80 Lead EKG


|
WikiDoc Resources for 80 Lead EKG |
|
Articles |
|---|
|
Most recent articles on 80 Lead EKG Most cited articles on 80 Lead EKG |
|
Media |
|
Powerpoint slides on 80 Lead EKG |
|
Evidence Based Medicine |
|
Clinical Trials |
|
Ongoing Trials on 80 Lead EKG at Clinical Trials.gov Clinical Trials on 80 Lead EKG at Google
|
|
Guidelines / Policies / Govt |
|
US National Guidelines Clearinghouse on 80 Lead EKG
|
|
Books |
|
News |
|
Commentary |
|
Definitions |
|
Patient Resources / Community |
|
Patient resources on 80 Lead EKG Discussion groups on 80 Lead EKG Patient Handouts on 80 Lead EKG Directions to Hospitals Treating 80 Lead EKG Risk calculators and risk factors for 80 Lead EKG
|
|
Healthcare Provider Resources |
|
Causes & Risk Factors for 80 Lead EKG |
|
Continuing Medical Education (CME) |
|
International |
|
|
|
Business |
|
Experimental / Informatics |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Overview
ST elevation myocardial infarction (STEMI) is the most serious form of heart attack. The ST segments elevate because the full thickness of heart muscle is injured (transmural injury). This full thickness injury and ST elevation is the result of a total occlusion of a coronary artery. Some STEMIs, particularly those involving the posterior or back surface of the heart, may be missed by the present traditional system of placing a limited number of leads on the front of the chest.
In contrast to the 12 leads of data and the limited anterior or front view of the heart from a traditional EKG, an 80 lead EKG (such as the PRIME ECG®) utilizes 80 leads placed on both the front and back of the patient to analyze a 360-degree spatial view of the heart. This new technology may allow the more rapid and accurate detection of STEMI and thereby potentially speed the delivery of care.
Display of 80 Lead EKG Data
Analysis is performed on a computer selected representative beat. ST-segment elevation and depression are translated into colors (red = elevation, blue = depression) and displayed against a 3 dimensional torso image for physician review. These images allow for rapid pattern recognition that identifies problem areas that correlate with regions of ischemia or infarction. This use of graphic imaging allows the physician to quickly focus on specific ECG morphology that contains the most valuable diagnostic information without having to expend time exploring data from all 80 leads. System software facilitates examination of the actual ECG trace for each of the 80 recordings. The user places a cursor over the suspect area and a pop-up window reveals the underlying electrode tracing and provides the value of elevation or depression at that lead.
Sensitivity and Specificity of 80 Lead EKGs
Ten years of clinical data and in-hospital experience have demonstrated an increase in sensitivity over the 12 lead EKG in the range of 18% with no loss in specificity. As a result, there is the potential to detect up to 40% more ST Elevation MIs (serious heart attacks) than the traditional 12-lead EKG.
Delays in Diagnosing ST Elevation MI with Traditional 12 Lead Systems
Registry data from the National Registry of Myocardial Infarction (NRMI), CRUSADE and GRACE have demonstrated that there are significant opportunities for improvement in door-to-balloon time and door-to-needle time in the management of serious heart attacks (STEMI). The 80 lead ECG may provide a technological advance that would speed the correct diagnosis of ST elevation MI. A substantial number of patients have a non-diagnostic 12-lead and these patients may wait for extended periods in the emergency room pending the results of tests that measure enzymes released into the bloodstream (biomarkers) to diagnose a heart attack.
The Potential to Miss the Diagnosis of STEMI Using the Traditional 12 Lead EKG
Heart attacks involving the back side of the heart may cause ST depression rather than ST elevation (STEMI) becuase the pattern of electrical injury is reversed on the traditional 12 lead EKG. One of These patients may currently be receiving less aggressive care because of a diagnosis of non-ST-elevation MI (NSTEMI) based on ST-depression, which may in fact be ST-elevation in a portion of the heart not visible with the 12 lead. Assuming approximately 20-30% of diagnosed MI patients are now diagnosed as STEMI patients and 70-80% are diagnosed as NSTEMI, the PRIME data would indicate that approximately 1 in every 3 patients may in fact be at a higher risk which would make them suitable for more aggressive care.
Example of a STEMI Missed on 12 Lead EKG Detected on 80 Lead EKG
Be sure to click on the images below to enlarge them

Shown below is the 12 lead EKG in a patient that presented with substernal chest pain. Note that there are non diagnostic changes. There is no evidence of ST segment elevation.
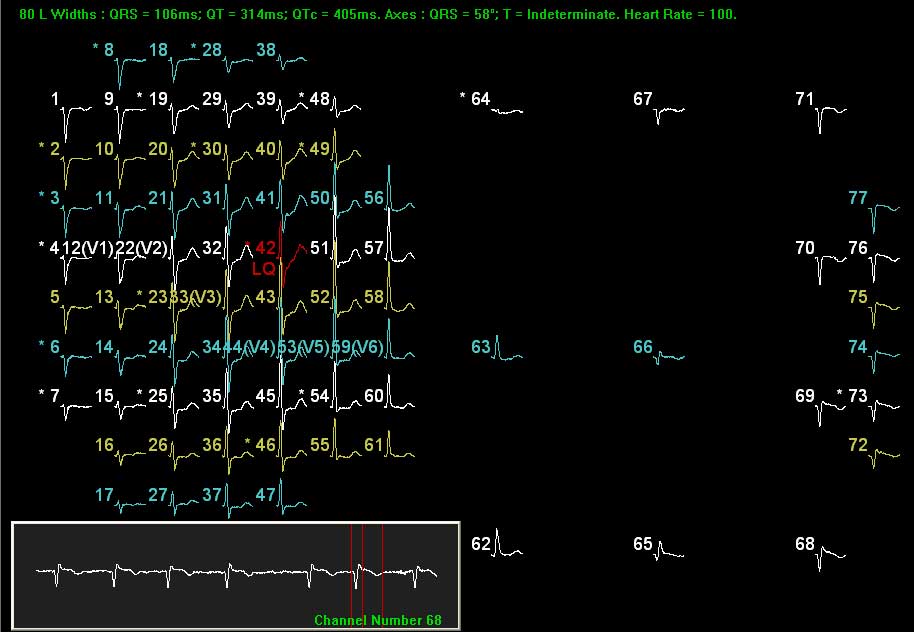
80 lead EKG.

An 80 lead EKG vest was then placed. Shown to the right are the 80 EKG lead tracings displayed individually. The anterior leads are displayed on the left hand side. The posterior or back of the heart leads are displayed on the right hand side of the figure. For instance lead 68 shows ST elevation. Posterior and right-sided leads reveal ST-elevation, where the 12-lead was silent.

In order to display the data in a more clinically relevant and intuitive fashion, the area of injury is shown in red on the patient's back, corresponding to the inferior-posterior location of the MI.
Clinical Application of the 80 Lead EKG
One 80 lead system, the PRIME ECG ® system, is currently approved for use in the US under a 510k.
References
- Self, W.H., Mattu, A., Martin, M., et.al. Body surface mapping in the ED evaluation of the patient with chest pain: use of the 80-lead electrocardiogram system. The American Journal of Emergency Medicine, 2006; 24, pp. 87-112.
- Hatrick, R., Teece, S., Curzen, N., Seeing transient regional myocardial ischaemia through new eyes: a case report, International Journal of Cardiac Interventions, 26/0/05, 17:16:35, 2005.
- Owens, C.G., McClelland, A.J.J., et.al, Pre-hospital 80-lead mapping: Does it add significantly to the diagnosis of acute coronary syndromes? Journal of Electrocardiology, 2004; 37, Supplement pp. 223-232.
- Carley SD, Jones KM, Jenkins M, Darlington E, Farzin FO, Curzen N. A novel method for the detection of transient myocardial ischaemia using body surface electrocardiac mapping. International Journal of Cardiology 2004; 95: 75-81.
- Owens, C.G., McClelland, A.J.J., et.al. Right ventricular Infarction complicating Inferior Myocardial Infarction Correlates with Higher TIMI Risk Scores and Increased Morbidity and Mortality ISCHE, 2004.
- Fermann, G., Comparison of the diagnostic efficacy of an ECG cardiac mapping device to a standard 12-lead, Abstract: American College of Emergency Physicians, 2004.
- O’Neil, B., PRIME Improves Emergency Department Diagnosis and Management in Moderate and High Risk Unstable Angina/NSTEMI Patients, Abstract: American College of Emergency Physicians, 2004.
- Daya, S., Tandri, H., Nasir, K., Chandra, B., Calkins, H., Johns Hopkins School of Medicine, Role of Body Surface Mapping in Evaluation of Patients with Arrhythmogenic Right Ventricular Dysplasia and Right Bundle Branch Block, Abstract: American College of Cardiology, 2004.
- Maynard, S.J., Riddell, J.W., Menown, I.B.A., et.al. Body Surface Mapping Improves Detection of ST Segment Alteration During Percutaneous Coronary Intervention. International Journal of Cardiology 2004; 93, pp. 203-210.
- Menown, I.B.A., Body Surface Mapping; Potential Role in Chest Pain Critical Care Pathway. Critical Pathways in Cardiology 2003; 2, pp. 46-51.
- McClelland, A.J.J., Owens, C.G., Menown, I.B.A., et.al, Comparison of 80-lead Body Surface Mapping Algorithm to Physician and to 12-Lead Electrocardiogram in Detection of Acute Myocardial Infarction, The American Journal of Cardiology, 2003; 92, pp. 252-257.
- Maynard, S.J., Menown, I.B.A., Manoharan, G., et.al. Body Surface Mapping Improves Early Diagnosis of Acute Myocardial Infarction in Patients with Chest Pain and Left Bundle Branch Block, Heart 2003; 89, pp. 998-1002.
- Fermann, G. New diagnostics for acute coronary syndromes. Evolution of diagnostic and treatment options monograph from the 2002 Emergency Medicine Cardiac Research and Education Group symposium in Seattle, Washington; 2003.
- Fox, T.R., Burton, J.H., Strout, T.D., et.al. Time to body surface map acquisition compared with ED 12-lead and right-sided ECG. American Journal of Emergency Medicine 2003; 21(2), pp. 164-165.
- Ornato JP, Menown IB, Riddell JW, et al. 80-lead Body Map Detects Acute ST-elevation Myocardial Infarction Missed by Standard 12-lead Electrocardiography. Journal of the American College of Cardiology 2002; 39(5): 332A.
- Carley S, Mackway-Jones K, Jenkins M, Curzen N. Detection of regional myocardial ischaemia using a novel body surface mapping system: implications for the investigation of myocardial ischaemia. Paper presented at the Faculty of the British Accident and Emergency Society; November 17, 2001; London.
- Menown IB, Allen J, Anderson JM, Adgey AA. ST depression only on the initial 12-lead ECG: early diagnosis of acute myocardial infarction. European Heart Journal 2001; 22, pp. 218–227.
- Fermann G. New diagnostics for acute coronary syndromes. Paper presented at Emergency Medicine Cardiology Research Group International (EMCREG) annual meeting; October 14, 2001; Chicago.
- Carley S, Curzen N, Mackway-Jones K. Isolated evolving right ventricular infarct as seen on PRIME ECGTM body surface mapping system. Paper presented at the PRIME Users Meeting; October 2001; London.
- Menown IB, Allen J, Anderson JM, Adgey AA. Early diagnosis of right ventricular or posterior infarction associated with inferior wall left ventricular acute myocardial infarction. American Journal of Cardiology. 2000; 85: 934–938.
- Menown, I.B.A., Allen, J., Anderson, J. McC., Adgey, A.A.J., Early Diagnosis of Right Ventricular or Posterior Infarction Associated With Inferior Wall Left Ventricular Acute Myocardial Infarction. The American Journal of Cardiology, 2000; 85, pp. 934-938.
- Menown IB, Allen J, Anderson JM, Adgey AA. Noninvasive assessment of reperfusion after fibrinolytic therapy for acute myocardial infarction. American Journal of Cardiology. 2000; 86:736–741.
- Menown, I.B.A., Patterson, R.S.H.W., MacKenzie, G. Adgey, A.A.J., “Body-Surface Map Models for Early Diagnosis of Acute Myocardial Infarction,” Journal of Electrocardiology 1998, Vol. 31, Supplement.
- Menown, I.B.A., McMechan, S.R., Allen, J., Anderson, J., Adgey, A.A.J., Body Surface Mapping and the 12-lead ECG for Non-invasive Assessment of Reperfusion Following Thrombolytic Therapy in Acute Myocardial Infarction. Journal of the American College of Cardiology, February 1998.
- Menown IB, Patterson RS, MacKenzie G, Adgey AA. Body surface vector mapping for early diagnosis of acute myocardial infarction with left bundle branch block. Journal of the American College of Cardiology 1998; 31 (supplement):229.
- Menown IB, Patterson RS, MacKenzie G, Adgey A.A. Body surface mapping and the 12-lead ECG for non-invasive assessment of reperfusion following thrombolytic therapy in acute myocardial infarction. Journal of the American College of Cardiology. 1998; 31 (supplement):137.
- Menown, I.B.A., MacKenzie, G., Patterson, R.S.H.W., et.al. Limits to the 12-lead electrocardiographic diagnosis of acute myocardial infarction: can we improve on ST segment elevation? Journal of the American College of Cardiology 1998; 31(2), 446A.
- McMechan, S.R., MacKenzie, G., Allen, J., et.al. Body Surface ECG Potential Maps in Acute Myocardial Infarction. Journal of Electrocardiology 1995 (28), pp. 184-190.
- McMechan, S.R., Cullen, C.M., MacKenzie, G., et.al. Discriminate function analysis of body surface potential maps in acute myocardial infarction. Journal of Electrocardiology 1994; 27, pp. 117-120. Related Material
- Boie, E.T. Initial Evaluation of Chest Pain. Emergency Medicine Clinics of North America 2005; 23, pp. 937-957.
- American Heart Association, 2005 Heart and Stroke Statistical Update, 2005.
- Vesterinen, P., Hanninen, H., Karvonen, M., et.al. Spatial repolarization abnormalities in old myocardial infarction. Journal of Electrocardiology 2005; 38, pp. 264-270.
- Gersh, B., Stone, G., White, H., et.al. Pharmacological facilitation of primary PCI for AMI: is the slope of the curve the shape of the future? JAMA 2005; 298:980.
- Antman, E.M., Anbe, D.T., Armstrong, P.W., et.al. ACC/AHA Guidelines for the management of patients with ST-elevation myocardial infarction – executive summary. Journal of the American College of Cardiology 2004; 44(3), pp. 671-719.
- Terkelsen, C.J., Lassen, J.F., Norgaard, B.L., et.al. Mortality rtaes in patients with ST-elevation vs. non-ST-elevation acute myocardial infarction; observations from an unselected cohort. European Heart Journal 2004; 26 (1), pp. 18-26.
- Hanninen, H., Takala, P., Tantonen, J., et.al. ST-T integral and T-wave amplitude in detection of exercise-induced myocardial ischemia evaluated with body surface potential mapping. Journal of Electrocardiology 2003; 36(2), pp. 89-98.
- Fox, K.A., Goodman, S.J., Anderson, F.A., et.al. From guidelines to clinical practice: the impact of hospital and geographical characteristics on temporal trends in the management of acute coronary syndromes. European Heart Journal 2003; 24(15), pp. 1414-1424.
- Mahoney, E.M., et.al. Cost and cost-effectiveness of an Early Invasive vs. Conservative Strategy for the treatment of Unstable Angina and Non-ST-Segment Elevation Myocardial Infarction. JAMA 2002; 288 (15), pp. 1851-1858.
- Goldman BU, Christenson RH, Hamm CW, Meinertz T, Ohman EM. Implications of troponin testing in clinical medicine. Curr Control Trials Cardiovascular Medicine 2001; 2:75–84.
- Cannon, C.P., Gibson, C.M., Lambrew, C.T., et.al. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA 2000; 283, pp. 2941-2947.
- Menown, I.B.A., MacKenzie, G., Adgey, A.A.J., “Optimizing the initial 12-lead electrocardiographic diagnosis of acute myocardial infarction.” European Heart Journal, 2000; 21:275–283.
- Pope JH, Aufderheide TP, Ruthazer R, et al. Missed diagnoses of acute cardiac ischemia in the emergency department. New England Journal of Medicine 2000; 342:1163–1170.
- Mehta RH, Eagle KA. Editorial: Missed diagnoses of acute coronary syndromes in the emergency room—continuing challenges. New England Journal of Medicine 2000; 342:1207–1210.
- Ryan TJ, Antman EM, Brooks NH, et al. ACC/AHA guidelines for the management of patients with acute myocardial infarction: 1999 update: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Acute Myocardial Infarction). Available at: http://www.acc.org/clinical guidelines/ and http://www.americanheart.org. Accessed October 10, 2000.
- McCarthy BD, Beshansky JR, D’Agostino RB, Selker HP. Missed diagnosis of acute myocardial infarction in the emergency department: results from a multicenter study. Annals of Emergency Medicine 1993; 22: 579–582. Cited by: Mehta RH, Eagle KA. Editorial: Missed diagnoses of acute coronary syndromes in the emergency room—continuing challenges, New England Journal of Medicine 2000; 342:1207–1210.
- Canto JG, Shlipak MG, Rogers WJ, et al. Prevalence, clinical characteristics, and mortality among patients with myocardial infarction presenting without chest pain. JAMA 2000; 283:3223–3229.
- Berger, P.B., Ellis, S.G., Holmes, D.R., et.al. Relationship between delay in performing direct coronary angioplasty and early clinical outcome in patients with acute myocardial infarction (GUSTO-IIb). Circulation 1999; 100, pp. 14-20.
- Kornreich F. Identification of best electrocardiographic leads for diagnosing acute myocardial ischaemia. Journal of Electrocardiology 1998; 31(supplement):157–163.
- Zalenski RJ, Rydman RJ, Ting S, et al. A National Survey of Emergency Department Chest Pain Centers in the United States. American Journal of Cardiology 1998; Vol. 81.
- Taccardi, B., Punske, B.B., Lux, R.L., MacLeod, R.S., Ershler, P.R., Dustman, T.J., Vyhmeister, Y., “Useful Lessons from Body Surface Mapping,” Journal of Cardiovascular Electrophysiology, Vol. 9, No. 7, 1998.
- Dracup K, Moser DK. Treatment-seeking behavior among those with signs and symptoms of acute myocardial infarction. Heart Lung 1991; 20 (5 pt 2):570–575. Cited by: National Heart, Lung, and Blood Institute. Educational Strategies to Prevent Prehospital Delay. NHLBI 1997; NIH Pub. No.97-3787.
- National Heart, Lung, and Blood Institute. An evaluation of technologies for identifying acute cardiac ischemia in the emergency department: a report from a National Heart Attack Alert Program working group. Annals of Emergency Medicine 1997; 29:13–87.
- Timm TC, Ross R, McKendall GR, Braunwald E, Williams DO, and the TIMI Investigators. Left ventricular function and early cardiac events as a function of time to treatment with t-PA: a report from TIMI II [abstract]. Circulation 1991; 84(4 supplement): II, p.230. Cited by: National Heart, Lung, and Blood Institute. Educational Strategies to Prevent Prehospital Delay. NHLBI 1997; NIH Pub. No.97-3787.
- National Heart, Lung, and Blood Institute. Educational Strategies to Prevent Prehospital Delay. NHLBI 1997; NIH Pub. No. 97-3787.
- Peberdy, M.A., Ornato, J.P., “Improving Triage of Patients with Chest Pain,” Contemporary Internal Medicine 1997; 9(3).
- ACC/AHA Practice Guidelines for the Management of Patients with Acute Myocardial Infarction, Journal of the American College of Cardiology 1996; 28(5), 1996.
- Mair J, Smidt J, Lechleitner P, Dienstl F, Puschendorf B. A decision tree for the early diagnosis of acute myocardial infarction in nontraumatic chest pain patients at hospital admission. Chest 1995; 108:1502–1509.
- The World Market for Cardiovascular Products, Clinica Reports 1995.
- National Institutes of Health, Rapid Identification and Treatment of Patients with Acute Myocardial Infarction 1995.
- Green, L.S., Abildskov, J.A., “Clinical Applications of Body Surface Mapping,” Clinical Cardiology 1995; 18.
- Emergency department: rapid identification and treatment of patients with acute myocardial infarction. NHLBI 1995; NIH Pub. No. 95-3278.
- Rogers WJ, Bowlby LJ, Chandra NC, et al, for the participants in the National Registry of Myocardial Infarction. Treatment of myocardial infarction in the United States (1990–1993). Observations from the National Registry of Myocardial Infarction. Circulation 1994; 90:2103-2114.
- Adams, J., Trent, R., Rawles, J., “Earliest electrocardiographic evidence of myocardial infarction: implications for thrombolytic treatment,” British Medical Journal 1993.
- Kornreich F, Montague TJ, Rautaharju PM. Body surface potential mapping of ST segment changes in acute myocardial infarction. Implications for ECG enrollment criteria for thrombolytic therapy. Circulation 1993; 87:773-82.
- American Heart Association/Emergency Cardiac Care Committee and Subcommittees. Guidelines for cardiopulmonary resuscitation and emergency cardiac care, III: adult advanced cardiac life support. JAMA 1992; 268(16), pp. 2199–2241. Cited by: National Heart Attack Alert Program Coordinating Committee, 60 Minutes to Treatment Working Group.
- Pardee HEB. An electrocardiographic sign of coronary artery obstruction. Archives of Internal Medicine 1920; 26: 244–257.