Bicuspid aortic stenosis pathophysiology
|
Bicuspid aortic stenosis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Bicuspid aortic stenosis pathophysiology On the Web |
|
American Roentgen Ray Society Images of Bicuspid aortic stenosis pathophysiology |
|
Risk calculators and risk factors for Bicuspid aortic stenosis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Usama Talib, BSc, MD [3]
Overview
A congenital bicuspid aortic valve may be associated with the development of either progressive clacific stenosis or regurgitation. What differentiates the pathophysiology of bicuspid aortic stenosis from other forms of aortic stenosis such as the degenerative aortic stenosis is the presence of concomitant valve disease, aortic root disease, and an increased incidence of coarctation of the aorta.[1]
Pathophysiology of Aortic Stenosis
The pathophysiology of aortic stenosis is described in the main chapter on the pathophysiology of aortic stenosis here. What differentiates the pathophysiology of bicuspid aortic stenosis from other forms of aortic stenosis such as the degenerative aortic stenosis is the presence of concomitant valve disease, aortic root disease, and an increased incidence of coarctation of the aorta.[2]
Incidence of Concomitant Valve Disease
- Only 25% of patients with congenital aortic stenosis (AS) have aortic insufficiency (AI) compared with 75% of cases with acquired AS.
- In 75% of those with acquired AS, there is associated mitral valve disease. This association is rare in congenital AS.
Concomitant Disease of the Aorta
The aorta of patients with bicuspid aortic valve does not have the same histological characteristics of a normal aorta. The tensile strength is reduced. These patients are at a higher risk for aortic dissection and aneurysm formation of the ascending aorta. The size of the proximal aorta should be evaluated carefully during the evaluation of the patient for aortic stenosis surgery. The initial diameter of the aorta should be noted and periodic evaluation with CT scan (every year or sooner if there is a change in aortic diameter) should be recommended. Therefore, if the patient needs surgery, the size of the aorta will determine what type of surgery should be offered to the patient.[3]
Associated Congenital Heart Disease
Patients with bicuspid aortic valve are also at higher risk of aortic coarctation, an abnormal narrowing of the thoracic aorta [4].
Gross Pathology
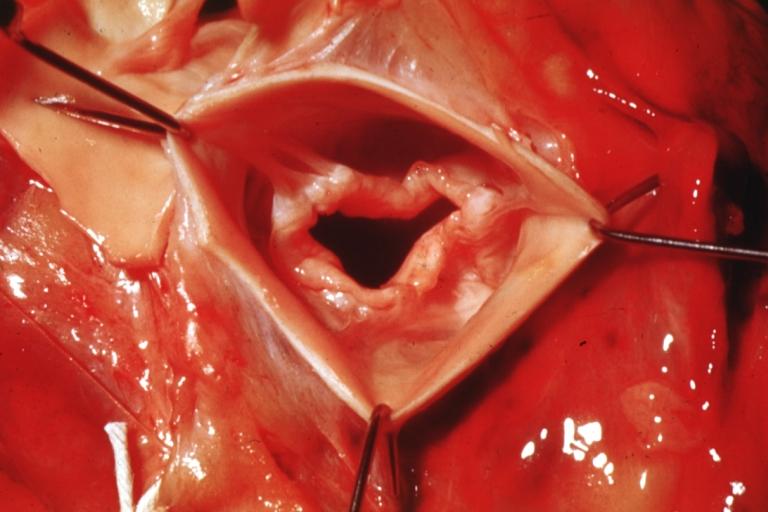
Gross pathologic evaluation in patients with bicuspid aortic stenosis demonstrates fusion of one of the three commisures which results in two functional leaflets instead of the usual three aortic leaflets. Left ventricular hypertrophy is present in bicuspid aortic stenosis.[5]
Pathological Findings
Images shown below are courtesy of Professor Peter Anderson DVM PhD[6] and published with permission.
-
 Aortic Stenosis, Bicuspid valve: Gross; excellent image of bicuspid and calcific valve showing a false raphe.
Aortic Stenosis, Bicuspid valve: Gross; excellent image of bicuspid and calcific valve showing a false raphe. -
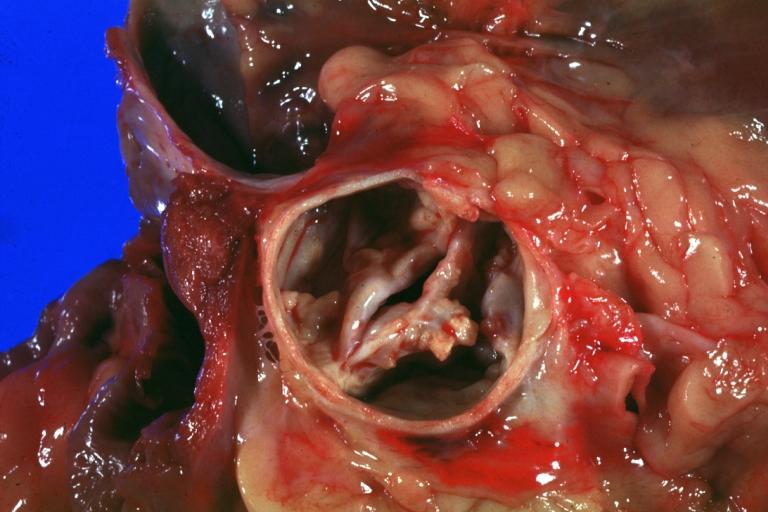
 Aortic Stenosis, Bicuspid valve: Gross; good example of bicuspid valve
Aortic Stenosis, Bicuspid valve: Gross; good example of bicuspid valve


-
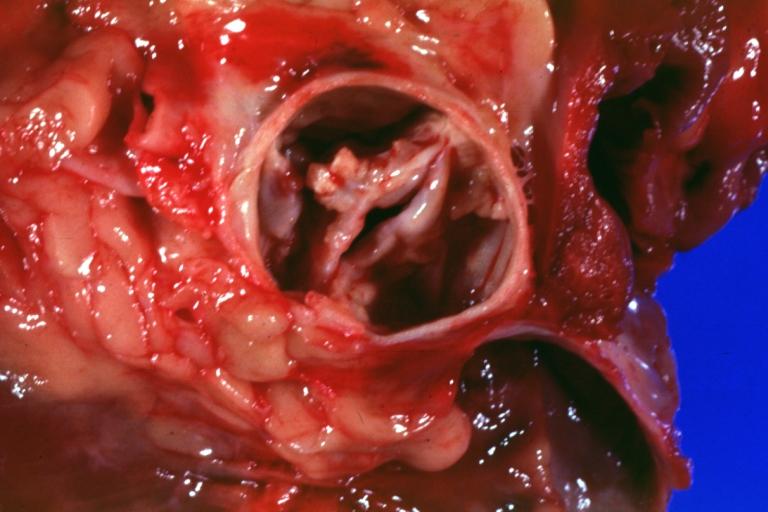
 Aortic Stenosis, Bicuspid valve: Gross; image of bicuspid aortic valve, an excellent example
Aortic Stenosis, Bicuspid valve: Gross; image of bicuspid aortic valve, an excellent example -
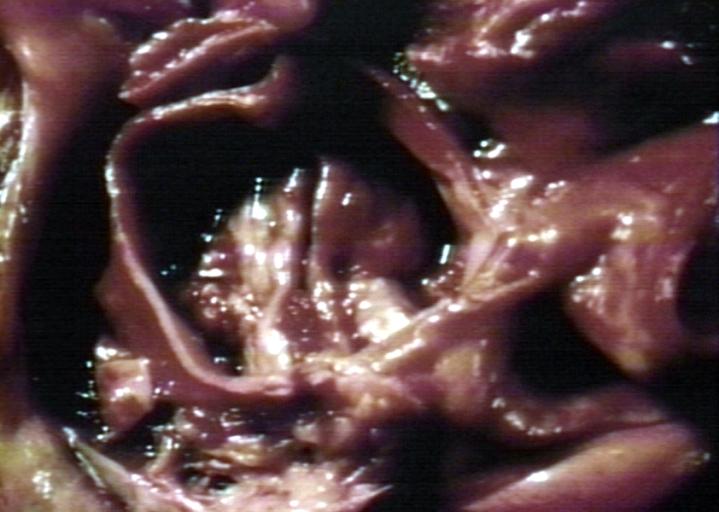
 Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve.
Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve.


-
 Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve.
Aortic Stenosis, Bicuspid valve: Gross; close-up image of bicuspid aortic valve. -
 Bicuspid aortic valve
Bicuspid aortic valve


-
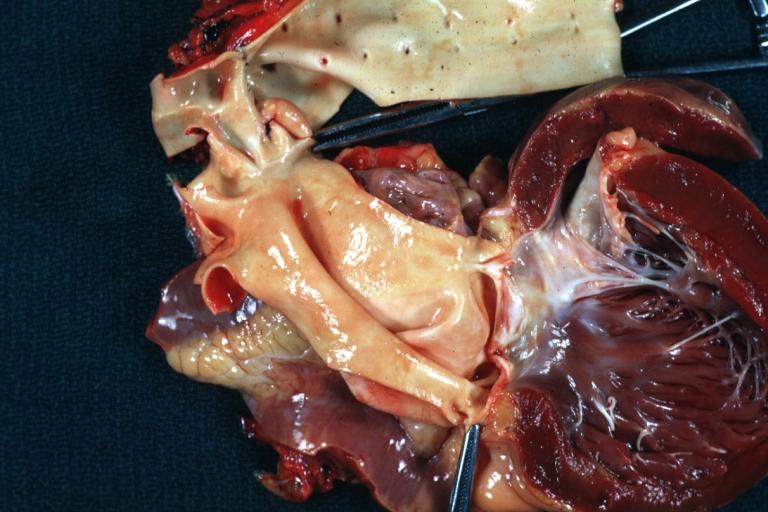
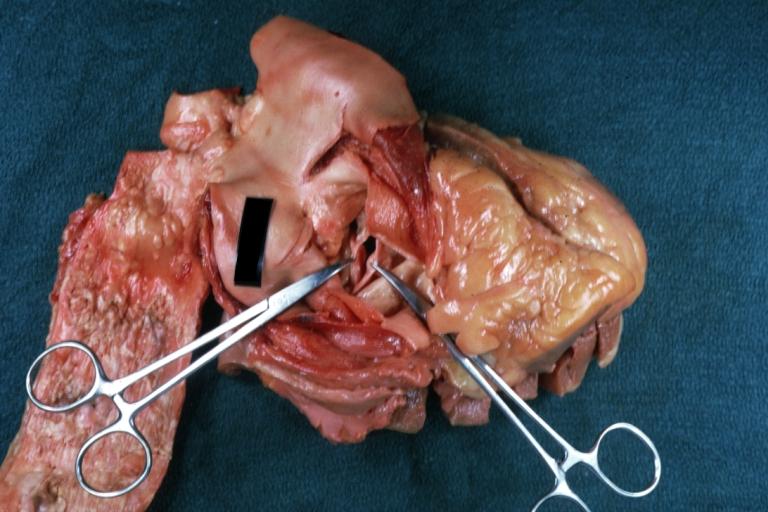 Gross natural color opened first portion aortic arch with bicuspid aortic valve shows stenosis and aortic root is dilated
Gross natural color opened first portion aortic arch with bicuspid aortic valve shows stenosis and aortic root is dilated -
 Aortic Stenosis Bicuspid: Gross; natural color opened left ventricular outflow tract with calcific masses on valve as well as anterior leaflet mitral valve probably did not cause significant stenosis
Aortic Stenosis Bicuspid: Gross; natural color opened left ventricular outflow tract with calcific masses on valve as well as anterior leaflet mitral valve probably did not cause significant stenosis


-
 Bicuspid Aortic Valve with Repaired Aorta Coarctation: Gross natural color opened left ventricular outflow tract with uncomplicated bicuspid aortic valve repaired coarctation barely visible ruptured postoperative young female with ovaries Turner mosaic not ruled out
Bicuspid Aortic Valve with Repaired Aorta Coarctation: Gross natural color opened left ventricular outflow tract with uncomplicated bicuspid aortic valve repaired coarctation barely visible ruptured postoperative young female with ovaries Turner mosaic not ruled out -
 Bicuspid Aortic Stenosis: Gross; fixed tissue
Bicuspid Aortic Stenosis: Gross; fixed tissue


-
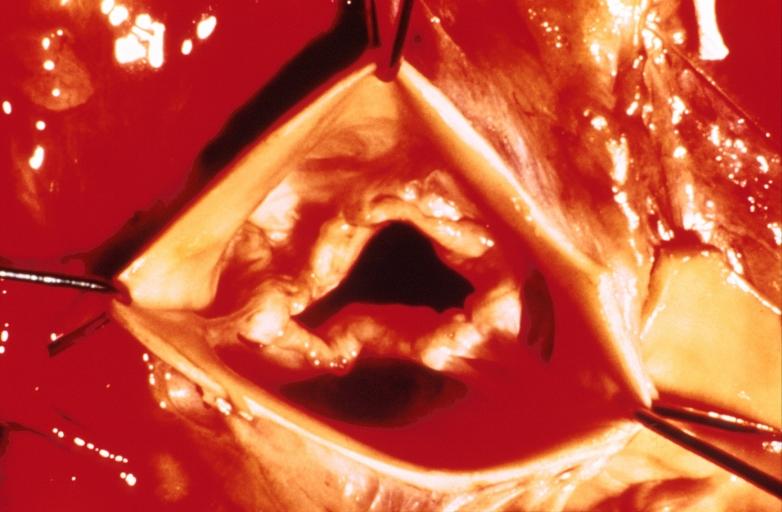
 Aortic Stenosis, Bicuspid: Gross; fixed tissue view of stenotic valve through ventricular outlet track
Aortic Stenosis, Bicuspid: Gross; fixed tissue view of stenotic valve through ventricular outlet track -
 Aortic Stenosis Bicuspid: Gross; fixed tissue. Bicuspid valve and false raphe classical
Aortic Stenosis Bicuspid: Gross; fixed tissue. Bicuspid valve and false raphe classical


-
 Bicuspid aortic valve
Bicuspid aortic valve -
 Bicuspid aortic valve
Bicuspid aortic valve


-
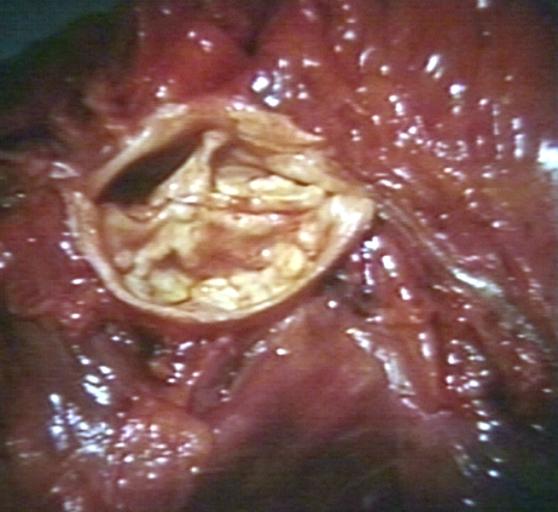 Bicuspid aortic valve
Bicuspid aortic valve -
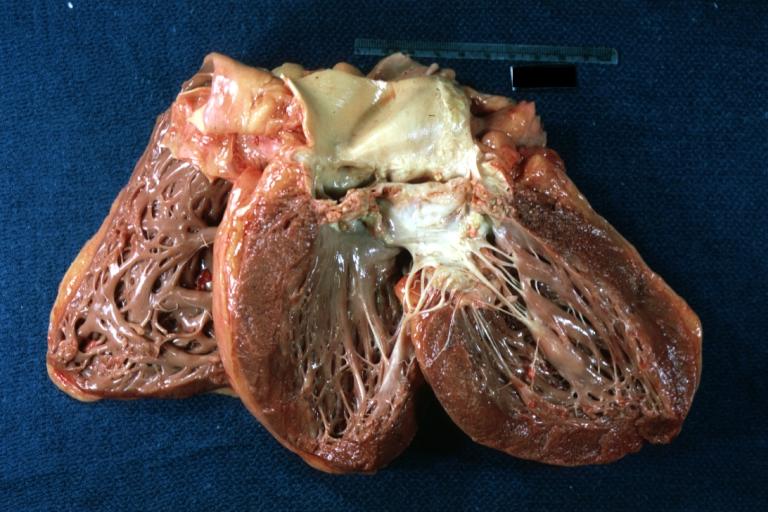
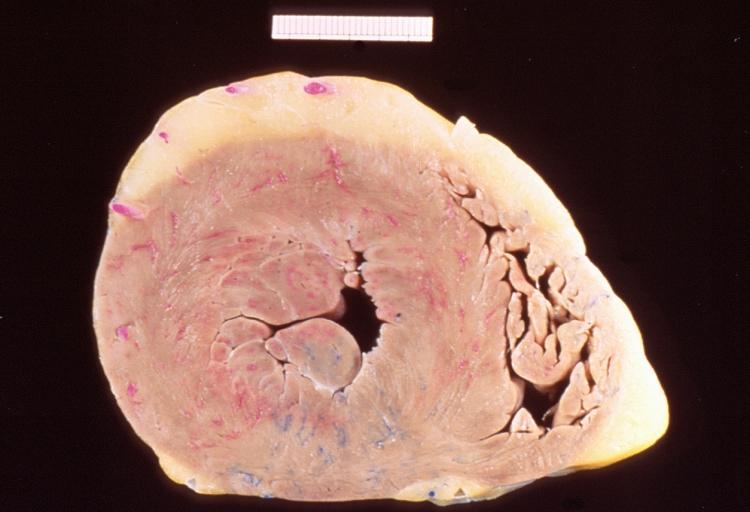 Left ventricular hypertrophy due to bicuspid aortic valve
Left ventricular hypertrophy due to bicuspid aortic valve


References
- ↑ Bonow RO, Carabello BA, Chatterjee K, de Leon AC, Faxon DP, Freed MD; et al. (2008). "2008 focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Endorsed by the Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons". J Am Coll Cardiol. 52 (13): e1–142. doi:10.1016/j.jacc.2008.05.007. PMID 18848134.
- ↑ Dweck MR, Boon NA, Newby DE (2012). "Calcific aortic stenosis: a disease of the valve and the myocardium". J Am Coll Cardiol. 60 (19): 1854–63. doi:10.1016/j.jacc.2012.02.093. PMID 23062541.
- ↑ Zilberszac R, Gabriel H, Schemper M, Laufer G, Maurer G, Rosenhek R (2016). "Asymptomatic Severe Aortic Stenosis in the Elderly". JACC Cardiovasc Imaging. doi:10.1016/j.jcmg.2016.05.015. PMID 27639763.
- ↑ Cohn LH, Edmunds LH Jr. Cardiac Surgery in the Adult. McGraw-Hill, 2003.
- ↑ Jang JY, Seo JS, Sun BJ, Kim DH, Song JM, Kang DH; et al. (2016). "Impact of Valvuloarterial Impedance on Concentric Remodeling in Aortic Stenosis and Its Regression after Valve Replacement". J Cardiovasc Ultrasound. 24 (3): 201–207. doi:10.4250/jcu.2016.24.3.201. PMC 5050308. PMID 27721950.
- ↑ http://www.peir.net © PEIR, University of Alabama at Birmingham, Department of Pathology