Bone fracture natural history, complications and prognosis
|
Bone fracture Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Bone fracture natural history, complications and prognosis On the Web |
|
American Roentgen Ray Society Images of Bone fracture natural history, complications and prognosis |
|
FDA on Bone fracture natural history, complications and prognosis |
|
CDC on Bone fracture natural history, complications and prognosis |
|
Bone fracture natural history, complications and prognosis in the news |
|
Blogs on Bone fracture natural history, complications and prognosis |
|
Risk calculators and risk factors for Bone fracture natural history, complications and prognosis |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Natural History
Bone Healing
The natural process of healing a fracture starts when the injured bone and surrounding tissues bleed. The blood coagulates to form a blood clot situated between the broken fragments. Within a few days blood vessels grow into the jelly-like matrix of the blood clot. The new blood vessels bring white blood cells to the area, which gradually remove the non-viable material. The blood vessels also bring fibroblasts in the walls of the vessels and these multiply and produce collagen fibers. In this way the blood clot is replaced by a matrix of collagen. Collagen's rubbery consistency allows bone fragments to move only a small amount unless severe or persistent force is applied.
At this stage, some of the fibroblasts begin to lay down bone matrix (calcium hydroxyapatite) in the form of insoluble crystals. This mineralization of the collagen matrix stiffens it and transforms it into bone. In fact, bone is a mineralized collagen matrix; if the mineral is dissolved out of bone, it becomes rubbery. Healing bone callus is on average sufficiently mineralized to show up on X-ray within 6 weeks in adults and less in children. This initial "woven" bone does not have the strong mechanical properties of mature bone. By a process of remodeling, the woven bone is replaced by mature "lamellar" bone. The whole process can take up to 18 months, but in adults the strength of the healing bone is usually 80% of normal by 3 months after the injury.
Several factors can help or hinder the bone healing process. For example, any form of nicotine hinders the process of bone healing, and adequate nutrition (including calcium intake) will help the bone healing process. Weight-bearing stress on bone, after the bone has healed sufficiently to bear the weight, also builds bone strength. Although there are theoretical concerns about NSAIDs slowing the rate of healing, there is not enough evidence to warrant withholding the use of this type analgesic in simple fractures.
-
 X-ray showing a healed tibia fracture with pins.
X-ray showing a healed tibia fracture with pins. -
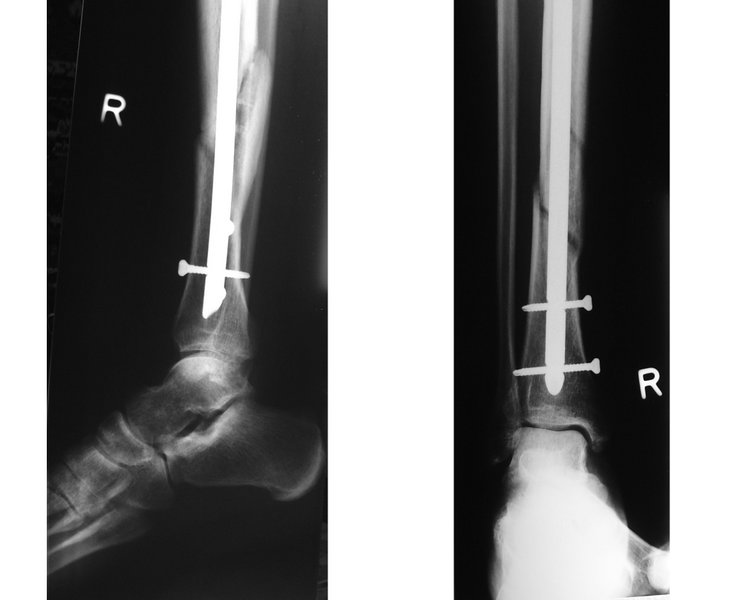 X-ray showing fractured tibia and pinning.
X-ray showing fractured tibia and pinning.


Complications
Some fractures can lead to serious complications including a condition known as compartment syndrome. If not treated, compartment syndrome can result in amputation of the affected limb. Other complications may include non-union, where the fractured bone fails to heal or mal-union, where the fractured bone heals in a deformed manner.
In children, whose bones are still developing, there are risks of either a growth plate injury or a greenstick fracture.
- A greenstick fracture occurs due to mechanical failure on the tension side. That is, since the bone is not as brittle as it would be in an adult, it does not completely fracture, but rather exhibits bowing without complete disruption of the bone's cortex in the surface opposite the applied force.
- Growth plate injuries, as in Salter-Harris fractures, require careful treatment and accurate reduction to make sure that the bone continues to grow normally.
- Plastic deformation of the bone, in which the bone permanently bends but does not break, is also possible in children. These injuries may require an osteotomy (bone cut) to realign the bone if it is fixed and cannot be realigned by closed methods.
- Certain fractures are known to occur mainly in the pediatric age group, such as fracture of the clavicle and supracondylar fracture of the humerus.
Prognosis
For most fractures, the whole process can take up to 18 months, but in adults the strength of the healing bone is usually 80% of normal by 3 months after the injury.