Timothy syndrome is a rare syndrome that follows [[autosomal dominant]] inheritance pattern. Timothy syndrome is a multisystem disorder characterized by [[physiological]] and developmental defects which include long [[LQTS|QT-prolongation]], [[arrhythmia]]s, structural [[heart defects]], [[syndactyly]] and [[autism]] spectrum disorders. Timothy syndrome may be classified into 2 groups, classical form(type-1) and atypical form(type-2). Timothy syndrome caused by [[mutations]] in [[CACNA1C]], which encodes for [[calcium channel]] α subunit. Timothy syndrome often ends in early death. The United States of America in order to categorize a [[condition]] as a [[rare disease]] it should affect fewer than 200,000 people. [[Rare diseases]] also called as [[Orphan disease|orphan diseases]]. [[Orphan Drug Act]] was passed in 1983 by congress for the [[rare diseases]]. Today an average of 25-30 million Americans have been reported with [[rare diseases]]. The number of people with individual [[rare disease]] may be less but overall the number of people with [[rare diseases]] are large in number.
Timothy syndrome is a rare syndrome that follows [[autosomal dominant]] inheritance pattern. Timothy syndrome is a multisystem disorder characterized by [[physiological]] and developmental defects which include long [[LQTS|QT-prolongation]], [[arrhythmia]]s, structural [[heart defects]], [[syndactyly]] and [[autism]] [[spectrum]] disorders. Timothy syndrome may be classified into 2 groups, classical form(type-1) and atypical form(type-2). Timothy syndrome caused by [[mutations]] in [[CACNA1C]], which encodes for [[calcium channel]] α subunit. Timothy syndrome often ends in early death. The United States of America in order to categorize a [[condition]] as a [[rare disease]] it should affect fewer than 200,000 people. [[Rare diseases]] also called as [[Orphan disease|orphan diseases]]. [[Orphan Drug Act]] was passed in 1983 by congress for the [[rare diseases]]. Today an average of 25-30 million Americans have been reported with [[rare diseases]]. The number of people with individual [[rare disease]] may be less but overall the number of people with [[rare diseases]] are large in number.
==Historical Perspective==
==Historical Perspective==
Line 11:
Line 12:
* Timothy syndrome was first discovered by Reichenbach and Marks, in 1992.<ref name="pmid1318983">{{cite journal| author=Reichenbach H, Meister EM, Theile H| title=[The heart-hand syndrome. A new variant of disorders of heart conduction and syndactylia including osseous changes in hands and feet]. | journal=Kinderarztl Prax | year= 1992 | volume= 60 | issue= 2 | pages= 54-6 | pmid=1318983 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1318983 }}</ref><ref name="pmid7572644">{{cite journal| author=Marks ML, Trippel DL, Keating MT| title=Long QT syndrome associated with syndactyly identified in females. | journal=Am J Cardiol | year= 1995 | volume= 76 | issue= 10 | pages= 744-5 | pmid=7572644 | doi=10.1016/s0002-9149(99)80216-1 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7572644 }}</ref>
* Timothy syndrome was first discovered by Reichenbach and Marks, in 1992.<ref name="pmid1318983">{{cite journal| author=Reichenbach H, Meister EM, Theile H| title=[The heart-hand syndrome. A new variant of disorders of heart conduction and syndactylia including osseous changes in hands and feet]. | journal=Kinderarztl Prax | year= 1992 | volume= 60 | issue= 2 | pages= 54-6 | pmid=1318983 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1318983 }}</ref><ref name="pmid7572644">{{cite journal| author=Marks ML, Trippel DL, Keating MT| title=Long QT syndrome associated with syndactyly identified in females. | journal=Am J Cardiol | year= 1995 | volume= 76 | issue= 10 | pages= 744-5 | pmid=7572644 | doi=10.1016/s0002-9149(99)80216-1 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7572644 }}</ref>
* In 1995, Splawski, Reichenbach, and Marks were the first to give the name Timothy syndrome in the honor of Dr. Katherine W. Timothy who did the [[Phenotype|phenotypic]] analysis.<ref name="pmid221060443">{{cite journal| author=Gillis J, Burashnikov E, Antzelevitch C, Blaser S, Gross G, Turner L et al.| title=Long QT, syndactyly, joint contractures, stroke and novel CACNA1C mutation: expanding the spectrum of Timothy syndrome. | journal=Am J Med Genet A | year= 2012 | volume= 158A | issue= 1 | pages= 182-7 | pmid=22106044 | doi=10.1002/ajmg.a.34355 | pmc=3319791 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22106044 }}</ref>
* In 1995, Splawski, Reichenbach, and Marks were the first to give the name Timothy syndrome in the honor of Dr.Katherine W. Timothy who did the [[Phenotype|phenotypic]] analysis.<ref name="pmid221060443">{{cite journal| author=Gillis J, Burashnikov E, Antzelevitch C, Blaser S, Gross G, Turner L et al.| title=Long QT, syndactyly, joint contractures, stroke and novel CACNA1C mutation: expanding the spectrum of Timothy syndrome. | journal=Am J Med Genet A | year= 2012 | volume= 158A | issue= 1 | pages= 182-7 | pmid=22106044 | doi=10.1002/ajmg.a.34355 | pmc=3319791 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22106044 }}</ref>
== Classification ==
== Classification ==
* Timothy syndrome may be classified into 2 groups as follows:<ref name="pmid8392192">{{cite journal| author=Schultz D, Mikala G, Yatani A, Engle DB, Iles DE, Segers B et al.| title=Cloning, chromosomal localization, and functional expression of the alpha 1 subunit of the L-type voltage-dependent calcium channel from normal human heart. | journal=Proc Natl Acad Sci U S A | year= 1993 | volume= 90 | issue= 13 | pages= 6228-32 | pmid=8392192 | doi=10.1073/pnas.90.13.6228 | pmc=46901 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=8392192 }}</ref><ref name="pmid7737988">{{cite journal| author=Soldatov NM, Bouron A, Reuter H| title=Different voltage-dependent inhibition by dihydropyridines of human Ca2+ channel splice variants. | journal=J Biol Chem | year= 1995 | volume= 270 | issue= 18 | pages= 10540-3 | pmid=7737988 | doi=10.1074/jbc.270.18.10540 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7737988 }}</ref><ref name="pmid12176756">{{cite journal| author=Lyford GL, Strege PR, Shepard A, Ou Y, Ermilov L, Miller SM et al.| title=alpha(1C) (Ca(V)1.2) L-type calcium channel mediates mechanosensitive calcium regulation. | journal=Am J Physiol Cell Physiol | year= 2002 | volume= 283 | issue= 3 | pages= C1001-8 | pmid=12176756 | doi=10.1152/ajpcell.00140.2002 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12176756 }}</ref>
* Timothy syndrome may be classified into 2 groups as follows:<ref name="pmid8392192">{{cite journal| author=Schultz D, Mikala G, Yatani A, Engle DB, Iles DE, Segers B et al.| title=Cloning, chromosomal localization, and functional expression of the alpha 1 subunit of the L-type voltage-dependent calcium channel from normal human heart. | journal=Proc Natl Acad Sci U S A | year= 1993 | volume= 90 | issue= 13 | pages= 6228-32 | pmid=8392192 | doi=10.1073/pnas.90.13.6228 | pmc=46901 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=8392192 }}</ref><ref name="pmid25691416">{{cite journal| author=Hiippala A, Tallila J, Myllykangas S, Koskenvuo JW, Alastalo TP| title=Expanding the phenotype of Timothy syndrome type 2: an adolescent with ventricular fibrillation but normal development. | journal=Am J Med Genet A | year= 2015 | volume= 167A | issue= 3 | pages= 629-34 | pmid=25691416 | doi=10.1002/ajmg.a.36924 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=25691416 }}</ref><ref name="pmid7737988">{{cite journal| author=Soldatov NM, Bouron A, Reuter H| title=Different voltage-dependent inhibition by dihydropyridines of human Ca2+ channel splice variants. | journal=J Biol Chem | year= 1995 | volume= 270 | issue= 18 | pages= 10540-3 | pmid=7737988 | doi=10.1074/jbc.270.18.10540 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7737988 }}</ref><ref name="pmid12176756">{{cite journal| author=Lyford GL, Strege PR, Shepard A, Ou Y, Ermilov L, Miller SM et al.| title=alpha(1C) (Ca(V)1.2) L-type calcium channel mediates mechanosensitive calcium regulation. | journal=Am J Physiol Cell Physiol | year= 2002 | volume= 283 | issue= 3 | pages= C1001-8 | pmid=12176756 | doi=10.1152/ajpcell.00140.2002 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=12176756 }}</ref>
*It is understood that Timothy syndrome both classical and atypical form is the result of a [[missense mutation]] in the [[CACNA1C]] [[gene]].<ref name="pmid28371864">{{cite journal| author=Walsh MA, Turner C, Timothy KW, Seller N, Hares DL, James AF et al.| title=A multicentre study of patients with Timothy syndrome. | journal=Europace | year= 2018 | volume= 20 | issue= 2 | pages= 377-385 | pmid=28371864 | doi=10.1093/europace/euw433 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=28371864 }}</ref><ref name="pmid27868338">{{cite journal| author=Baurand A, Falcon-Eicher S, Laurent G, Villain E, Bonnet C, Thauvin-Robinet C et al.| title=Incomplete Timothy syndrome secondary to a mosaic mutation of the CACNA1C gene diagnosed using next-generation sequencing. | journal=Am J Med Genet A | year= 2017 | volume= 173 | issue= 2 | pages= 531-536 | pmid=27868338 | doi=10.1002/ajmg.a.38045 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=27868338 }}</ref>
*It is understood that Timothy syndrome both classical and atypical form is the result of a [[missense mutation]] in the [[CACNA1C]] [[gene]].<ref name="pmid28371864">{{cite journal| author=Walsh MA, Turner C, Timothy KW, Seller N, Hares DL, James AF et al.| title=A multicentre study of patients with Timothy syndrome. | journal=Europace | year= 2018 | volume= 20 | issue= 2 | pages= 377-385 | pmid=28371864 | doi=10.1093/europace/euw433 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=28371864 }}</ref><ref name="pmid27868338">{{cite journal| author=Baurand A, Falcon-Eicher S, Laurent G, Villain E, Bonnet C, Thauvin-Robinet C et al.| title=Incomplete Timothy syndrome secondary to a mosaic mutation of the CACNA1C gene diagnosed using next-generation sequencing. | journal=Am J Med Genet A | year= 2017 | volume= 173 | issue= 2 | pages= 531-536 | pmid=27868338 | doi=10.1002/ajmg.a.38045 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=27868338 }}</ref><ref name="pmid21700933">{{cite journal| author=Cheng EP, Yuan C, Navedo MF, Dixon RE, Nieves-Cintrón M, Scott JD et al.| title=Restoration of normal L-type Ca2+ channel function during Timothy syndrome by ablation of an anchoring protein. | journal=Circ Res | year= 2011 | volume= 109 | issue= 3 | pages= 255-61 | pmid=21700933 | doi=10.1161/CIRCRESAHA.111.248252 | pmc=3151468 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=21700933 }}</ref>
*[[CACNA1C]] [[gene]] encodes for [[calcium channel]] α [[subunit]] across [[cell membranes]].
*[[CACNA1C]] [[gene]] encodes for [[calcium channel]] α [[subunit]] across [[cell membranes]].
*Any [[missense mutation]] in exon 8 (atypical form) and exon 8a (classical form) of [[CACNA1C]] [[gene]] results in structural changes of Ca(V)1.2[[Ion channel|channels]] and delayed [[calcium channel]] α subunit closing and, thus, increased [[cellular]] excitability.<ref name="pmid15454078">{{cite journal| author=Splawski I, Timothy KW, Sharpe LM, Decher N, Kumar P, Bloise R et al.| title=Ca(V)1.2 calcium channel dysfunction causes a multisystem disorder including arrhythmia and autism. | journal=Cell | year= 2004 | volume= 119 | issue= 1 | pages= 19-31 | pmid=15454078 | doi=10.1016/j.cell.2004.09.011 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=15454078 }}</ref><ref name="pmid22999068">{{cite journal| author=Dixon RE, Cheng EP, Mercado JL, Santana LF| title=L-type Ca2+ channel function during Timothy syndrome. | journal=Trends Cardiovasc Med | year= 2012 | volume= 22 | issue= 3 | pages= 72-6 | pmid=22999068 | doi=10.1016/j.tcm.2012.06.015 | pmc=3640256 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22999068 }}</ref><ref name="pmid26822303">{{cite journal| author=Dick IE, Joshi-Mukherjee R, Yang W, Yue DT| title=Arrhythmogenesis in Timothy Syndrome is associated with defects in Ca(2+)-dependent inactivation. | journal=Nat Commun | year= 2016 | volume= 7 | issue= | pages= 10370 | pmid=26822303 | doi=10.1038/ncomms10370 | pmc=4740114 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=26822303 }}</ref>
*Any [[missense mutation]] in [[exon]] 8 (atypical form) and [[exon]] 8a (classical form) of [[CACNA1C]] [[gene]] results in structural changes of Ca(V)1.2[[Ion channel|channels]] and delayed [[calcium channel]] α subunit closing and, thus, increased [[cellular]] excitability.<ref name="pmid15454078">{{cite journal| author=Splawski I, Timothy KW, Sharpe LM, Decher N, Kumar P, Bloise R et al.| title=Ca(V)1.2 calcium channel dysfunction causes a multisystem disorder including arrhythmia and autism. | journal=Cell | year= 2004 | volume= 119 | issue= 1 | pages= 19-31 | pmid=15454078 | doi=10.1016/j.cell.2004.09.011 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=15454078 }}</ref><ref name="pmid22999068">{{cite journal| author=Dixon RE, Cheng EP, Mercado JL, Santana LF| title=L-type Ca2+ channel function during Timothy syndrome. | journal=Trends Cardiovasc Med | year= 2012 | volume= 22 | issue= 3 | pages= 72-6 | pmid=22999068 | doi=10.1016/j.tcm.2012.06.015 | pmc=3640256 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22999068 }}</ref><ref name="pmid26822303">{{cite journal| author=Dick IE, Joshi-Mukherjee R, Yang W, Yue DT| title=Arrhythmogenesis in Timothy Syndrome is associated with defects in Ca(2+)-dependent inactivation. | journal=Nat Commun | year= 2016 | volume= 7 | issue= | pages= 10370 | pmid=26822303 | doi=10.1038/ncomms10370 | pmc=4740114 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=26822303 }}</ref>
*There is one more mutation in ''G406R'' that is associated with the timothy syndrome.<ref name="pmid1149428">{{cite journal| author=De Oliveira CC, Figueiredo EA, Gazzinelli G, Howells RE, Pellegrino J| title=Biochemical changes in the transformation of Schistosoma mansoni cercariae to schistosomules. | journal=Comp Biochem Physiol B | year= 1975 | volume= 51 | issue= 4 | pages= 417-20 | pmid=1149428 | doi=10.1016/0305-0491(75)90031-0 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1149428 }}</ref>
*There is one more [[mutation]] in ''G406R'' that is associated with the timothy syndrome.<ref name="pmid282119895">{{cite journal| author=Sepp R, Hategan L, Bácsi A, Cseklye J, Környei L, Borbás J et al.| title=Timothy syndrome 1 genotype without syndactyly and major extracardiac manifestations. | journal=Am J Med Genet A | year= 2017 | volume= 173 | issue= 3 | pages= 784-789 | pmid=28211989 | doi=10.1002/ajmg.a.38084 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=28211989 }}</ref><ref name="pmid1149428">{{cite journal| author=De Oliveira CC, Figueiredo EA, Gazzinelli G, Howells RE, Pellegrino J| title=Biochemical changes in the transformation of Schistosoma mansoni cercariae to schistosomules. | journal=Comp Biochem Physiol B | year= 1975 | volume= 51 | issue= 4 | pages= 417-20 | pmid=1149428 | doi=10.1016/0305-0491(75)90031-0 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=1149428 }}</ref>
*The location of ''G406R'' is in domain one segment six (''D1S6'') which holds glycine at this position and plays a very important role in voltage-dependent inactivation
*The location of ''G406R'' is in domain one segment six (''D1S6'') which holds [[glycine]] at this position and plays a very important role in [[voltage]]-dependent inactivation.
*[[Calcium channel]] α subunit especially Ca(V)1.2 involved in transporting positively charged [[calcium ions]] into the [[cells]] across a [[cell membrane]] which plays a critical role in the normal function of [[heart]] and [[brain]] cells
*[[Calcium channel]] α subunit especially [[Ca]](V)1.2 involved in transporting positively charged [[calcium ions]] into the [[cells]] across a [[cell membrane]] which plays a critical role in the normal function of [[heart]] and [[brain]] [[Cells (biology)|cells]].
*[[Mutation|Mutations]] in Ca(V)1.2 [[Calcium channel|calcium channels]] leads to disruption of the following events in the [[heart]] and other organs:<ref name="pmid259819772">{{cite journal| author=Betzenhauser MJ, Pitt GS, Antzelevitch C| title=Calcium Channel Mutations in Cardiac Arrhythmia Syndromes. | journal=Curr Mol Pharmacol | year= 2015 | volume= 8 | issue= 2 | pages= 133-42 | pmid=25981977 | doi=10.2174/1874467208666150518114857 | pmc=4762596 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=25981977 }}</ref>
*[[Mutation|Mutations]] in Ca(V)1.2 [[Calcium channel|calcium channels]] leads to disruption of the following events in the [[heart]] and other organs:<ref name="pmid259819772">{{cite journal| author=Betzenhauser MJ, Pitt GS, Antzelevitch C| title=Calcium Channel Mutations in Cardiac Arrhythmia Syndromes. | journal=Curr Mol Pharmacol | year= 2015 | volume= 8 | issue= 2 | pages= 133-42 | pmid=25981977 | doi=10.2174/1874467208666150518114857 | pmc=4762596 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=25981977 }}</ref>
**Cell-to-cell communication
**Cell-to-cell communication
Line 57:
Line 58:
**Normal regulation of certain [[genes]]
**Normal regulation of certain [[genes]]
* Due to the fact that [[exon]] 8(atypical Timothy syndrome) is more expressed in heart muscles than that of exon 8a(classic Timothy syndrome) patients with exon 8 mutation have a severe form of long QT interval.
* Due to the fact that [[exon]] 8(atypical Timothy syndrome) is more expressed in heart muscles than that of [[exon]] 8a(classic Timothy syndrome) patients with [[exon]] 8 [[mutation]] have a severe form of long [[QT interval]].
== Causes ==
== Causes ==
Line 63:
Line 64:
=== Genetic Causes ===
=== Genetic Causes ===
* Timothy syndrome is caused by a [[Missense mutation|missense]] [[mutation]] in the [[CACNA1C]] [[gene]].
* Timothy syndrome is caused by a [[Missense mutation|missense]] [[mutation]] in the [[CACNA1C]] [[gene]].<ref name="pmid25882468">{{cite journal| author=Corona-Rivera JR, Barrios-Prieto E, Nieto-García R, Bloise R, Priori S, Napolitano C et al.| title=Unusual retrospective prenatal findings in a male newborn with Timothy syndrome type 1. | journal=Eur J Med Genet | year= 2015 | volume= 58 | issue= 6-7 | pages= 332-5 | pmid=25882468 | doi=10.1016/j.ejmg.2015.04.001 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=25882468 }}</ref><ref name="pmid25260352">{{cite journal| author=Boczek NJ, Miller EM, Ye D, Nesterenko VV, Tester DJ, Antzelevitch C et al.| title=Novel Timothy syndrome mutation leading to increase in CACNA1C window current. | journal=Heart Rhythm | year= 2015 | volume= 12 | issue= 1 | pages= 211-9 | pmid=25260352 | doi=10.1016/j.hrthm.2014.09.051 | pmc=4907369 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=25260352 }}</ref>
== Differentiating Timothy syndrome from other Diseases ==
== Differentiating Timothy syndrome from other Diseases ==
Line 108:
Line 109:
=== Natural History ===
=== Natural History ===
* The [[symptoms]] of Timothy syndrome usually develop in the first decade of life, and start with [[Symptom|symptoms]] such as [[cardiac]], hand/foot, facial, and [[Neurodevelopmental disorders|neurodevelopmental]] symptoms.
* The [[symptoms]] of Timothy syndrome usually develop in the first decade of life, and start with [[Symptom|symptoms]] such as [[cardiac]], [[hand]]/[[foot]], [[facial]], and [[Neurodevelopmental disorders|neurodevelopmental]] symptoms.
=== Complications ===
=== Complications ===
Line 115:
Line 116:
**[[Ventricular tachyarrhythmia]] which includes both [[ventricular tachycardia]] and [[ventricular fibrillation]] is the cause of death in most of the patients with Timothy syndrome
**[[Ventricular tachyarrhythmia]] which includes both [[ventricular tachycardia]] and [[ventricular fibrillation]] is the cause of death in most of the patients with Timothy syndrome
** Severe [[infections]] due to weakened [[immune system]](despite aggressive [[antibiotic therapy]])
** Severe [[infections]] due to weakened [[immune system]](despite aggressive [[antibiotic therapy]])
** Intractable [[hypoglycemia]]
** Intractable [[hypoglycemia]]<ref name="pmid282119894">{{cite journal| author=Sepp R, Hategan L, Bácsi A, Cseklye J, Környei L, Borbás J et al.| title=Timothy syndrome 1 genotype without syndactyly and major extracardiac manifestations. | journal=Am J Med Genet A | year= 2017 | volume= 173 | issue= 3 | pages= 784-789 | pmid=28211989 | doi=10.1002/ajmg.a.38084 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=28211989 }}</ref>
=== Prognosis ===
=== Prognosis ===
Line 128:
Line 129:
*[[Sequence analysis]](100% detectable), Targeted [[analysis]] for [[pathogenic]] variants(>95% detectable), [[Gene]]-targeted [[deletion]]/duplication [[analysis]] of ''[[CACNA1C]]'' [[gene]] testing is the [[Gold standard (test)|gold standard]] test for the [[diagnosis]] of Timothy syndrome.<ref name="pmid221060442">{{cite journal| author=Gillis J, Burashnikov E, Antzelevitch C, Blaser S, Gross G, Turner L et al.| title=Long QT, syndactyly, joint contractures, stroke and novel CACNA1C mutation: expanding the spectrum of Timothy syndrome. | journal=Am J Med Genet A | year= 2012 | volume= 158A | issue= 1 | pages= 182-7 | pmid=22106044 | doi=10.1002/ajmg.a.34355 | pmc=3319791 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22106044 }}</ref>
*[[Sequence analysis]](100% detectable), Targeted [[analysis]] for [[pathogenic]] variants(>95% detectable), [[Gene]]-targeted [[deletion]]/duplication [[analysis]] of ''[[CACNA1C]]'' [[gene]] testing is the [[Gold standard (test)|gold standard]] test for the [[diagnosis]] of Timothy syndrome.<ref name="pmid221060442">{{cite journal| author=Gillis J, Burashnikov E, Antzelevitch C, Blaser S, Gross G, Turner L et al.| title=Long QT, syndactyly, joint contractures, stroke and novel CACNA1C mutation: expanding the spectrum of Timothy syndrome. | journal=Am J Med Genet A | year= 2012 | volume= 158A | issue= 1 | pages= 182-7 | pmid=22106044 | doi=10.1002/ajmg.a.34355 | pmc=3319791 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=22106044 }}</ref>
*Along with the genetic testing patients also evaluate for following recommendations:
*Along with the [[Genetics|genetic]] testing patients also evaluate for following recommendations:
Common [[symptoms]] of Timothy syndrome include:<ref name="pmid249323603">{{cite journal| author=Tester DJ, Ackerman MJ| title=Genetics of long QT syndrome. | journal=Methodist Debakey Cardiovasc J | year= 2014 | volume= 10 | issue= 1 | pages= 29-33 | pmid=24932360 | doi=10.14797/mdcj-10-1-29 | pmc=4051331 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=24932360 }}</ref><ref name="pmid282119893">{{cite journal| author=Sepp R, Hategan L, Bácsi A, Cseklye J, Környei L, Borbás J et al.| title=Timothy syndrome 1 genotype without syndactyly and major extracardiac manifestations. | journal=Am J Med Genet A | year= 2017 | volume= 173 | issue= 3 | pages= 784-789 | pmid=28211989 | doi=10.1002/ajmg.a.38084 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=28211989 }}</ref>
*[[Torsade de pointes]]
*[[Torsade de pointes]]
Line 148:
Line 149:
=== Less Common Symptoms ===
=== Less Common Symptoms ===
Less common [[Symptom|symptoms]] of Timothy syndrome include
Less common [[Symptom|symptoms]] of Timothy syndrome include:<ref name="pmid249323602">{{cite journal| author=Tester DJ, Ackerman MJ| title=Genetics of long QT syndrome. | journal=Methodist Debakey Cardiovasc J | year= 2014 | volume= 10 | issue= 1 | pages= 29-33 | pmid=24932360 | doi=10.14797/mdcj-10-1-29 | pmc=4051331 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=24932360 }}</ref><ref name="pmid256914162">{{cite journal| author=Hiippala A, Tallila J, Myllykangas S, Koskenvuo JW, Alastalo TP| title=Expanding the phenotype of Timothy syndrome type 2: an adolescent with ventricular fibrillation but normal development. | journal=Am J Med Genet A | year= 2015 | volume= 167A | issue= 3 | pages= 629-34 | pmid=25691416 | doi=10.1002/ajmg.a.36924 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=25691416 }}</ref>
*[[Ventricular fibrillation]]
*[[Ventricular fibrillation]]
Line 156:
Line 157:
== Electrocardiogram ==
== Electrocardiogram ==
* An [[The electrocardiogram|ECG]] is helpful in the [[diagnosis]] of Timothy syndrome. Findings on an [[The electrocardiogram|ECG]] [[diagnostic]] of Timothy syndrome include the following:<ref name="pmid21185501">{{cite journal| author=Goldenberg I, Horr S, Moss AJ, Lopes CM, Barsheshet A, McNitt S et al.| title=Risk for life-threatening cardiac events in patients with genotype-confirmed long-QT syndrome and normal-range corrected QT intervals. | journal=J Am Coll Cardiol | year= 2011 | volume= 57 | issue= 1 | pages= 51-9 | pmid=21185501 | doi=10.1016/j.jacc.2010.07.038 | pmc=3332533 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=21185501 }}</ref><ref name="pmid1318983" /><ref name="pmid7798527">{{cite journal| author=Marks ML, Whisler SL, Clericuzio C, Keating M| title=A new form of long QT syndrome associated with syndactyly. | journal=J Am Coll Cardiol | year= 1995 | volume= 25 | issue= 1 | pages= 59-64 | pmid=7798527 | doi=10.1016/0735-1097(94)00318-k | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7798527 }}</ref><ref name="pmid15863612">{{cite journal| author=Splawski I, Timothy KW, Decher N, Kumar P, Sachse FB, Beggs AH et al.| title=Severe arrhythmia disorder caused by cardiac L-type calcium channel mutations. | journal=Proc Natl Acad Sci U S A | year= 2005 | volume= 102 | issue= 23 | pages= 8089-96; discussion 8086-8 | pmid=15863612 | doi=10.1073/pnas.0502506102 | pmc=1149428 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=15863612 }}</ref>
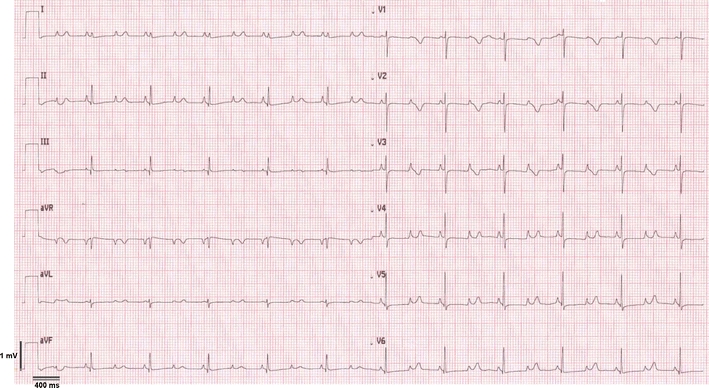
*[[File:Prolonged QT interval (QTc 600 ms).jpg|thumb|Trimonth syndrome ECG after birth showed a prolonged QT interval (QTc 600 ms), 2:1 atrioventricular block and significant bradycardia (ventricular rate 60/min). Case courtesy by U. Krause Et Al<ref>{{Cite web|url=https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3222804/|title=A rare association of long QT syndrome and syndactyly: Timothy Syndrome (LQT 8)|last=|first=|date=|website=|archive-url=|archive-date=|dead-url=|access-date=}}</ref>]]An [[The electrocardiogram|ECG]] is helpful in the [[diagnosis]] of Timothy syndrome. Findings on an [[The electrocardiogram|ECG]] [[diagnostic]] of Timothy syndrome include the following:<ref name="pmid21185501">{{cite journal| author=Goldenberg I, Horr S, Moss AJ, Lopes CM, Barsheshet A, McNitt S et al.| title=Risk for life-threatening cardiac events in patients with genotype-confirmed long-QT syndrome and normal-range corrected QT intervals. | journal=J Am Coll Cardiol | year= 2011 | volume= 57 | issue= 1 | pages= 51-9 | pmid=21185501 | doi=10.1016/j.jacc.2010.07.038 | pmc=3332533 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=21185501 }}</ref><ref name="pmid1318983" /><ref name="pmid7798527">{{cite journal| author=Marks ML, Whisler SL, Clericuzio C, Keating M| title=A new form of long QT syndrome associated with syndactyly. | journal=J Am Coll Cardiol | year= 1995 | volume= 25 | issue= 1 | pages= 59-64 | pmid=7798527 | doi=10.1016/0735-1097(94)00318-k | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=7798527 }}</ref><ref name="pmid15863612">{{cite journal| author=Splawski I, Timothy KW, Decher N, Kumar P, Sachse FB, Beggs AH et al.| title=Severe arrhythmia disorder caused by cardiac L-type calcium channel mutations. | journal=Proc Natl Acad Sci U S A | year= 2005 | volume= 102 | issue= 23 | pages= 8089-96; discussion 8086-8 | pmid=15863612 | doi=10.1073/pnas.0502506102 | pmc=1149428 | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=15863612 }}</ref>
** Prolongation of the [[QTc interval]] with an average [[QT interval|QTc]] of 580 ms in classic Timothy syndrome
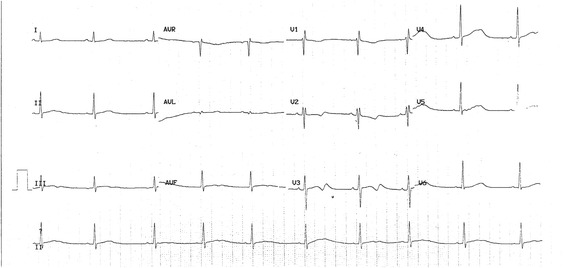
**[[File:ECG in long QT syndrome.jpg|alt=long Qt syndrome|thumb|A boy with a heart rate at 58/min, QT 498 ms and QTc 490 ms in long Qt syndrome. Case courtesy by Thomas Hof Et Al<ref>{{Cite web|url=https://www.ncbi.nlm.nih.|title=TRPM4 non-selective cation channel variants in long QT syndrome|last=|first=|date=|website=|archive-url=|archive-date=|dead-url=|access-date=}}</ref>]]Prolongation of the [[QTc interval]] with an average [[QT interval|QTc]] of 580 ms in classic Timothy syndrome
**Prolongation of the [[QTc interval]] with an average [[QT interval|QTc]] of 640 ms in atypical Timothy syndrome
**Prolongation of the [[QTc interval]] with an average [[QT interval|QTc]] of 640 ms in atypical Timothy syndrome
**[[File:Syndactyly in Timothy syndrome (TS) .gif|alt=syndactyly|thumb|Bilateral cutaneous syndactyly of the third, fourth, and fifth fingers. Case courtesy by Hyo Soon An Et Al<ref>{{Cite web|url=https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3653096/?report=classic|title=Sudden Cardiac Arrest during Anesthesia in a 30-Month-Old Boy with Syndactyly: A Case of Genetically Proven Timothy Syndrome|last=|first=|date=|website=|archive-url=|archive-date=|dead-url=|access-date=}}</ref>]][[Ventricular fibrillation]]
**[[File:Syndactyly in Timothy syndrome (TS) .gif|alt=syndactyly|thumb|Bilateral cutaneous syndactyly of the third, fourth, and fifth fingers. Case courtesy by Hyo Soon An Et Al<ref>{{Cite web|url=https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3653096/?report=classic|title=Sudden Cardiac Arrest during Anesthesia in a 30-Month-Old Boy with Syndactyly: A Case of Genetically Proven Timothy Syndrome|last=|first=|date=|website=|archive-url=|archive-date=|dead-url=|access-date=}}</ref>]][[Ventricular fibrillation]]
== Physical Examination ==
== Physical Examination ==
Physical examination of patients with [disease name] is usually normal. OR Physical examination of patients with [disease name] is usually remarkable for [finding 1], [finding 2], and [finding 3]. OR The presence of [finding(s)] on physical examination is diagnostic of [disease name]. OR The presence of [finding(s)] on physical examination is highly suggestive of [disease name].
[[File:Phenotypic features of Timothy syndrome.gif|thumb|Characteristic phenotypic features of Timothy syndrome: bald head and lower–set ears, webbing of fingers and toes. Case courtesy by U. Krause Et Al<ref>{{Cite web|url=https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3222804/|title=A rare association of long QT syndrome and syndactyly: Timothy Syndrome (LQT 8)|last=|first=|date=|website=|archive-url=|archive-date=|dead-url=|access-date=}}</ref>]]
=== Appearance of the Patient ===
* Patients with [disease name] usually appear [general appearance].
=== Vital Signs ===
* High-grade / low-grade fever
* [[Hypothermia]] / hyperthermia may be present
* [[Tachycardia]] with regular pulse or (ir)regularly irregular pulse
* [[Bradycardia]] with regular pulse or (ir)regularly irregular pulse
* Tachypnea / bradypnea
* Kussmal respirations may be present in _____ (advanced disease state)
* High/low blood pressure with normal pulse pressure / [[wide pulse pressure]] / [[narrow pulse pressure]]
=== Skin ===
* Skin examination of patients with [disease name] is usually normal.
OR
* [[Cyanosis]]
* [[Jaundice]]
* [[Pallor]]
* Bruises
* UploadedImage-01.jpg Description (Adapted from Dermatology Atlas)
* Description (Adapted from Dermatology Atlas)
=== HEENT ===
=== HEENT ===
* HEENT examination of patients with Timothy syndrome is usually shows characteristic [[facial]] features such as:<ref name="pmid20301577">{{cite journal| author=Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K et al.| title=GeneReviews® | journal= | year= 1993 | volume= | issue= | pages= | pmid=20301577 | doi= | pmc= | url= }}</ref>
* HEENT examination of patients with Timothy syndrome is usually shows characteristic [[facial|Craniofacial]] features such as:<ref name="pmid282119892">{{cite journal| author=Sepp R, Hategan L, Bácsi A, Cseklye J, Környei L, Borbás J et al.| title=Timothy syndrome 1 genotype without syndactyly and major extracardiac manifestations. | journal=Am J Med Genet A | year= 2017 | volume= 173 | issue= 3 | pages= 784-789 | pmid=28211989 | doi=10.1002/ajmg.a.38084 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=28211989 }}</ref><ref name="pmid20301577">{{cite journal| author=Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K et al.| title=GeneReviews® | journal= | year= 1993 | volume= | issue= | pages= | pmid=20301577 | doi= | pmc= | url= }}</ref>
**Bald head
**Depressed [[nasal bridge]]
**Depressed [[nasal bridge]]
**Premaxillary underdevelopment
**[[Low-set ears]]
**[[Low-set ears]]
**Thin vermilion border of the upper [[lip]]
**Thin vermilion border of the upper [[lip]]
**Round [[face]]
**Round [[face]]
**Poor [[dental]] [[enamel]] with widely spaced [[teeth]]
OR
* Abnormalities of the head/hair may include ___
* Evidence of trauma
* Icteric sclera
* [[Nystagmus]]
* Extra-ocular movements may be abnormal
* Pupils non-reactive to light / non-reactive to accommodation / non-reactive to neither light nor accommodation
* Ophthalmoscopic exam may be abnormal with findings of ___
* Hearing acuity may be reduced
* [[Weber test]] may be abnormal (Note: A positive Weber test is considered a normal finding / A negative Weber test is considered an abnormal finding. To avoid confusion, you may write "abnormal Weber test".)
* [[Rinne test]] may be positive (Note: A positive Rinne test is considered a normal finding / A negative Rinne test is considered an abnormal finding. To avoid confusion, you may write "abnormal Rinne test".)
* [[Exudate]] from the ear canal
* Tenderness upon palpation of the ear pinnae/tragus (anterior to ear canal)
* A high/low grade early/late [[systolic murmur]] / [[diastolic murmur]] best heard at the base/apex/(specific valve region) may be heard using the bell/diaphgram of the stethoscope
=== Abdomen ===
=== Extremities ===
* Abdominal examination of patients with [disease name] is usually normal.
OR
* [[Abdominal distension]]
* [[Abdominal tenderness]] in the right/left upper/lower abdominal quadrant
* [[Rebound tenderness]] (positive Blumberg sign)
* A palpable abdominal mass in the right/left upper/lower abdominal quadrant
* Genitourinary examination of patients with [disease name] is usually normal.
* Ultrasound may be helpful in the diagnosis of syndactyly during pregnancy with Timothy syndrome patients.
OR
== X Ray, CT scan and MRI scan ==
* A pelvic/adnexal mass may be palpated
* There are no [[X-rays|x-ray]], [[Computed tomography|CT scan]] and [[Magnetic resonance imaging|MRI scan]] findings associated with Timothy syndrome.
* Neuromuscular examination of patients with [disease name] is usually normal.
*[[Verapamil]], [[mexiletine]] and [[ranolazine]] are also effective in treating the patients of Timothy syndrome.<ref name="JacobsKnight2006">{{cite journal|last1=Jacobs|first1=Avrum|last2=Knight|first2=Bradley P.|last3=McDonald|first3=Karen T.|last4=Burke|first4=Martin C.|title=Verapamil decreases ventricular tachyarrhythmias in a patient with Timothy syndrome (LQT8)|journal=Heart Rhythm|volume=3|issue=8|year=2006|pages=967–970|issn=15475271|doi=10.1016/j.hrthm.2006.04.024}}</ref><ref name="pmid20883512">{{cite journal| author=Shah DP, Baez-Escudero JL, Weisberg IL, Beshai JF, Burke MC| title=Ranolazine safely decreases ventricular and atrial fibrillation in Timothy syndrome (LQT8). | journal=Pacing Clin Electrophysiol | year= 2012 | volume= 35 | issue= 3 | pages= e62-4 | pmid=20883512 | doi=10.1111/j.1540-8159.2010.02913.x | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=20883512 }}</ref><ref name="pmid23580742">{{cite journal| author=Gao Y, Xue X, Hu D, Liu W, Yuan Y, Sun H et al.| title=Inhibition of late sodium current by mexiletine: a novel pharmotherapeutical approach in timothy syndrome. | journal=Circ Arrhythm Electrophysiol | year= 2013 | volume= 6 | issue= 3 | pages= 614-22 | pmid=23580742 | doi=10.1161/CIRCEP.113.000092 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=23580742 }}</ref><ref name="pmid282119896">{{cite journal| author=Sepp R, Hategan L, Bácsi A, Cseklye J, Környei L, Borbás J et al.| title=Timothy syndrome 1 genotype without syndactyly and major extracardiac manifestations. | journal=Am J Med Genet A | year= 2017 | volume= 173 | issue= 3 | pages= 784-789 | pmid=28211989 | doi=10.1002/ajmg.a.38084 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=28211989 }}</ref><ref name="pmid235807422">{{cite journal| author=Gao Y, Xue X, Hu D, Liu W, Yuan Y, Sun H et al.| title=Inhibition of late sodium current by mexiletine: a novel pharmotherapeutical approach in timothy syndrome. | journal=Circ Arrhythm Electrophysiol | year= 2013 | volume= 6 | issue= 3 | pages= 614-22 | pmid=23580742 | doi=10.1161/CIRCEP.113.000092 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=23580742 }}</ref>
*[[Beta blockers|Beta-blockers]] helps in controlling the [[QT interval]] prolongation which in-turn helps in preventing [[ventricular tachycardia]], which is the main cause of death in patients with Timothy syndrome.
OR
*In [[Patient|patients]] with Timothy syndrome despite treated with the [[Beta blockers|beta-blockers]] risk of [[cardiac]] events still persists.<ref name="pmid19118258">{{cite journal| author=Vincent GM, Schwartz PJ, Denjoy I, Swan H, Bithell C, Spazzolini C et al.| title=High efficacy of beta-blockers in long-QT syndrome type 1: contribution of noncompliance and QT-prolonging drugs to the occurrence of beta-blocker treatment "failures". | journal=Circulation | year= 2009 | volume= 119 | issue= 2 | pages= 215-21 | pmid=19118258 | doi=10.1161/CIRCULATIONAHA.108.772533 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=19118258 }}</ref>
**Preferred regimen (1): [[Nadolol]] 1–1.5 mg/kg/day administered once a day in patients ≥12 years of age, divided twice daily in [[Infant|infants]] and [[children]]
* Patient is usually oriented to persons, place, and time
**Preferred regimen (2): [[Verapamil]] 120 mg twice a day and by decreasing the [[beta blocker]] dosage to half.
* Pitting/non-pitting [[edema]] of the upper/lower extremities
* Muscle atrophy
* Fasciculations in the upper/lower extremity
**
* [[Implantable cardioverter defibrillator|ICDs]] are single most effective method for preventing sudden death in patients with Timothy syndrome.<ref name="pmid258824682">{{cite journal| author=Corona-Rivera JR, Barrios-Prieto E, Nieto-García R, Bloise R, Priori S, Napolitano C et al.| title=Unusual retrospective prenatal findings in a male newborn with Timothy syndrome type 1. | journal=Eur J Med Genet | year= 2015 | volume= 58 | issue= 6-7 | pages= 332-5 | pmid=25882468 | doi=10.1016/j.ejmg.2015.04.001 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=25882468 }}</ref><ref name="pmid256914163">{{cite journal| author=Hiippala A, Tallila J, Myllykangas S, Koskenvuo JW, Alastalo TP| title=Expanding the phenotype of Timothy syndrome type 2: an adolescent with ventricular fibrillation but normal development. | journal=Am J Med Genet A | year= 2015 | volume= 167A | issue= 3 | pages= 629-34 | pmid=25691416 | doi=10.1002/ajmg.a.36924 | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=25691416 }}</ref>
* [[Implantable cardioverter defibrillator|ICDs]] are reserved for the patients who undergone [[cardiac arrest]] [[resuscitation]].
*[[Implantable cardioverter defibrillator|ICDs]] are good alternative choice of treatment for the patients who are resistant to [[beta blockers]].
*LCSDs are reserved for the patients who are not compatible with [[Beta blockers|beta blocker]] or [[Implantable cardioverter defibrillator|Implantable cardioverter-defibrillators]] ([[Implantable cardioverter defibrillator|ICDs]]).
'''Pacemaker'''
* In patients with Timothy syndrome placing a [[pacemaker]] is going to help in controlling the 2:1 [[AV block]] and [[bradycardia]].
== Surgery ==
===Signs and symptoms===
* Surgery is not the first-line treatment option for patients with Timothy syndrome. Surgery is usually reserved for patients with either:
The most striking sign of Timothy syndrome is the co-occurrence of both [[syndactyly]] (~0.03% of births) and [[long QT syndrome]] (1% per year) in a single patient. Other common symptoms of Timothy syndrome are cardiac [[arrhythmia]] (94%), heart malformations (59%), [[autism]] or an autism spectrum disorder (80% who survive long enough for evaluation). Facial dysmorphologies such as flattened noses also occur in approximately half of patients. Children with this disorder have small teeth which, due to poor [[Tooth enamel|enamel]] coating, are prone to [[dental cavities]] and often require removal. The average age of death due to complications of these symptoms is 2.5 years.<ref name="Marks_1995a">{{cite journal | author = Marks M, Whisler S, Clericuzio C, Keating M | title = A new form of long QT syndrome associated with syndactyly. | journal = J Am Coll Cardiol | volume = 25 | issue = 1 | pages = 59-64 | year = 1995 | id = PMID 7798527}}</ref><ref name="Marks_1995b">{{cite journal | author = Marks M, Trippel D, Keating M | title = Long QT syndrome associated with syndactyly identified in females. | journal = Am J Cardiol | volume = 76 | issue = 10 | pages = 744-5 | year = 1995 | id = PMID 7572644}}</ref><ref name="Splawski_2004">{{cite journal | author = Splawski I, Timothy K, Sharpe L, Decher N, Kumar P, Bloise R, Napolitano C, Schwartz P, Joseph R, Condouris K, Tager-Flusberg H, Priori S, Sanguinetti M, Keating M | title = Ca(V)1.2 calcium channel dysfunction causes a multisystem disorder including arrhythmia and autism. | journal = Cell | volume = 119 | issue = 1 | pages = 19-31 | year = 2004 | id = PMID 15454078}}</ref>
Atypical Timothy syndrome has largely the same symptoms as the classical form. Differences in the atypical form are the lack of syndactyly, the presence of musculoskeletal problems (particularly hyperflexible joints), and [[atrial fibrillation]]s. Patients with atypical Timothy syndrome also have more facial deformities, including protruding foreheads and tongues. Finally, one patient with atypical Timothy syndrome had body development discrepancy wherein her upper body was normally developed (that of a 6-year-old) while her lower half resembled a 2 or 3-year-old.<ref name="Splawski_2005">{{cite journal | author = Splawski I, Timothy K, Decher N, Kumar P, Sachse F, Beggs A, Sanguinetti M, Keating M | title = Severe arrhythmia disorder caused by cardiac L-type calcium channel mutations. | journal = Proc Natl Acad Sci U S A | volume = 102 | issue = 23 | pages = 8089-96; discussion 8086-8 | year = 2005 | id = PMID 15863612}}</ref>
== Primary Prevention ==
Interestingly, children with Timothy syndrome tend to be born via [[cesarean section]] due to fetal distress.
*There are no established measures for the [[primary prevention]] of Timothy syndrome.
===Physical Examination===
==Secondary Prevention==
====Extremities====
Syndactyly and other deformities are typically observed and diagnosed at birth.
===Electrocardiogram===
*Effective measures for the [[secondary prevention]] of Timothy syndrome include:<ref name="pmid203015793">{{cite journal| author=Adam MP, Ardinger HH, Pagon RA, Wallace SE, Bean LJH, Stephens K et al.| title=GeneReviews® | journal= | year= 1993 | volume= | issue= | pages= | pmid=20301579 | doi= | pmc= | url= }}</ref>
Long QT syndrome sometimes presents itself as a complication due to surgery to correct syndactyly. Other times, children collapse spontaneously while playing. In all cases, it is confirmed with [[ECG]] measurements. The sequencing of the [[CACNA1C]] gene further confirms the diagnosis.
**Taking special care while giving the [[anesthesia]] due to the risk of [[cardiac]] [[arrhythmias]].
**Monitoring of serum [[glucose]] levels due to intractable [[hypoglycemia]] in patients with Timothy syndrome.
==Treatment==
Surgery is typically used to correct structural heart defects and syndactyly. [[Propanolol]] or [[beta adrenergic receptor|beta-adrenergic blocker]]s are often prescribed as well as insertion of a [[artificial pacemaker|pacemaker]] to maintain proper heart rhythm. With the characterization of Timothy syndrome mutations indicating that they cause defects in [[calcium]] currents, it has been suggested that [[calcium channel]] blockers may be effective as a therapeutic agent.<ref name="Splawski_2005" />
Synonyms and keywords: Long QT syndrome 8; LQT8; Long QT syndrome with syndactyly; TS
Overview
Timothy syndrome is a rare syndrome that follows autosomal dominant inheritance pattern. Timothy syndrome is a multisystem disorder characterized by physiological and developmental defects which include long QT-prolongation, arrhythmias, structural heart defects, syndactyly and autismspectrum disorders. Timothy syndrome may be classified into 2 groups, classical form(type-1) and atypical form(type-2). Timothy syndrome caused by mutations in CACNA1C, which encodes for calcium channel α subunit. Timothy syndrome often ends in early death. The United States of America in order to categorize a condition as a rare disease it should affect fewer than 200,000 people. Rare diseases also called as orphan diseases. Orphan Drug Act was passed in 1983 by congress for the rare diseases. Today an average of 25-30 million Americans have been reported with rare diseases. The number of people with individual rare disease may be less but overall the number of people with rare diseases are large in number.
Historical Perspective
Timothy syndrome was first discovered by Reichenbach and Marks, in 1992.[1][2]
In 1995, Splawski, Reichenbach, and Marks were the first to give the name Timothy syndrome in the honor of Dr.Katherine W. Timothy who did the phenotypic analysis.[3]
Classification
Timothy syndrome may be classified into 2 groups as follows:[4][5][6][7]
There is one more mutation in G406R that is associated with the timothy syndrome.[14][15]
The location of G406R is in domain one segment six (D1S6) which holds glycine at this position and plays a very important role in voltage-dependent inactivation.
Due to the fact that exon 8(atypical Timothy syndrome) is more expressed in heart muscles than that of exon 8a(classic Timothy syndrome) patients with exon 8 mutation have a severe form of long QT interval.
Trimonth syndrome ECG after birth showed a prolonged QT interval (QTc 600 ms), 2:1 atrioventricular block and significant bradycardia (ventricular rate 60/min). Case courtesy by U. Krause Et Al[35]An ECG is helpful in the diagnosis of Timothy syndrome. Findings on an ECGdiagnostic of Timothy syndrome include the following:[36][1][37][38]
A boy with a heart rate at 58/min, QT 498 ms and QTc 490 ms in long Qt syndrome. Case courtesy by Thomas Hof Et Al[39]Prolongation of the QTc interval with an average QTc of 580 ms in classic Timothy syndrome
Prolongation of the QTc interval with an average QTc of 640 ms in atypical Timothy syndrome
Bilateral cutaneous syndactyly of the third, fourth, and fifth fingers. Case courtesy by Hyo Soon An Et Al[41]Ventricular fibrillation
Physical Examination
Characteristic phenotypic features of Timothy syndrome: bald head and lower–set ears, webbing of fingers and toes. Case courtesy by U. Krause Et Al[42]
HEENT
HEENT examination of patients with Timothy syndrome is usually shows characteristic Craniofacial features such as:[43][44]
Beta-blockers helps in controlling the QT interval prolongation which in-turn helps in preventing ventricular tachycardia, which is the main cause of death in patients with Timothy syndrome.
↑ 28.028.1Splawski I, Timothy K, Sharpe L, Decher N, Kumar P, Bloise R, Napolitano C, Schwartz P, Joseph R, Condouris K, Tager-Flusberg H, Priori S, Sanguinetti M, Keating M (2004). "Ca(V)1.2 calcium channel dysfunction causes a multisystem disorder including arrhythmia and autism". Cell. 119 (1): 19–31. PMID 15454078.CS1 maint: Multiple names: authors list (link)
↑ 29.029.1Splawski I, Timothy K, Decher N, Kumar P, Sachse F, Beggs A, Sanguinetti M, Keating M (2005). "Severe arrhythmia disorder caused by cardiac L-type calcium channel mutations". Proc Natl Acad Sci U S A. 102 (23): 8089–96, discussion 8086-8. PMID 15863612.CS1 maint: Multiple names: authors list (link)
↑Marks M, Whisler S, Clericuzio C, Keating M (1995). "A new form of long QT syndrome associated with syndactyly". J Am Coll Cardiol. 25 (1): 59–64. PMID 7798527.CS1 maint: Multiple names: authors list (link)
↑Marks M, Trippel D, Keating M (1995). "Long QT syndrome associated with syndactyly identified in females". Am J Cardiol. 76 (10): 744–5. PMID 7572644.CS1 maint: Multiple names: authors list (link)
↑Jacobs, Avrum; Knight, Bradley P.; McDonald, Karen T.; Burke, Martin C. (2006). "Verapamil decreases ventricular tachyarrhythmias in a patient with Timothy syndrome (LQT8)". Heart Rhythm. 3 (8): 967–970. doi:10.1016/j.hrthm.2006.04.024. ISSN1547-5271.
.jpg)

_.gif)
