Aortic stenosis gross pathology: Difference between revisions
Varun Kumar (talk | contribs) (New page: {{SI}} {{CMG}} {{EH}} ==Pathological Findings== Images shown below are courtesy of Professor Peter Anderson DVM PhD and published with permission. [http://www.peir.net © PEIR, Univers...) |
Aysha Aslam (talk | contribs) No edit summary |
||
| (18 intermediate revisions by 8 users not shown) | |||
| Line 1: | Line 1: | ||
{{ | {{Aortic stenosis}} | ||
{{CMG}}; '''Associate Editors-In-Chief:''' Claudia P. Hochberg, M.D. [mailto:chochber@bidmc.harvard.edu], [[User:Abdarabi|Abdul-Rahman Arabi, M.D.]] [mailto:abdarabi@yahoo.com], [[User:KeriShafer|Keri Shafer, M.D.]] [mailto:kshafer@bidmc.harvard.edu], [[Priyamvada Singh|Priyamvada Singh, MBBS]] [mailto:psingh13579@gmail.com], {{AA}}; '''Assistant Editor-In-Chief:''' [[Kristin Feeney|Kristin Feeney, B.S.]] [mailto:kfeeney@elon.edu] | |||
{{CMG}} | |||
{{ | |||
==Overview== | |||
Gross anatomy dissection may be used as a diagnostic tool in the evaluation of aortic stenosis. Common findings associated with aortic stenosis include [[left ventricular hypertrophy]] and [[heart block]]. | |||
==Pathological Findings== | ==Pathological Findings== | ||
Pathological findings of congenital or acquired aortic stenosis in adults results in thickening and calcification of aortic valve. Following patterns may be seen:<ref name="pmid3402479">{{cite journal| author=Normand J, Loire R, Zambartas C| title=The anatomical aspects of adult aortic stenosis. | journal=Eur Heart J | year= 1988 | volume= 9 Suppl E | issue= | pages= 31-6 | pmid=3402479 | doi= | pmc= | url=https://www.ncbi.nlm.nih.gov/entrez/eutils/elink.fcgi?dbfrom=pubmed&tool=sumsearch.org/cite&retmode=ref&cmd=prlinks&id=3402479 }} </ref> | |||
*Calcified bicuspid valve involving anterior or posterior cusps | |||
*Calcified aortic valve cusps with fusion of commissures seen in post rheumatic cases | |||
*Degenerative calcific aortic stenosis which shows sinuses of valsalva filled with calcium deposits seen in age >70 | |||
Images shown below are courtesy of Professor Peter Anderson DVM PhD and published with permission. [http://www.peir.net © PEIR, University of Alabama at Birmingham, Department of Pathology] | Images shown below are courtesy of Professor Peter Anderson DVM PhD and published with permission. [http://www.peir.net © PEIR, University of Alabama at Birmingham, Department of Pathology] | ||
<gallery> | |||
<gallery | |||
Image:Bicuspid aortic valve1.jpg|Aortic Stenosis, Bicuspid valve: Gross; excellent image of bicuspid and calcific valve showing a false raphe. | Image:Bicuspid aortic valve1.jpg|Aortic Stenosis, Bicuspid valve: Gross; excellent image of bicuspid and calcific valve showing a false raphe. | ||
Image:Bicuspid aortic valve2.jpg|Aortic Stenosis, Bicuspid valve: Gross; good example of bicuspid valve | Image:Bicuspid aortic valve2.jpg|Aortic Stenosis, Bicuspid valve: Gross; good example of bicuspid valve | ||
Image:Bicuspid aortic valve3.jpg|Aortic Stenosis, Bicuspid valve: Gross; image of bicuspid aortic valve, an excellent example | Image:Bicuspid aortic valve3.jpg|Aortic Stenosis, Bicuspid valve: Gross; image of bicuspid aortic valve, an excellent example | ||
Image:Bicuspid aortic valve4.jpg|Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve. | Image:Bicuspid aortic valve4.jpg|Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve. | ||
Image:Bicuspid aortic valve5.jpg|Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve. | Image:Bicuspid aortic valve5.jpg|Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve. | ||
Image:Bicuspid aortic valve6.jpg|Bicuspid aortic valve | Image:Bicuspid aortic valve6.jpg|Bicuspid aortic valve | ||
Image:Bicuspid aortic valve7.jpg|Gross natural color opened first portion aortic arch with bicuspid aortic valve shows stenosis and aortic root is dilated | Image:Bicuspid aortic valve7.jpg|Gross natural color opened first portion aortic arch with bicuspid aortic valve shows stenosis and aortic root is dilated | ||
Image:Bicuspid aortic valve8.jpg|Aortic Stenosis Bicuspid: Gross; natural color opened left ventricular outflow tract with calcific masses on valve as well as anterior leaflet mitral valve probably did not cause significant stenosis | Image:Bicuspid aortic valve8.jpg|Aortic Stenosis Bicuspid: Gross; natural color opened left ventricular outflow tract with calcific masses on valve as well as anterior leaflet mitral valve probably did not cause significant stenosis | ||
Image:Bicuspid aortic valve9.jpg|Bicuspid Aortic Valve with Repaired Aorta Coarctation: Gross natural color opened left ventricular outflow tract with uncomplicated bicuspid aortic valve repaired coarctation barely visible ruptured postoperative young female with ovaries Turner mosaic not ruled out | Image:Bicuspid aortic valve9.jpg|Bicuspid Aortic Valve with Repaired Aorta Coarctation: Gross natural color opened left ventricular outflow tract with uncomplicated bicuspid aortic valve repaired coarctation barely visible ruptured postoperative young female with ovaries Turner mosaic not ruled out | ||
Image:Bicuspid aortic valve10.jpg|Bicuspid Aortic Stenosis: Gross; fixed tissue | Image:Bicuspid aortic valve10.jpg|Bicuspid Aortic Stenosis: Gross; fixed tissue | ||
Image:Bicuspid aortic valve11.jpg|Aortic Stenosis, Bicuspid: Gross; fixed tissue view of stenotic valve through ventricular outlet track | Image:Bicuspid aortic valve11.jpg|Aortic Stenosis, Bicuspid: Gross; fixed tissue view of stenotic valve through ventricular outlet track | ||
Image:Bicuspid aortic valve12.jpg|Aortic Stenosis Bicuspid: Gross; fixed tissue. Bicuspid valve and false raphe classical | Image:Bicuspid aortic valve12.jpg|Aortic Stenosis Bicuspid: Gross; fixed tissue. Bicuspid valve and false raphe classical | ||
Image:Bicuspid aortic valve13.jpg|Bicuspid aortic valve | Image:Bicuspid aortic valve13.jpg|Bicuspid aortic valve | ||
Image:Bicuspid aortic valve14.jpg|Bicuspid aortic valve | Image:Bicuspid aortic valve14.jpg|Bicuspid aortic valve | ||
Image:Bicuspid aortic valve15.jpg|Bicuspid aortic valve | Image:Bicuspid aortic valve15.jpg|Bicuspid aortic valve | ||
Image:Bicuspid aortic valve16.jpg|Left ventricular hypertrophy due to bicuspid aortic valve | Image:Bicuspid aortic valve16.jpg|Left ventricular hypertrophy due to bicuspid aortic valve | ||
Image:Congenital aortic stenosis.jpg|Congenital aortic stenosis: Gangrene toe In Infant: Gross, natural color, 1 month old child with congenital aortic stenosis | Image:Congenital aortic stenosis.jpg|Congenital aortic stenosis: Gangrene toe In Infant: Gross, natural color, 1 month old child with congenital aortic stenosis | ||
Image:Unicuspid aortic stenosis.jpg|Unicuspid aortic stenosis | Image:Unicuspid aortic stenosis.jpg|Unicuspid aortic stenosis | ||
</gallery> | </gallery> | ||
==References== | ==References== | ||
{{reflist|2}} | {{reflist|2}} | ||
[[es:Estenosis aórtica]] | |||
[[fr:Rétrécissement aortique]] | |||
[[pl:Stenoza Aortalnej]] | |||
[[pt:Estenose aórtica]] | |||
[[ro:Stenoza Aortică]] | |||
[[tr:Aort darlığı]] | |||
[[Category: Cardiology]] | {{WH}} | ||
{{WS}} | |||
[[CME Category::Cardiology]] | |||
[[Category:Disease]] | |||
[[Category:Valvular heart disease]] | |||
[[Category:Cardiology]] | |||
[[Category:Congenital heart disease]] | |||
[[Category:Mature chapter]] | |||
[[Category:Cardiac surgery]] | |||
[[Category:Surgery]] | |||
[[Category:Overview complete]] | |||
[[Category:Template complete]] | |||
Latest revision as of 20:44, 23 December 2016
|
Aortic Stenosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Percutaneous Aortic Balloon Valvotomy (PABV) or Aortic Valvuloplasty |
|
Transcatheter Aortic Valve Replacement (TAVR) |
|
Case Studies |
|
Aortic stenosis gross pathology On the Web |
|
American Roentgen Ray Society Images of Aortic stenosis gross pathology |
|
Directions to Hospitals Treating Aortic stenosis gross pathology |
|
Risk calculators and risk factors for Aortic stenosis gross pathology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editors-In-Chief: Claudia P. Hochberg, M.D. [2], Abdul-Rahman Arabi, M.D. [3], Keri Shafer, M.D. [4], Priyamvada Singh, MBBS [5], Aysha Anwar, M.B.B.S[6]; Assistant Editor-In-Chief: Kristin Feeney, B.S. [7]
Overview
Gross anatomy dissection may be used as a diagnostic tool in the evaluation of aortic stenosis. Common findings associated with aortic stenosis include left ventricular hypertrophy and heart block.
Pathological Findings
Pathological findings of congenital or acquired aortic stenosis in adults results in thickening and calcification of aortic valve. Following patterns may be seen:[1]
- Calcified bicuspid valve involving anterior or posterior cusps
- Calcified aortic valve cusps with fusion of commissures seen in post rheumatic cases
- Degenerative calcific aortic stenosis which shows sinuses of valsalva filled with calcium deposits seen in age >70
Images shown below are courtesy of Professor Peter Anderson DVM PhD and published with permission. © PEIR, University of Alabama at Birmingham, Department of Pathology
-

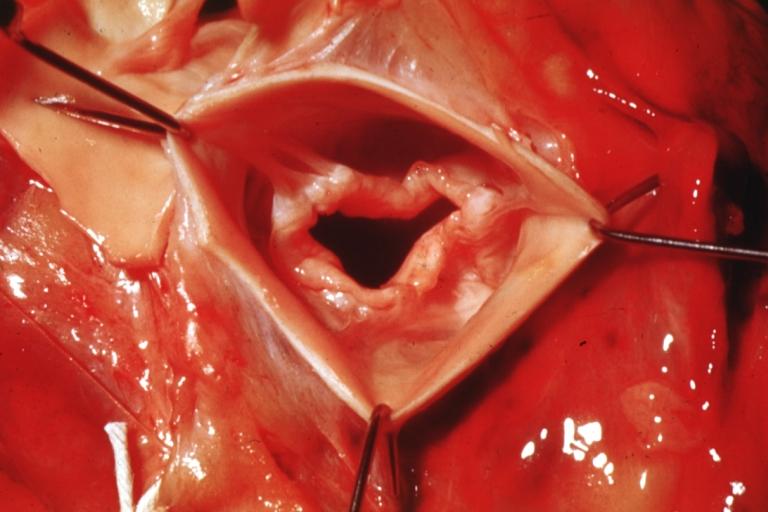
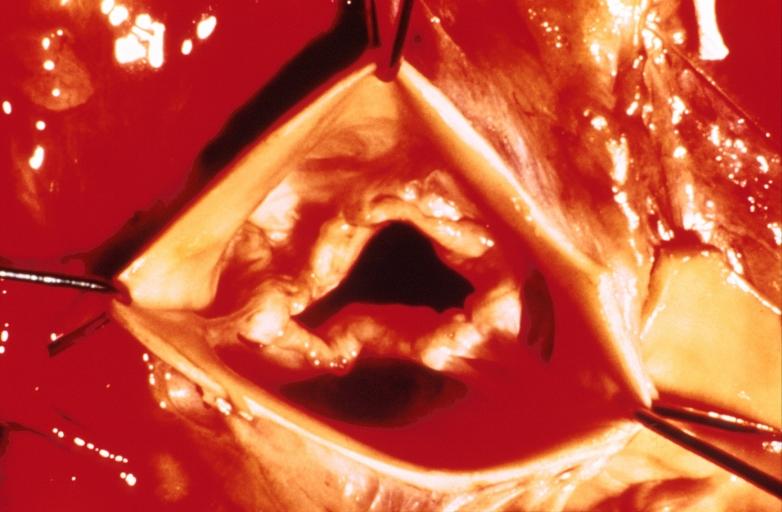
Aortic Stenosis, Bicuspid valve: Gross; excellent image of bicuspid and calcific valve showing a false raphe.
-
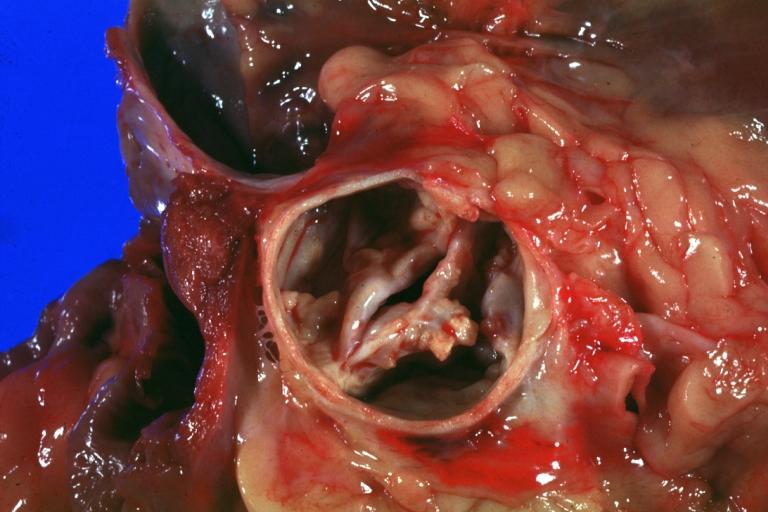
Aortic Stenosis, Bicuspid valve: Gross; good example of bicuspid valve
-
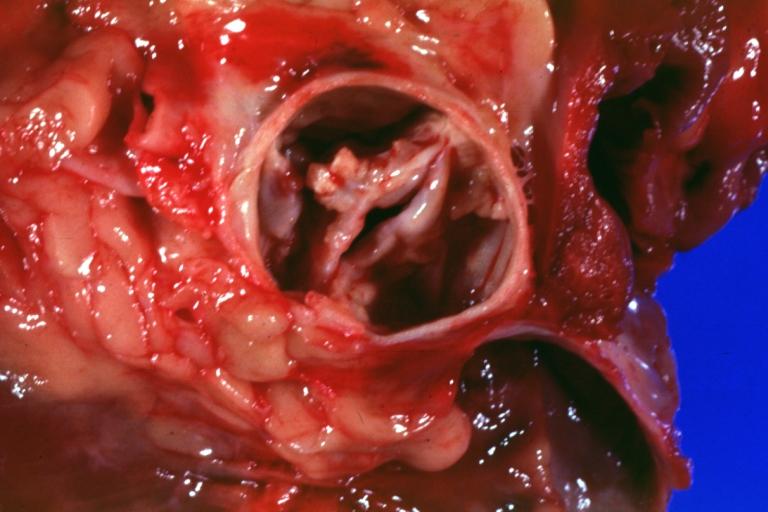
Aortic Stenosis, Bicuspid valve: Gross; image of bicuspid aortic valve, an excellent example
-

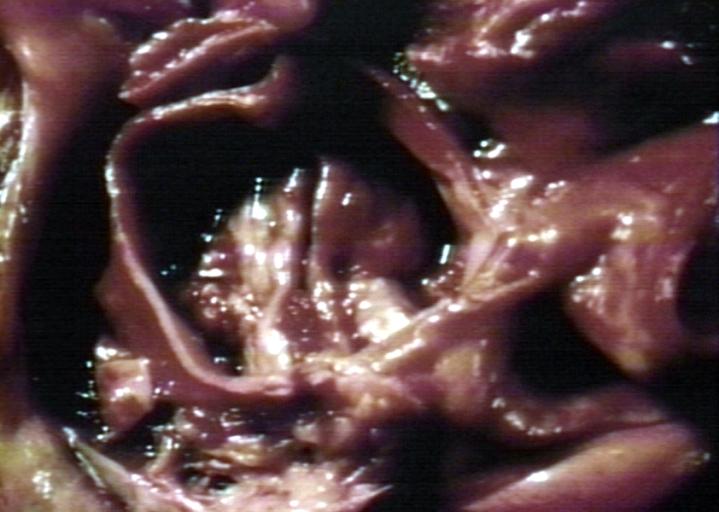
Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve.
-

Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve.
-
Bicuspid aortic valve
-
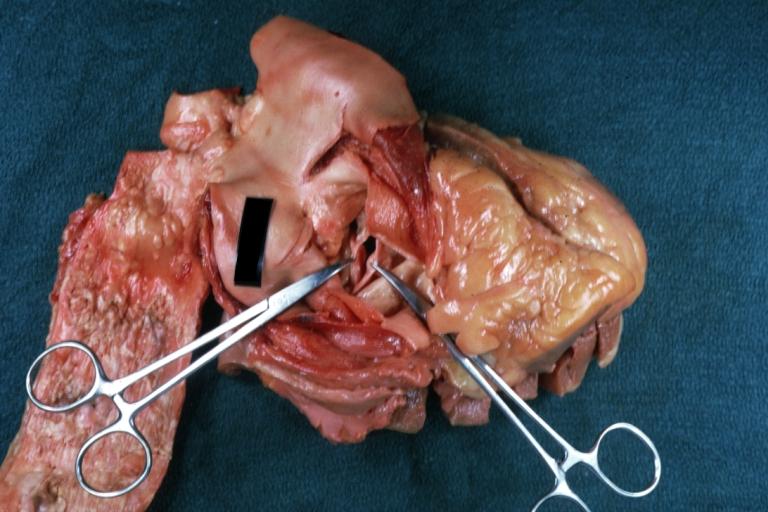
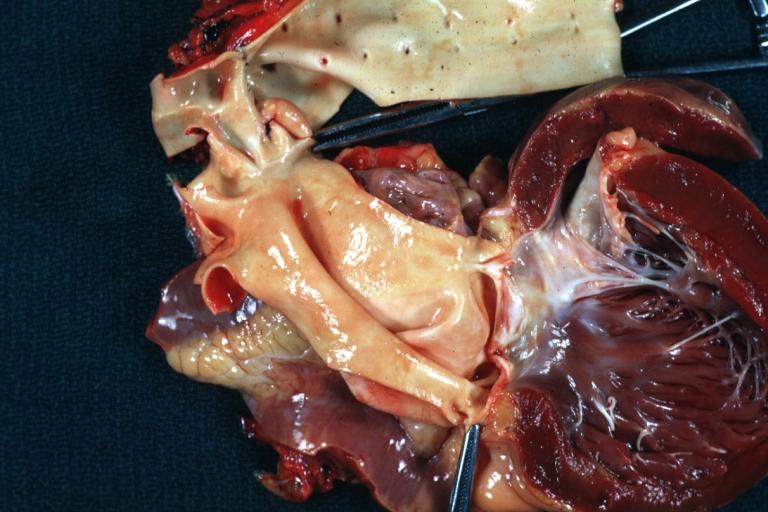
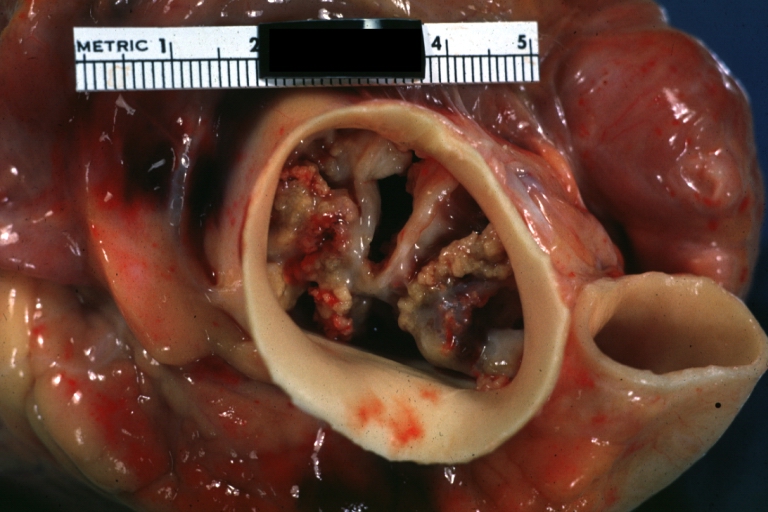
Gross natural color opened first portion aortic arch with bicuspid aortic valve shows stenosis and aortic root is dilated
-
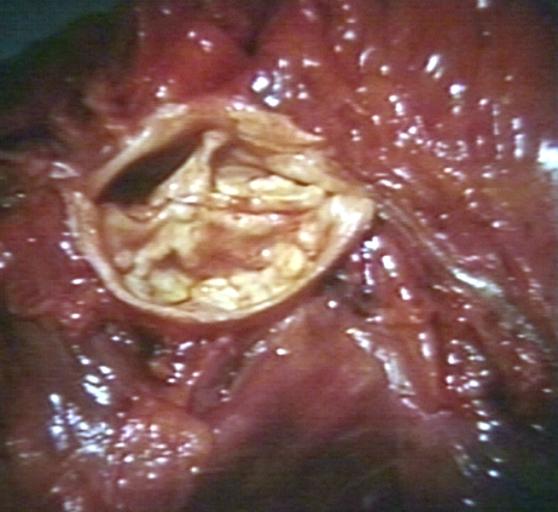
Aortic Stenosis Bicuspid: Gross; natural color opened left ventricular outflow tract with calcific masses on valve as well as anterior leaflet mitral valve probably did not cause significant stenosis
-
Bicuspid Aortic Valve with Repaired Aorta Coarctation: Gross natural color opened left ventricular outflow tract with uncomplicated bicuspid aortic valve repaired coarctation barely visible ruptured postoperative young female with ovaries Turner mosaic not ruled out
-

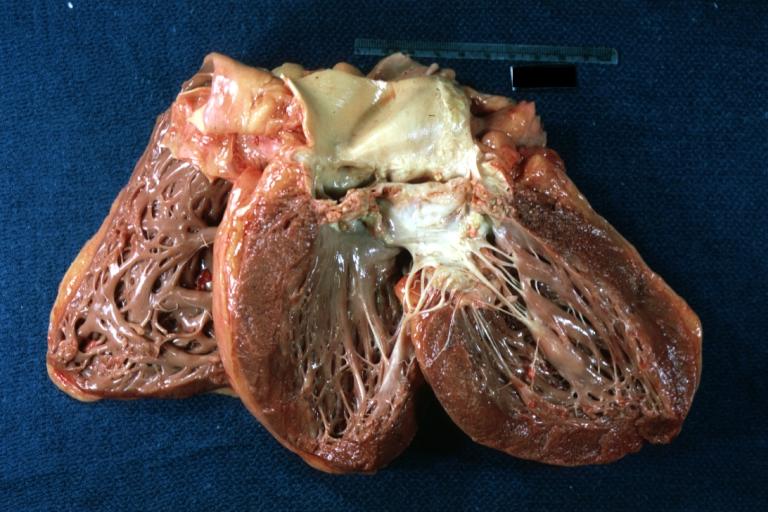
Bicuspid Aortic Stenosis: Gross; fixed tissue
-

Aortic Stenosis, Bicuspid: Gross; fixed tissue view of stenotic valve through ventricular outlet track
-

Aortic Stenosis Bicuspid: Gross; fixed tissue. Bicuspid valve and false raphe classical
-
Bicuspid aortic valve
-
Bicuspid aortic valve
-
Bicuspid aortic valve
-
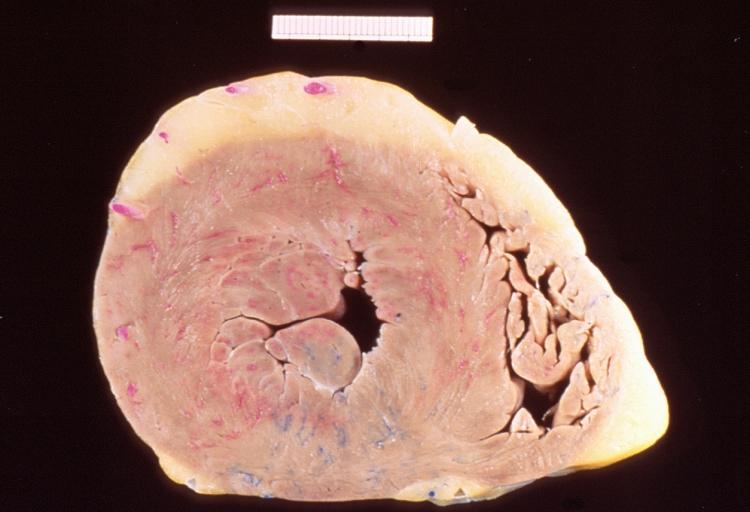
Left ventricular hypertrophy due to bicuspid aortic valve
-

Congenital aortic stenosis: Gangrene toe In Infant: Gross, natural color, 1 month old child with congenital aortic stenosis
-
Unicuspid aortic stenosis


















References
- ↑ Normand J, Loire R, Zambartas C (1988). "The anatomical aspects of adult aortic stenosis". Eur Heart J. 9 Suppl E: 31–6. PMID 3402479.