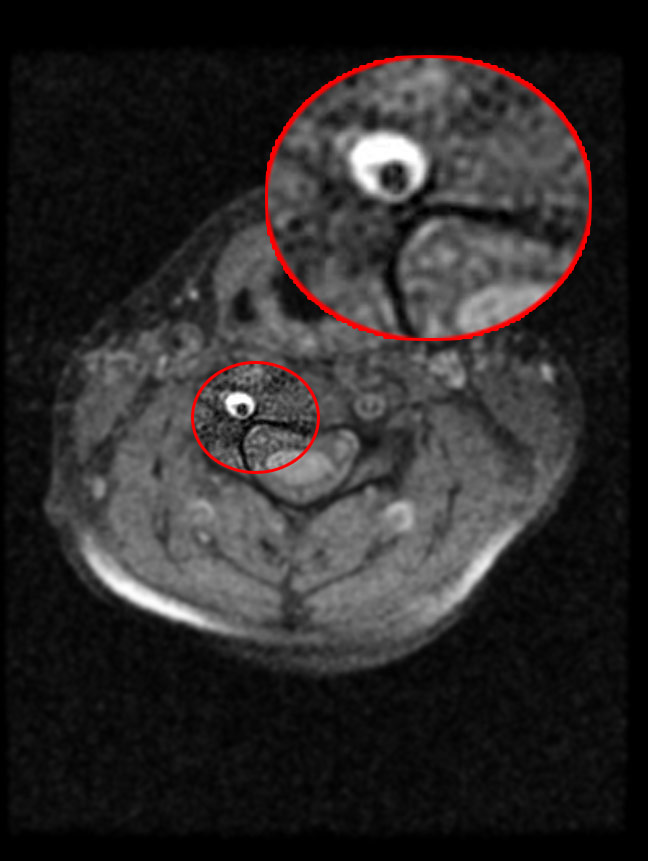
-

Vertebral artery dissection 4


-

Vertebral artery dissection 5
-
Vertebral artery dissection 6
-
Vertebral artery dissection 7



Treatment
Secondary Prevention
Guideline on the Management of Patients With Extracranial Carotid and Vertebral Artery Disease: Management of Atherosclerotic Risk Factors in Patients with Vertebral Artery Disease[3] (DO NOT EDIT)
| Class I |
| "1. Medical therapy and lifestyle modification to reduce atherosclerotic risk are recommended in patients with vertebral atherosclerosis according to the standards recommended for those with extracranial carotid atherosclerosis. (Level of Evidence: B) " |
| "2. In the absence of contraindications, patients with atherosclerosis involving the vertebral arteries should receive antiplatelet therapy with aspirin (75 to 325 mg daily) to prevent MI and other ischemic events. (Level of Evidence: B) " |
| "3. Antiplatelet drug therapy is recommended as part of the initial management for patients who sustain ischemic stroke or TIA associated with extracranial vertebral atherosclerosis. Aspirin (81 to 325 mg daily), the combination of aspirin plus extended-release dipyridamole (25 and 200 mg twice daily, respectively), and clopidogrel (75 mg daily) are acceptable options. Selection of an antiplatelet regimen should be individualized on the basis of patient risk factor profiles, cost, tolerance, and other clinical characteristics, as well as guidance from regulatory agencies. (Level of Evidence: B) " |
| Class IIa |
| "1. For patients with atherosclerosis of the extracranial vertebral arteries in whom aspirin is contraindicated by factors other than active bleeding, including those with allergy to aspirin, either clopidogrel (75 mg daily) or ticlopidine (250 mg twice daily) is a reasonable alternative. (Level of Evidence: C) " |
References
- ↑ Thanvi B, Munshi SK, Dawson SL, Robinson TG (2005). "Carotid and vertebral artery dissection syndromes". Postgrad Med J. 81 (956): 383–8. doi:10.1136/pgmj.2003.016774. PMID 15937204.
- ↑ 2.0 2.1 Santos-Franco JA, Zenteno M, Lee A (2008). "Dissecting aneurysms of the vertebrobasilar system. A comprehensive review on natural history and treatment options". Neurosurg Rev. doi:10.1007/s10143-008-0124-x. PMID 18309525.
- ↑ 3.0 3.1 Brott TG, Halperin JL, Abbara S, Bacharach JM, Barr JD, Bush RL; et al. (2011). "2011 ASA/ACCF/AHA/AANN/AANS/ACR/ASNR/CNS/SAIP/SCAI/SIR/SNIS/SVM/SVS guideline on the management of patients with extracranial carotid and vertebral artery disease: executive summary. A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American Stroke Association, American Association of Neuroscience Nurses, American Association of Neurological Surgeons, American College of Radiology, American Society of Neuroradiology, Congress of Neurological Surgeons, Society of Atherosclerosis Imaging and Prevention, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of NeuroInterventional Surgery, Society for Vascular Medicine, and Society for Vascular Surgery". Circulation. 124 (4): 489–532. doi:10.1161/CIR.0b013e31820d8d78. PMID 21282505.