Uveitis pathophysiology
|
Uveitis Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Uveitis pathophysiology On the Web |
|
American Roentgen Ray Society Images of Uveitis pathophysiology |
|
Risk calculators and risk factors for Uveitis pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Tarek Nafee, M.D. [2]
Overview
The exact pathogenesis of uveitis is not fully understood. It is thought that uveitis is mediated by a genetic predisposition and an acquired cross immunity to infectious agents, or cross immunity to self-antigens due to underlying autoimmune diseases. From 35% up to 50% of cases of uveitis are idiopathic.[1][2]Development of uveitis is hypothesized to be the result of a genetic predisposition for acquiring the disease. Contributions of several Human Leukocyte Antigen (HLA) alleles are most commonly implicated.[2][3]
Pathogenesis
The exact pathogenesis of uveitis is not fully understood. It is thought that uveitis is mediated by a genetic predisposition combined with cross immunity to infectious agents, or cross immunity to self-antigens due to underlying autoimmune diseases. Up to 35% of cases of uveitis are idiopathic.[1][2] Uveitis, in the setting of underlying infectious diseases, is hypothesized to be secondary to a T-cell mediated hypersensitivity reaction resulting in immunoactivating cytokine production by proliferating Tн17 and Tн1 cells.[3][4] A similar mechanism is hypothesized for autoimmune etiologies of uveitis with the exception of an unknown source of the triggering antigen.[5][6][7][8]
Genetics
Development of uveitis is hypothesized to be the result of a genetic predisposition for acquiring the disease. Contributions of several Human Leukocyte Antigen (HLA) alleles are most commonly implicated. This includes, HLA-B27 in seronegative spondyloarthropathies, HLA-A29 in birdshot chorioretinopathy, HLA-B51 in Behcet syndrome and multiple sclerosis, HLA-B8, HLA-DR15, and HLA-DR2.[2][3]
Associated Conditions
The following conditions are associated with uveitis:[1][2][9]
- Seronegative spondyloarthropathy
- Sarcoidosis
- Multiple sclerosis
- Inflammatory bowel disease
- Systemic lupus erythematosus (SLE)
- Behçet's syndrome
- Birdshot retinochoroidopathy
- Juvenile Idiopathic Arthritis (JIA)
- Vogt-Koyanagi-Harada Syndrome
- Fuch's heterochromic iridocyclitis
- Lymphoma
- Lyme Disease
- Acquired immunodeficiency syndrome (AIDS)
- Herpes simplex
- Varicella Zoster
- Cytomegalovirus
- Syphilis
- Toxoplasmosis
- Toxocariasis
- Tuberculosis
- Rubella
- Cat scratch disease (Bartonella spp.)
Gross Pathology
The following are images of the gross pathology of uveitis:[10][11]
-
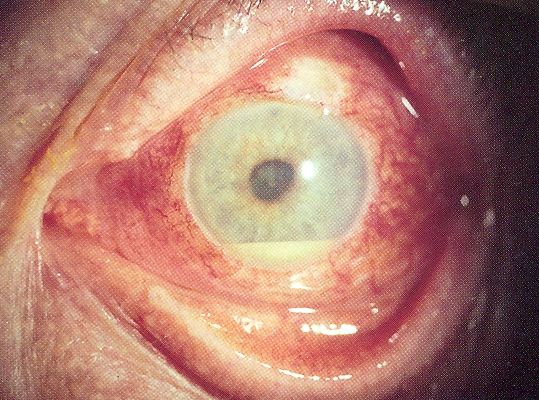
Uveitis with pus in the anterior chamber
-
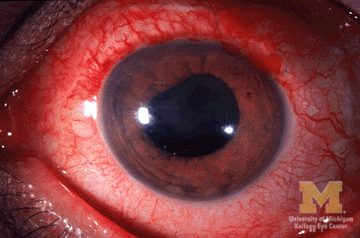
Anterior Uveitis


Microscopic Pathology
The following are images of the microscopic pathology of uveitis:[12]
-
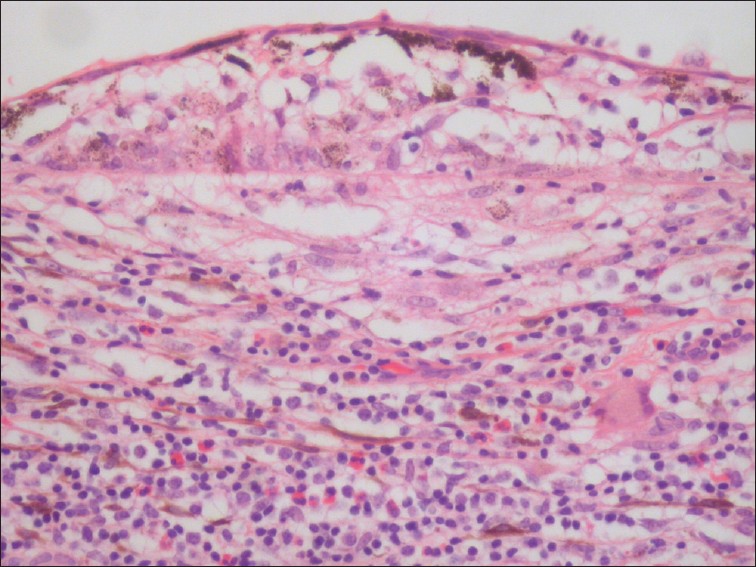
Uveitis with infiltration of lymphocytes
-
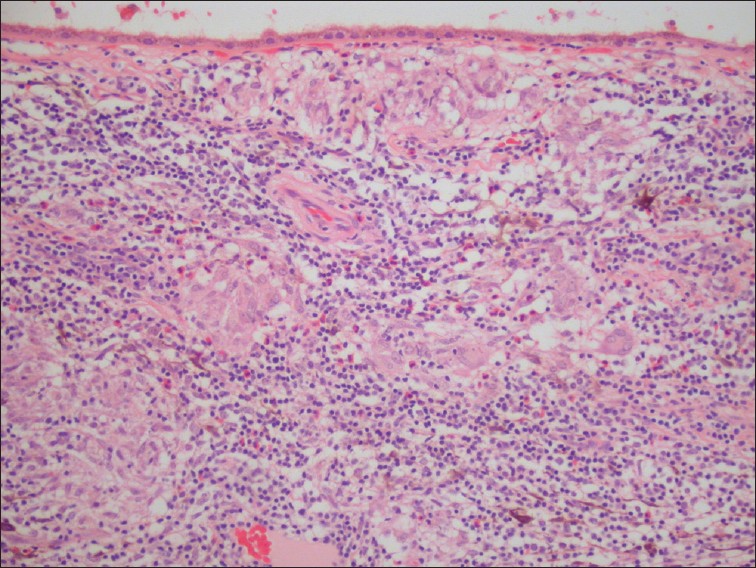
Uveitis with granulomatous inflammation and infiltration of the choroid by lymphocytes and macrophages.


References
- ↑ 1.0 1.1 1.2 Rodriguez A, Calonge M, Pedroza-Seres M, Akova YA, Messmer EM, D'Amico DJ; et al. (1996). "Referral patterns of uveitis in a tertiary eye care center". Arch Ophthalmol. 114 (5): 593–9. PMID 8619771.
- ↑ 2.0 2.1 2.2 2.3 2.4 Guly CM, Forrester JV (2010). "Investigation and management of uveitis". BMJ. 341: c4976. doi:10.1136/bmj.c4976. PMID 20943722.
- ↑ 3.0 3.1 3.2 Przeździecka-Dołyk J, Węgrzyn A, Turno-Kręcicka A, Misiuk-Hojło M (2016). "Immunopathogenic Background of Pars Planitis". Arch Immunol Ther Exp (Warsz). 64 (2): 127–37. doi:10.1007/s00005-015-0361-y. PMC 4805694. PMID 26438050.
- ↑ Urban B, Bakunowicz-Łazarczyk A, Michalczuk M (2014). "Immune recovery uveitis: pathogenesis, clinical symptoms, and treatment". Mediators Inflamm. 2014: 971417. doi:10.1155/2014/971417. PMC 4096001. PMID 25089078.
- ↑ Sun D, Liang D, Kaplan HJ, Shao H (2015). "The role of Th17-associated cytokines in the pathogenesis of experimental autoimmune uveitis (EAU)". Cytokine. 74 (1): 76–80. doi:10.1016/j.cyto.2014.12.017. PMC 4457592. PMID 25742774.
- ↑ Bi HS, Liu ZF, Cui Y (2015). "Pathogenesis of innate immunity and adaptive immunity in the mouse model of experimental autoimmune uveitis". J Chin Med Assoc. 78 (5): 276–82. doi:10.1016/j.jcma.2015.01.002. PMID 25769932.
- ↑ Horai R, Caspi RR (2011). "Cytokines in autoimmune uveitis". J Interferon Cytokine Res. 31 (10): 733–44. doi:10.1089/jir.2011.0042. PMC 3189550. PMID 21787221.
- ↑ Ke Y, Liu K, Huang GQ, Cui Y, Kaplan HJ, Shao H; et al. (2009). "Anti-inflammatory role of IL-17 in experimental autoimmune uveitis". J Immunol. 182 (5): 3183–90. doi:10.4049/jimmunol.0802487. PMC 3275433. PMID 19234216.
- ↑ American Academy of Ophthalmology EyeWiki(2015)http://eyewiki.aao.org/Category:Uveitis
- ↑ Wikipedia Uveitis(2006)https://en.wikipedia.org/wiki/Uveitis#/media/File:Hypopyon.jpg
- ↑ University of Michigan Eyes Have It(2009)http://kellogg.umich.edu/theeyeshaveit/red-eye/anterior-uveitis.html
- ↑ Arevalo JF, Garcia RA, Al-Dhibi HA, Sanchez JG, Suarez-Tata L (2012). "Update on sympathetic ophthalmia". Middle East Afr J Ophthalmol. 19 (1): 13–21. doi:10.4103/0974-9233.92111. PMC 3277011. PMID 22346110.
{kind=link}