Narrow complex tachycardia resident survival guide: Difference between revisions
Rim Halaby (talk | contribs) |
Rim Halaby (talk | contribs) |
||
| Line 216: | Line 216: | ||
Shown below is an algorithm summarizing the management of narrow complex tachycardia according to the 2003 ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias.<ref name="circ.ahajournals.org">{{Cite web | last = | first = | title = ACC/AHA/ESC Guidelines for the Management of Patients With Supraventricular Arrhythmias—Executive Summary | url = http://circ.ahajournals.org/content/108/15/1871 | publisher = | date = | accessdate = 15 August 2013 }}</ref> <br> | Shown below is an algorithm summarizing the management of narrow complex tachycardia according to the 2003 ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias.<ref name="circ.ahajournals.org">{{Cite web | last = | first = | title = ACC/AHA/ESC Guidelines for the Management of Patients With Supraventricular Arrhythmias—Executive Summary | url = http://circ.ahajournals.org/content/108/15/1871 | publisher = | date = | accessdate = 15 August 2013 }}</ref> <br> | ||
<span style="font-size:85%">'''Abbreviations:''' '''AF''': atrial fibrillation; '''AV''': atrioventricular; '''AVNRT''': atrioventricular nodal reciprocating tachycardia; '''AVRT''': atrioventricular reciprocating tachycardia; '''BBB''': bundle-branch block; '''ECG''': electrocardiography; ''' IV''': intravenous; '''LV''': left ventricle; '''SVT''': supraventricular tachycardia; '''VT''': ventricular tachycardia </span> | <span style="font-size:85%">'''Abbreviations:''' '''AF''': atrial fibrillation; '''AV''': atrioventricular; '''AVNRT''': atrioventricular nodal reciprocating tachycardia; '''AVRT''': atrioventricular reciprocating tachycardia; '''BBB''': bundle-branch block; '''ECG''': electrocardiography; ''' IV''': intravenous; '''LV''': left ventricle; '''SVT''': supraventricular tachycardia; '''VT''': ventricular tachycardia </span> | ||
{{familytree/start}} | {{familytree/start}} | ||
{{familytree | | | D01 | | | {{familytree | | | A01 | | A01= Assess the hemodynamic status of the patient <br> Signs of hemodynamic instability include: <br> | ||
❑ Hypotension <br> | |||
❑ Acute altered mental status <br> | |||
❑ Signs of shock <br> | |||
❑ Acute heart failure<br> | |||
❑ Chest discomfort suggestive of ischemia<br>}} | |||
{{familytree | |,|-|^|-|.| | }} | |||
{{familytree | B01 | | B02 | B01= Stable | B02= Unstable }} | |||
{{familytree | |!| | | |!| | | | | }} | |||
{{familytree | C01 | | C02 | | | | C01= Synchronized cardioversion| C02= Does the patient have any of the following? <br> [[Atrial fibrillation]] <br> [[Atrial flutter]] <br> [[Wolff Parkinson Wolff syndrome]] (orthodromic AVRT)}} | |||
{{familytree | | | |,|-|^|-|.| | | }} | |||
{{familytree | | | C03 | | C04 | | | C03= No | C04= Yes }} | |||
{{familytree | | | |!| | | |!| | }} | |||
{{familytree | | | D01 | | D02=<div style="float: left; text-align: left; width: 35em; padding:1em;">'''Acute management:'''<br> | |||
❑ Perform vagal maneuvers ([[ACC AHA guidelines classification scheme|Class I, level of evidence B]])<br> | ❑ Perform vagal maneuvers ([[ACC AHA guidelines classification scheme|Class I, level of evidence B]])<br> | ||
: ❑ [[Valsalva maneuver]]<br> | : ❑ [[Valsalva maneuver]]<br> | ||
: ❑ [[Carotid sinus massage]]<br> | : ❑ [[Carotid sinus massage]]<br> | ||
❑ Monitor [[ECG]] continuously</div>}} | ❑ Monitor [[ECG]] continuously</div>| D02=}} | ||
{{familytree | | | |!| | | | |}} | {{familytree | | | |!| | | | |}} | ||
{{familytree | | | D02 | | |D02=<div style="float: left; text-align: left; width: 35em; padding:1em;">'''If vagal maneuvers fail:'''<br> | {{familytree | | | D02 | | | | D02=<div style="float: left; text-align: left; width: 35em; padding:1em;">'''If vagal maneuvers fail:'''<br> | ||
❑ Administer IV [[adenosine]]† ([[ACC AHA guidelines classification scheme|Class I, level of evidence A]])<br> | ❑ Administer IV [[adenosine]]† ([[ACC AHA guidelines classification scheme|Class I, level of evidence A]])<br> | ||
:❑ First dose: 6 mg rapid IV push, followed by 20 mL of [[normal saline]] bolus | :❑ First dose: 6 mg rapid IV push, followed by 20 mL of [[normal saline]] bolus | ||
Revision as of 16:32, 3 April 2014
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Hilda Mahmoudi M.D., M.P.H.[2]; Twinkle Singh, M.B.B.S. [3]; Rim Halaby, M.D. [4]; Amr Marawan, M.D. [5]
Synonyms and keywords: Supraventricular tachycardia, SVT
| Narrow Complex Tachycardia Resident Survival Guide Microchapters |
|---|
| Overview |
| Causes |
| Classification |
| Diagnosis |
| Treatment |
| Do's |
| Don'ts |
Overview
Narrow complex tachycardia (NCT) is characterized by a heart rate > 100 beats per minute and a QRS complex of a duration < 120 milliseconds. NCT may originate in the sinus node, atria, AV node, bundle of His, or a combination of these tissues. The diagnosis of NCT is based on the ECG findings. Hemodynamically unstable patients should receive urgent cardioversion.
Causes
Life Threatening Causes
Life-threatening causes include conditions which may result in death or permanent disability within 24 hours if left untreated.
Common Causes
Classification
- Atrial fibrillation
- Atrial flutter
- Atrial tachycardia
- Atrioventricular reentrant tachycardia (AVRT)
- AV nodal reentrant tachycardia (AVNRT)
- Inappropriate sinus tachycardia
- Intraatrial reentrant tachycardia (IART)
- Junctional tachycardia
- Multifocal atrial tachycardia
- Sinus node re-entry tachycardia
- Sinus tachycardia
Diagnosis
First Initial Rapid Evaluation of Suspected Narrow Complex Tachycardia
Shown below is an algorithm for the First Initial Rapid Evaluation (FIRE) of suspected narrow complex tachycardia.[1][2]
Boxes in red signify that an urgent management is needed.
Identify cardinal signs and symptoms that increase the pretest probability of NCT ❑ Palpitations (Most common presentation)
| |||||||||||||||||||||||||||||||||||||||||||||
Identify alarming signs and symptoms of hemodynamic instability ❑ Hypotension ❑ Acute altered mental status ❑ Signs of shock ❑ Acute heart failure ❑ Chest discomfort suggestive of ischemia | |||||||||||||||||||||||||||||||||||||||||||||
❑ Unstable patient | ❑ Stable patient | ||||||||||||||||||||||||||||||||||||||||||||
❑ Urgent synchronized cardioversion
| |||||||||||||||||||||||||||||||||||||||||||||
Complete Diagnostic Approach to Narrow Complex Tachycardia
Shown below is an algorithm summarizing the diagnostic approach to narrow complex tachycardia according to the 2003 ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias.[1]
Abbreviations: ECG: electrocardiogram; SVT: Supraventricular tachycardia; ms: milliseconds; bpm: beats per minute; NCT: Narrow complex tachycardia; AV: atrioventricular; AVNRT: atrioventricular nodal reciprocating tachycardia; MAT: multifocal atrial tachycardia; ms: milliseconds; PJRT: permanent form of junctional reciprocating tachycardia; RP interval: is the time between anterograde ventricular activation (R wave) and retrograde atrial activation (P wave)
Characterize the symptoms: ❑ Asymptomatic (most common presentation)
❑ Duration
| |||||||||||||||||||||||||||||||||||||||||||||
Identify possible triggers: | |||||||||||||||||||||||||||||||||||||||||||||
Examine the patient:
Neck
Cardiovascular examination
| |||||||||||||||||||||||||||||||||||||||||||||
❑ Order and monitor the ECG | |||||||||||||||||||||||||||||||||||||||||||||
Narrow QRS tachycardia ❑ Heart rate > 100 beats/min ❑ QRS duration < 120 ms | |||||||||||||||||||||||||||||||||||||||||||||
| ❑ Determine regularity of the rhythm | |||||||||||||||||||||||||||||||||||||||||||||
| Regular rhythm | Irregular rhythm | ||||||||||||||||||||||||||||||||||||||||||||
Consider the following causes: ❑ AVRT | Consider the following causes: ❑ Atrial fibrillation | ||||||||||||||||||||||||||||||||||||||||||||
| ❑ Determine P wave morphology | ❑ Determine P wave morphology | ||||||||||||||||||||||||||||||||||||||||||||
❑ P waves are not visible | ❑ P waves are visible | ❑ > 3 P wave morphologies | ❑ Absent P waves | ❑ Sawtooth appearance of P waves | |||||||||||||||||||||||||||||||||||||||||
| ❑ Consider AVNRT | ❑ Determine if atrial rate is greater than ventricular rate | ❑ Consider MAT | ❑ Consider atrial fibrillation | ❑ Consider atrial flutter | |||||||||||||||||||||||||||||||||||||||||
| Atrial rate > ventricular rate | Atrial rate ≤ ventricular rate | ||||||||||||||||||||||||||||||||||||||||||||
| ❑ Determine if RP interval > PR interval | |||||||||||||||||||||||||||||||||||||||||||||
| RP < PR | RP > PR | ||||||||||||||||||||||||||||||||||||||||||||
| ❑ Determine the duration of RP interval | |||||||||||||||||||||||||||||||||||||||||||||
| < 70 ms | > 70 ms | ||||||||||||||||||||||||||||||||||||||||||||
Consider the following cause: ❑ AVNRT | |||||||||||||||||||||||||||||||||||||||||||||
ECG Examples
| Type of Arrhythmia | EKG (lead II)† | Clues |
| Supraventricular tachycardia |  |
Any tachyarrhythmia that is initiated and maintained in atrial tissue or atrioventricular junctional tissue.[1] |
| Sinus tachycardia |  |
Rhythm with heart rate > 100 bpm, originating in SA node due to its increased automaticity. It is regular, non paroxysmal and has a gradual onset and termination. |
| Sinus node re-entry tachycardia | Rare paroxysmal tachycardia arising due to re-entry circuits with in SA node.[3] | |
| Atrial fibrillation | 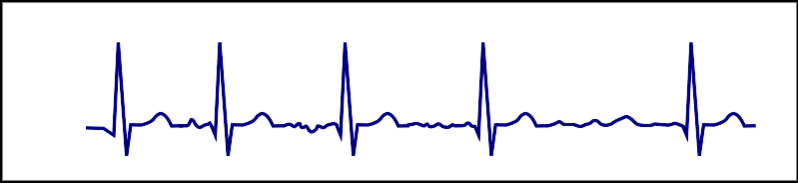 |
Supraventricular tachycardia with irregularly irregular rhythm and absent P waves on EKG. |
| Atrial flutter | 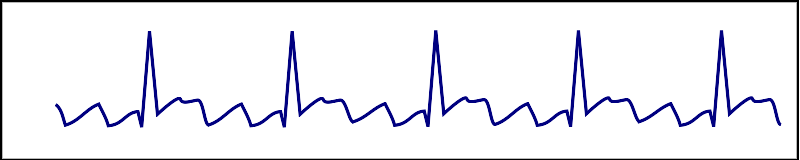 |
Cardiac rhythm characterized by an atrial rate ranging from 240 to 400 beats per minute and regular continuous wave-form.[4] |
| AVNRT | 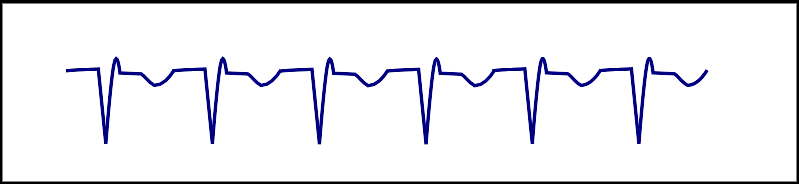 |
Most common form of PSVT with a heart rate of 140-250 bpm, re-entrant circuit involves two separate anatomical pathways (slow and fast) located in perinodal tissue. It is regular and paroxysmal. |
| AVRT |  |
Re-entrant tachycardia occurring due to an accessory pathway in addition to AV node, accessory pathway is essential for the initiation and the maintenance of tachycardia. It is regular and paroxysmal. |
| Focal atrial tachycardia | 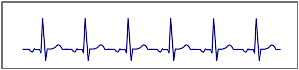 |
Focal atria tachycardia refers to a rhythm originating from a single site either in the left or right atrium with an atrial rate of 100-250 bpm. |
| Nonparoxysmal junctional tachycardia |  |
Benign tachycardia occurring due to increased automaticity arising from a high junctional focus. |
| Multifocal atrial tachycardia | 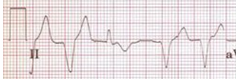 |
Irregular tachycardia characterized by 3 different P wave morphologies on EKG. |
† EKG strips are courtesy of ECGpedia.
Treatment
Treatment of SVT in a Hemodynamically Stable Patient
Shown below is an algorithm summarizing the management of narrow complex tachycardia according to the 2003 ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias.[1]
Abbreviations: AF: atrial fibrillation; AV: atrioventricular; AVNRT: atrioventricular nodal reciprocating tachycardia; AVRT: atrioventricular reciprocating tachycardia; BBB: bundle-branch block; ECG: electrocardiography; IV: intravenous; LV: left ventricle; SVT: supraventricular tachycardia; VT: ventricular tachycardia
| Assess the hemodynamic status of the patient Signs of hemodynamic instability include: ❑ Hypotension | |||||||||||||||||||||||||||
| Stable | Unstable | ||||||||||||||||||||||||||
| Synchronized cardioversion | Does the patient have any of the following? Atrial fibrillation Atrial flutter Wolff Parkinson Wolff syndrome (orthodromic AVRT) | ||||||||||||||||||||||||||
| No | Yes | ||||||||||||||||||||||||||
| {{{ D01 }}} | |||||||||||||||||||||||||||
If vagal maneuvers fail: ❑ Administer IV adenosine† (Class I, level of evidence A)
Adenosine is contraindicated in cardiac transplant patients. Use adenosine with caution in severe obstructive lung disease.[5] ❑ Monitor ECG continuously | |||||||||||||||||||||||||||
If adenosine fails, administer ONE of the following: ❑ IV verapamil 5 mg IV every 3-5 min, maximum 15 mg (Class I, level of evidence A)[5]
❑ IV beta blocker (Class IIb, level of evidence C)
❑ Monitor ECG continuously | |||||||||||||||||||||||||||
| Terminated arrhythmia | Persistent arrhythmia | ||||||||||||||||||||||||||
No further therapy is required if: ❑ Patient is stable ❑ LV function is normal ❑ Normal sinus rhythm on ECG | ❑ Administer AV-nodal-blocking agent AND one of the following
OR | ||||||||||||||||||||||||||
† Adenosine should be used cautiously in patients with severe coronary artery disease and may produce AF.
‡ Ibutilide is especially indicated for patients with atrial flutter but should not be used in patients with ejection fraction less than 30% as it increases risk of polymorphic VT.
Treatment of Specific Supraventricular Arrhythmia
Focal Atrial Tachycardia
Focal and Nonparoxysmal Junctional Tachycardia
| ||||||||
AVNRT
| ||||||||||||||||||||
Inappropriate Sinus Tachycardia
| |||
Do's
- Consider the arrhythmia to be paroxysmal if it is recurrent and abruptly begins and terminates.
- Refer patients with narrow complex tachycardia with any of the following to a cardiac arrhythmia specialist:
- Drug resistance
- Intolerance to drugs
- Refusal of drug therapy
- Severe symptoms such as syncope and dyspnea
- Wolff-Parkinson-White syndrome[5]
- Consider trying different types of anti-arrhythmic agents in case the SVT is refractory; however, closely monitor the blood pressure and heart rate.[5]
- Consider invasive electrophysiological investigation in the presence of pre-excitation and severe disabling symptoms.
- Monitor the 12 lead ECG during the administration ofadenosine or carotid massage.
- Make sure the equipment for resuscitation is available during the administration of adenosine in case of the occurrence of any complication, such as ventricular fibrillation or bronchospasm.[5]
- Consider esophageal pill electrodes in cases of invisible P waves.
- Administer higher doses of adenosine in patients taking theophylline.
- Perform the following tests when indicated:
- Echocardiography in case of sustained SVT to rule out structural heart disease
- 24 hour holter monitor in case of frequent but transient tachycardia
- Loop recorder in patients with less frequent arrhythmia
- Trans-esophageal atrial recordings if other investigations have failed to document an arrhythmia
Don'ts
- Do not perform esophageal stimulation if an invasive electrophysiological investigation is planned.
- Do not initiate treatment with anti-arrhythmic agents in a patient with undocumented arrhythmia.
- Do not administer adenosine in patients with severe bronchial asthma or heart transplant recipients.[5]
References
- ↑ 1.0 1.1 1.2 1.3 "ACC/AHA/ESC Guidelines for the Management of Patients With Supraventricular Arrhythmias—Executive Summary". Retrieved 15 August 2013.
- ↑ "Part 8: Adult Advanced Cardiovascular Life Support". Retrieved 3 April 2014.
- ↑ Cossú, SF.; Steinberg, JS. "Supraventricular tachyarrhythmias involving the sinus node: clinical and electrophysiologic characteristics". Prog Cardiovasc Dis. 41 (1): 51–63. PMID 9717859.
- ↑ Dhar S, Lidhoo P, Koul D, Dhar S, Bakhshi M, Deger FT (2009). "Current concepts and management strategies in atrial flutter". South. Med. J. 102 (9): 917–22. doi:10.1097/SMJ.0b013e3181b0f4b8. PMID 19668035. Unknown parameter
|month=ignored (help) - ↑ 5.0 5.1 5.2 5.3 5.4 5.5 5.6 5.7 5.8 Delacrétaz E (2006). "Clinical practice. Supraventricular tachycardia". N Engl J Med. 354 (10): 1039–51. doi:10.1056/NEJMcp051145. PMID 16525141.