Sandbox:kalpana
Overview
Fetal hydantoin syndrome was first discovered by Meadow et al. in 1968. Manson and Frederic clarified the teratogenic effects of hydantoin in their epidemiological studies in 1973 and Hanson and Smith in 1975. Fetal hydantoin syndrome, characterized by altered growth and development, has been well described in recent years in the fetus of epileptic mothers taking phenytoin or other hydantoin anticonvulsants during the gestational period. It is understood that fetal hydantoin syndromes is the result of infants born to mothers with seizure disorders treated with anticonvulsant medications during pregnancy. There is also an association with EPHX1 has been suggested. Although the exact pathogenesis of phenytoin (PTN) embryo toxicity is not clear, some possible mechanisms have been proposed. Phenytoin inhibits sodium (Na) and calcium (Ca) channels which act as membrane stabilizers, as a result of which free radicals are released and cause endothelial damage, myocardial depression, bradycardia, and consequently fetal hypoxia. Phenytoin induces cytochrome P450 activation which ends up within the release of teratogenic free radicals, sourced via the metabolism of epoxides, folate, and vitamin K within the liver. The severity of associated abnormalities will vary greatly from one infant to another. The characteristic features of fetal hydantoin synrome include abnormalities of growth such as pre and postnatal growth deficiency and microcephaly abnormalities of performance such as developmental delay or dull mentality to frank mental deficiency; and dysmorphic craniofacial features commonly including short nose with broad depressed bridge and inner epicanthic folds, mild ocular hypertelorism, ptosis of the eyelid, strabismus, wide mouth, sutural ridging, and short neck with mild webbing; less commonly cleft lip and palate, and limb anomalies including hypoplasia of the nails and distal phalanges with an increased frequency of low arch digital dermal ridge patterns, and fingerlike thumb. Less commonly children displaying these dysmorphic craniofacial and limb features were reported to have major anomalies in other systems, including cardiac anomalies. It was also shown an increased incidence of major genitourinary and central nervous system anomalies, more serious limb reduction defects, and diaphragmatic hernia. Fetal hydantoin syndrome may be caused by a combination of specific genetic and environmental factors. Common causes of fetal hydantoin syndrome may include anti-seizure(anticonvulsant) drug phenytoin (Dilantin) during pregnancy. Fetal hydantoin syndrome must be differentiated from other diseases that cause Hypoplastic nails and growth retardation along with some similar facial features are also found in the Coffin-Siris, Hypoplasia of distal phalanges in Noonan's syndrome and Nail hypoplasia in Robinson's disease. The exact incidence and prevalence of the fetal hydantoin syndrome is unknown.The risk appears to be 2-3 times greater than normal in the children of epileptic women taking anticonvulsant drugs than in the general population. The exact incidence and prevalence of the fetal hydantoin syndrome is unknown.The risk appears to be 2-3 times greater than normal in the children of epileptic women taking anticonvulsant drugs than in the general population. The risk of neurological impairment estimated to be 1% to 11% is 2 to 3 times higher than in the general population. The risk of oral clefts and cardiac anomalies is 5 times than others in hydantoin exposed infants. Less frequently observed abnormalities include microcephaly, ocular defects, hypospadias, umbilical and inguinal hernias. Fetal hydantoin syndrome affects males and females equally. Common risk factors in the development of fetal hydantoin syndrome include exposure of fetus to antiepileptic drugs phenytoin(Dilantin). There is insufficient evidence to recommend routine screening for fetal hydantoin syndrome. But In case fetus exposed in utero to phenytoin, screening by cytogenetic analysis, a careful screening by morphological ultrasound was recommended.Without termination of pregnancy, the patient will develop conditions of severe respiratory distress, multiple congenital anomalies, including an imperforate anus, ambiguous genitalia, dislocated hips, clubfeet, hypoplastic fingernails, a short neck, and a barrel-shaped thorax, swollen thigh, decrease breath sound and cardiac murmur which may eventually lead to neonatal death. Common complications of fetal hydantoin syndrome is microcephaly, growth deficiency, congenital heart defects, systemic abnormalities (nervous, renal, GI systems). The diagnosis is based on the clinical features along with a history of phenytoin exposure during pregnancy. Ultrasound may be helpful in the diagnosis of fetal hydantoin syndrome. Findings on ultrasound suggestive of fetal hydantoin syndrome includes gastroschisis, sacral meningomyelocele, absence of the upper limb lower limb, clubfoot, Pectus carinatum, dilated right/left heart with peri- cardial effusion. reatment of individuals with fetal hydantoin syndrome depends on the particular manifestation of the disease. Individuals with congenital heart disease may require to undergo major corrective surgery soon after birth. Other individuals who have relatively minor health problems require no therapy. Patients with fetal hydantoin syndrome require to follow up and close monitoring of growth, psychomotor craniofacial evaluation, cardiac evaluation.
Historical Perspective
Fetal hydantoin syndrome was first discovered by Meadow et al. in 1968. Manson and Frederic clarified the teratogenic effects of hydantoin in their epidemiological studies in 1973[1]and Hanson and Smith in 1975.[2]
Classification
There is no established system for the classification of Fetal hydantoin syndrome.
Pathophysiology
It is understood that fetal hydantoin syndromes is the result of infants born to mothers with seizure disorders treated with anticonvulsant medications during pregnancy are at an increased risk for teratogenic effects.[3]There is also an association with EPHX1 has been suggested.[4] Although the exact pathogenesis of phenytoin (PTN) embryo toxicity is not clear, some possible mechanisms have been proposed.[5] Phenytoin inhibits sodium (Na) and calcium (Ca) channels which act as membrane stabilizers, as a result of which free radicals are released and cause endothelial damage, myocardial depression, bradycardia, and consequently fetal hypoxia. Phenytoin induces cytochrome P450 activation which ends up within the release of teratogenic free radicals, sourced via the metabolism of epoxides, folate, and vitamin K within the liver.[6][7]The severity of associated abnormalities will vary greatly from one infant to another. The characteristic features of fetal hydantoin synrome include abnormalities of growth such as prenatal (IUGR) and postnatal growth deficiency and microcephaly abnormalities of performance such as developmental delay or dull mentality to frank mental deficiency; and dysmorphic craniofacial features commonly including short nose with broad depressed bridge and inner epicanthic folds, mild ocular hypertelorism, ptosis of the eyelid, strabismus, wide mouth, sutural ridging, and short neck with mild webbing; less commonly cleft lip and cleft palate, and limb anomalies including hypoplasia of the nails and distal phalanges with an increased frequency of low arch digital dermal ridge patterns, and fingerlike thumb (Triphalangeal-thumb). Less commonly children displaying these dysmorphic craniofacial and limb features were reported to have major anomalies in other systems, including cardiac anomalies. It was also shown an increased incidence of major genitourinary and central nervous system anomalies, more serious limb reduction defects, and diaphragmatic hernia.[8]
{kind=link}
{kind=link}
{kind=link}
Causes
Fetal hydantoin syndrome may be caused by a combination of specific genetic and environmental factors. Common causes of fetal hydantoin syndrome may include anti-seizure(anticonvulsant) drug phenytoin (Dilantin) during pregnancy.[9]
Differential Diagnosis
Fetal hydantoin syndrome must be differentiated from other diseases that cause Hypoplastic nails and growth retardation along with some similar facial features are also found in the Coffin-Siris,[10] Hypopiasia of distal phalanges in Noonan's syndrome and Nail hypoplasia in Robinson's disease[11]
Epidemiology and Demographics
The exact incidence and prevalence of the fetal hydantoin syndrome is unknown.The risk appears to be 2-3 times greater than normal in the children of epileptic women taking anticonvulsant drugs than in the general population.[12] The risk of neurological impairment estimated to be 1% to 11% is 2 to 3 times higher than in the general population. The risk of oral clefts and cardiac anomalies is 5 times than others in hydantoin exposed infants. Less frequently observed abnormalities include microcephaly, ocular defects, hypospadias, umbilical and inguinal hernias.[3]
Risk factors
Common risk factors in the development of fetal hydantoin syndrome include exposure of fetus to antiepileptic drugs phenytoin(Dilantin).[12]
Screening
There is insufficient evidence to recommend routine screening for fetal hydantoin syndrome. But In case fetus exposed in utero to phenytoin, screening by cytogenetic analysis, a careful screening by morphological ultrasound was recommended.[13]
Natural History, Complications, and Prognosis
Without termination of pregnancy, the patient will develop conditions of severe respiratory distress, multiple congenital anomalies, including an imperforate anus, ambiguous genitalia, dislocated hips, clubfeet, hypoplastic fingernails, a short neck, and a barrel-shaped thorax, swollen thigh, decrease breath sound and cardiac murmur which may eventually lead to neonatal death.[14]Common complications of fetal hydantoin syndrome is microcephaly, growth deficiency, congenital heart defects, systemic abnormalities (nervous, renal, GI systems).[3]
Diagnosis
Diagnostic Study of Choice
There are no established criteria for the diagnosis of fetal hydantoin syndrome. The diagnosis is based on the clinical features along with a history of phenytoin exposure during pregnancy.[11]
History and Symptoms
The patient with fetal hydantoin syndrome has a positive history of exposure to phenytoin during pregnancy. Common symptoms of fetal hydantoin syndrome include microcephaly, mental retardation, limb defects including hypoplastic nails and distal phalanges, heart defects.
Physical Examination
Common physical examination findings of fetal hydantoin syndrome include
- microcephaly, distinctive facial (cleft lip and palate) and limb anomalies, ocular defects, growth deficiency, congenital heart defects, cardiac rhythm disturbances, and variable systemic abnormalities involving the nervous, renal, and gastrointestinal systems.
- Congenital heart diseases associated with fetal hydantoin syndrome include pulmonary or aortic valvular stenosis, coarctation of aorta, patent ductus arteriosus, and ventricular septal defects.[15]
{kind=link}
Laboratory Findings
There are no diagnostic laboratory findings associated with fetal hydantoin syndrome.
Electrocardiogram
There are no ECG findings associated with fetal hydantoin syndrome.
Echocardiography
Echocardiography may be helpful in the diagnosis of fetal hydantoin syndrome. Findings on echocardiography suggestive of pulmonary or aortic valvular stenosis, coarctation of aorta, patent ductus arteriosus, and ventricular septal defects.
X Ray
An X-ray may be helpful in the diagnosis of fetal hydantoin syndrome. Findings on X-ray diagnostic of fetal hydantoin syndrome depends on the clinical features and include an absence of carpal, metacarpal, and phalangeal bone, hypoplasia of the nails and distal phalanges, Hyperphalangism, Pseudohyperphalangism, Adactyly/biphalangeal digits/absent nails Unilateral acheiria, congenital heart disease. [16]

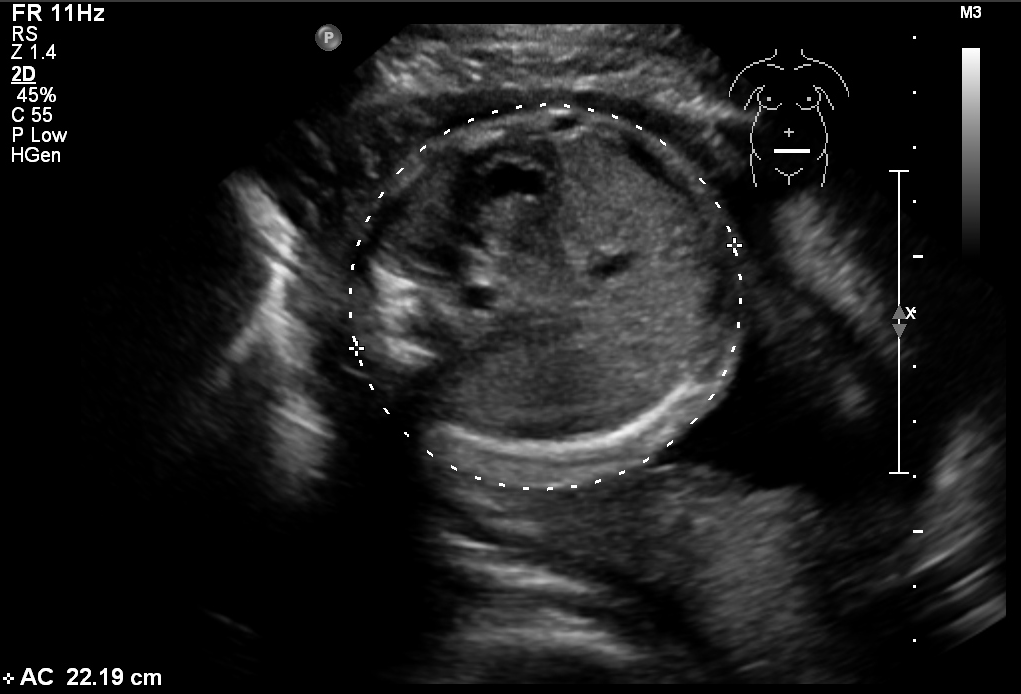
Ultrasound
Ultrasound may be helpful in the diagnosis of fetal hydantoin syndrome. Findings on ultrasound suggestive of fetal hydantoin syndrome includes gastroschisis, sacral meningomyelocele, absence of the upper limb lower limb, clubfoot, Pectus carinatum.[13] dilated right/left heart with peri- cardial effusion[15]
.JPG)
CT scan
There are no CT scan findings associated with fetal hydantoin syndrome.
Other Imaging Findings
There are no other imaging findings associated with fetal hydantoin syndrome.
Other Diagnostic Studies
Other diagnostic studies for fetal hydantoin syndrome include amniocentesis demonstrates, low epoxide hydrolase activity[17]
Treatment
Medical Therapy
Treatment of individuals with fetal hydantoin syndrome depends on the particular manifestation of the disease. Individuals with congenital heart disease may require to undergo major corrective surgery soon after birth. Other individuals who have relatively minor health problems require no therapy. Patients with fetal hydantoin syndrome require to follow up and close monitoring of growth, psychomotor craniofacial evaluation, cardiac evaluation.[3]
Surgery
Treatment of individuals with fetal hydantoin syndrome depends on the particular manifestation of the disease. Individuals with defects of bone require orthopedic surgery, nervous system require neurosurgery, cleft lip or cleft palate surgery and congenital heart disease may require to undergo major corrective surgery soon after birth. Other individuals who have relatively minor health problems require no therapy.[3]
Prevention
Primary Prevention
Effective measures for the primary prevention of fetal hydantoin syndrome include[18]
- changing AED from polytherapy to monotherapy before pregnancy
- decreasing the serum concentration of AEDs to the lowest levels possible without losing seizure control
- especially reducing PHT serum levels, supplementation with folate before pregnancy
- regular check‐up of the AED serum concentrations, folate, and α‐fetoprotein (AFP) values
- counseling with parents regarding the risk of pregnancy and malformations
- regular check‐up of the fetus directly with ultrasonography.
Secondary Prevention
Effective measures for the secondary prevention of fetal Hydantoin syndrome include[18]
- Periodic health checks of psychomotor and physical development.
- Electroencephalography: Annually
- Counseling: instructions regarding children with handicaps and/or psychomotor retardation
References
- ↑ Ozkinay F, Yenigün A, Kantar M, Ozkinay C, Avanoğlu A, Ulman I (1998). "Two siblings with fetal hydantoin syndrome". Turk J Pediatr. 40 (2): 273–8. PMID 9677735.
- ↑ "Reorganized text". JAMA Otolaryngol Head Neck Surg. 141 (5): 428. 2015. doi:10.1001/jamaoto.2015.0540. PMID 25996397.
- ↑ 3.0 3.1 3.2 3.3 3.4 Singh R, Kumar N, Arora S, Bhandari R, Jain A (2012). "Fetal hydantoin syndrome and its anaesthetic implications: a case report". Case Rep Anesthesiol. 2012: 370412. doi:10.1155/2012/370412. PMC 3469078. PMID 23082254.
- ↑ Online Mendelian Inheritance in Man (OMIM) 132810
- ↑ Webster WS, Howe AM, Abela D, Oakes DJ (2006). "The relationship between cleft lip, maxillary hypoplasia, hypoxia and phenytoin". Curr Pharm Des. 12 (12): 1431–48. doi:10.2174/138161206776389868. PMID 16611127.
- ↑ Nilsson MF, Ritchie H, Webster WS (2013). "The effect on rat embryonic heart rate of Na+, K+, and Ca2+ channel blockers, and the human teratogen phenytoin, changes with gestational age". Birth Defects Res B Dev Reprod Toxicol. 98 (5): 416–27. doi:10.1002/bdrb.21084. PMID 24323366.
- ↑ Azarbayjani F, Danielsson BR (2001). "Phenytoin-induced cleft palate: evidence for embryonic cardiac bradyarrhythmia due to inhibition of delayed rectifier K+ channels resulting in hypoxia-reoxygenation damage". Teratology. 63 (3): 152–60. doi:10.1002/tera.1026. PMID 11283972.
- ↑ Hanson JW, Buehler BA (1982). "Fetal hydantoin syndrome: current status". J Pediatr. 101 (5): 816–8. doi:10.1016/s0022-3476(82)80339-9. PMID 7131169.
- ↑ Jimenez JF, Seibert RW, Char F, Brown RE, Seibert JJ (1981). "Melanotic neuroectodermal tumor of infancy and fetal hydantoin syndrome". Am J Pediatr Hematol Oncol. 3 (1): 9–15. PMID 6263127.
- ↑ Hanson JW, Smith DW (1975). "The fetal hydantoin syndrome". J Pediatr. 87 (2): 285–90. doi:10.1016/s0022-3476(75)80604-4. PMID 50428.
- ↑ 11.0 11.1 Nanda A, Kaur S, Bhakoo ON, Kapoor MM, Kanwar AJ (1989). "Fetal hydantoin syndrome: a case report". Pediatr Dermatol. 6 (2): 130–3. doi:10.1111/j.1525-1470.1989.tb01011.x. PMID 2501774.
- ↑ 12.0 12.1 Speidel BD, Meadow SR (1972). "Maternal epilepsy and abnormalities of the fetus and newborn". Lancet. 2 (7782): 839–43. doi:10.1016/s0140-6736(72)92209-x. PMID 4116552.
- ↑ 13.0 13.1 "A case of prenatal diagnosis of fetal hydantoin syndrome by ultrasound".
- ↑ Kogutt MS, Young LW (1984). "Radiological case of the month. Fetal hydantoin syndrome". Am J Dis Child. 138 (4): 405–6. doi:10.1001/archpedi.1984.02140420071021. PMID 6702795.
- ↑ 15.0 15.1 Hegde A, Kaur A, Sood A, Dhanorkar M, Varma HT, Singh G; et al. (2017). "Fetal Hydantoin Syndrome". J Pediatr. 188: 304. doi:10.1016/j.jpeds.2017.05.018. PMID 28578158.
- ↑ Sabry MA, Farag TI (1996). "Hand anomalies in fetal-hydantoin syndrome: from nail/phalangeal hypoplasia to unilateral acheiria". Am J Med Genet. 62 (4): 410–2. doi:10.1002/ajmg.1320620403. PMID 8723073.
- ↑ Buehler BA, Delimont D, van Waes M, Finnell RH (1990). "Prenatal prediction of risk of the fetal hydantoin syndrome". N Engl J Med. 322 (22): 1567–72. doi:10.1056/NEJM199005313222204. PMID 2336087.
- ↑ 18.0 18.1 Oguni M, Osawa M (2004). "Epilepsy and pregnancy". Epilepsia. 45 Suppl 8: 37–41. doi:10.1111/j.0013-9580.2004.458008.x. PMID 15610193.