Multiple sclerosis epidemiology and demographics: Difference between revisions
No edit summary |
No edit summary |
||
| Line 7: | Line 7: | ||
== Epidemiology and Demographics== | == Epidemiology and Demographics== | ||
There is a lower frequency of people suffering from Multiple Sclerosis among citizens of the Arabian Peninsula, Asia, and continental South America than people living in northern Europe, continental North America, and Australasia, which is about one of every 1000 citizens. In addition, in sub-Saharan Africa, [[MS]] is extremely rare.<ref>[http://www.fedem.org/revista/n16/kurtzkeing.htm Epidemiology and multiple sclerosis. a personal review]</ref> | There is a lower frequency of people suffering from Multiple Sclerosis among citizens of the Arabian Peninsula, Asia, and continental South America than people living in northern Europe, continental North America, and Australasia, which is about one of every 1000 citizens. In addition, in sub-Saharan Africa, [[MS]] is extremely rare.<ref>[http://www.fedem.org/revista/n16/kurtzkeing.htm Epidemiology and multiple sclerosis. a personal review]</ref> factors including sunlight exposure, climate, [[diet]], [[toxins]], [[genetic]] factors, geomagnetism, Childhood environmental factors and [[infections]] have been proved to cause this differences in [[MS]] prevalence. Several studies demonstrated that if immigration occurs before the age of fifteen, the migrant's susceptibility to [[MS]] will be equal to that region's native people, But if migration occurs after the age of fifteen, the migrant's susceptibility will remain equal to his home country.<ref>Marrie, RA. ''Environmental risk factors in multiple sclerosis aetiology.'' Lancet Neurol. 2004 Dec;3(12):709-18. Review. PMID 15556803</ref> | ||
The | The prevalence of [[MS]] varies among countries. according to some studies [[MS]] occurs mostly in Caucasians while it is rare in the Native American tribes of North America, Australian Aborigines and the Māori of New Zealand. Among countries Scotland seems to have the highest rate of [[MS]] in the world.<ref>{{cite journal |author=Rothwell PM, Charlton D |title=High incidence and prevalence of multiple sclerosis in south east Scotland: evidence of a genetic predisposition |journal=J. Neurol. Neurosurg. Psychiatr. |volume=64 |issue=6 |pages=730-5 |year=1998 |pmid=9647300 |doi=}}</ref> We can conclude that due to [[genetic]] susceptibility, [[lifestyle]] and different culture, the development of this [[disease]] is not equal in various regions. [[autoimmune disorders]] such as [[MS]] is at least two times more common among women than men but this difference will disappear after the age of 50 and in children reach three females for each male. Onset of [[symptoms]] is mostly between age of fifteen to forty years, rarely before age fifteen or after age sixty. [[Genetics|genetic]] factors are an important risk factors to [[MS]] disease. It is estimated that among [[MS]] patients siblings, one can be affected eventually. The [[Identical twin|identical twins]] of [[MS]]-affected individuals, almost half of them will develop [[MS]], but in [[fraternal twins]] it's one of twenty.if one of the parents is affected by [[MS]], the risk of developing [[MS]] for each child is about one in forty.<ref>Sadovnick, AD, Ebers, GC, Dyment, DA, Risch, NJ. ''Evidence for genetic basis of multiple sclerosis. The Canadian Collaborative Study Group.'' Lancet 1996; 347:1728. PMID 8656905</ref> | ||
it is important to say that some studies on related [[diseases]] have shown that some diseases which were formerly considered [[MS]] cases are not [[MS]] at all. all the studies before 2004 can be affected because of inability to distinguish [[MS]] and [[Devic's disease]] (NMO).<ref>{{cite journal |author=Weinshenker B |title=Western vs optic-spinal MS: two diseases, one treatment?|journal=Neurology |volume=64 |issue=4 |pages=594-5 |year=2005 |pmid=15728277}}</ref> | |||
<gallery> | <gallery> | ||
Revision as of 20:28, 6 March 2018
|
Multiple sclerosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Multiple sclerosis epidemiology and demographics On the Web |
|
American Roentgen Ray Society Images of Multiple sclerosis epidemiology and demographics |
|
Multiple sclerosis epidemiology and demographics in the news |
|
Risk calculators and risk factors for Multiple sclerosis epidemiology and demographics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
Epidemiology and Demographics
There is a lower frequency of people suffering from Multiple Sclerosis among citizens of the Arabian Peninsula, Asia, and continental South America than people living in northern Europe, continental North America, and Australasia, which is about one of every 1000 citizens. In addition, in sub-Saharan Africa, MS is extremely rare.[1] factors including sunlight exposure, climate, diet, toxins, genetic factors, geomagnetism, Childhood environmental factors and infections have been proved to cause this differences in MS prevalence. Several studies demonstrated that if immigration occurs before the age of fifteen, the migrant's susceptibility to MS will be equal to that region's native people, But if migration occurs after the age of fifteen, the migrant's susceptibility will remain equal to his home country.[2]
The prevalence of MS varies among countries. according to some studies MS occurs mostly in Caucasians while it is rare in the Native American tribes of North America, Australian Aborigines and the Māori of New Zealand. Among countries Scotland seems to have the highest rate of MS in the world.[3] We can conclude that due to genetic susceptibility, lifestyle and different culture, the development of this disease is not equal in various regions. autoimmune disorders such as MS is at least two times more common among women than men but this difference will disappear after the age of 50 and in children reach three females for each male. Onset of symptoms is mostly between age of fifteen to forty years, rarely before age fifteen or after age sixty. genetic factors are an important risk factors to MS disease. It is estimated that among MS patients siblings, one can be affected eventually. The identical twins of MS-affected individuals, almost half of them will develop MS, but in fraternal twins it's one of twenty.if one of the parents is affected by MS, the risk of developing MS for each child is about one in forty.[4]
it is important to say that some studies on related diseases have shown that some diseases which were formerly considered MS cases are not MS at all. all the studies before 2004 can be affected because of inability to distinguish MS and Devic's disease (NMO).[5]
-
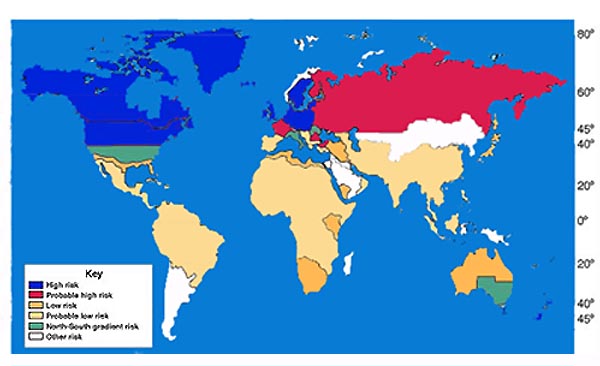
World map showing that risk for MS increases with greater distance from the equator

References
- ↑ Epidemiology and multiple sclerosis. a personal review
- ↑ Marrie, RA. Environmental risk factors in multiple sclerosis aetiology. Lancet Neurol. 2004 Dec;3(12):709-18. Review. PMID 15556803
- ↑ Rothwell PM, Charlton D (1998). "High incidence and prevalence of multiple sclerosis in south east Scotland: evidence of a genetic predisposition". J. Neurol. Neurosurg. Psychiatr. 64 (6): 730–5. PMID 9647300.
- ↑ Sadovnick, AD, Ebers, GC, Dyment, DA, Risch, NJ. Evidence for genetic basis of multiple sclerosis. The Canadian Collaborative Study Group. Lancet 1996; 347:1728. PMID 8656905
- ↑ Weinshenker B (2005). "Western vs optic-spinal MS: two diseases, one treatment?". Neurology. 64 (4): 594–5. PMID 15728277.