Radial artery catheterization: Difference between revisions
No edit summary |
No edit summary |
||
| Line 69: | Line 69: | ||
==Performance of the [[Allen Test]] Before the Procedure== | ==Performance of the [[Allen Test]] Before the Procedure== | ||
The hand is normally supplied by blood from the ulnar and radial arteries. The arteries undergo [[anastomosis]] in the hand. Thus, if the blood supply from one of the arteries is cut off, the other artery can supply adequate blood to the hand. A minority of people lack this dual blood supply. An [[Allen Test]] should be performed before the procedure to confirm that there is sufficient blood flow in the [[ulnar artery]] should there be a loss of patency in the [[radial artery]] due to either thrombosis or spasm which can result in gangrenous finger or had loss. This test is named after [[Edgar Van Nuys Allen]].<ref>{{WhoNamedIt|synd|189}}</ref> | The hand is normally supplied by blood from the ulnar and radial arteries. The arteries undergo [[anastomosis]] in the hand. Thus, if the blood supply from one of the arteries is cut off, the other artery can supply adequate blood to the hand. A minority of people lack this dual blood supply. An [[Allen Test]] should be performed before the procedure to confirm that there is sufficient blood flow in the [[ulnar artery]] should there be a loss of patency in the [[radial artery]] due to either thrombosis or spasm which can result in gangrenous finger or had loss. People who have a single blood supply in one hand often have a dual supply in the other, allowing the practitioner to take blood from the side with dual supply. This test is named after [[Edgar Van Nuys Allen]].<ref>{{WhoNamedIt|synd|189}}</ref> | ||
The utility of the Allen's test has been questioned,<ref name="pmid11081899">{{cite journal |author=Jarvis MA, Jarvis CL, Jones PR, Spyt TJ |title=Reliability of Allen's test in selection of patients for radial artery harvest |journal=Ann. Thorac. Surg. |volume=70 |issue=4 |pages=1362–5 |year=2000 |month=October |pmid=11081899 |doi= |url=http://linkinghub.elsevier.com/retrieve/pii/S0003-4975(00)01551-4}}</ref> and no direct association with ischemic complications of radial artery cannulation have ever been demonstrated. In 1983, Slogoff and colleagues reviewed 1,782 radial artery cannulations and found that 25% of them resulted in complete radial artery occlusion, without apparent adverse effects.<ref>Slogoff s, Keats AS, Arlund C. On the safety of radial artery cannulation. Anesthesiology 1983; 59:42-7</ref> A number of reports have been published in which permanent ischemic sequelae occurred even in the presence of a normal Allen's test.<ref>Thompson SR, Hirschberg A: Allen's test re-examined. Crit Care Med 16:915, 1988</ref><ref>Wilkins RG: Radial artery cannulation and ischaemic damage: A review. Anaesthesia 40:896-899, 1985</ref> In addition, the results of Allen's tests do not appear to correlate with distal blood flow as demonstrated by fluorescein dye injections<ref>McGregor AD: The Allen test-an investigation of its accuracy by fluorescein angiography. J Hand Surg [Br] 12:82-85, 1987</ref> or photoplethysmography.<ref>Stead SW, Stirt JA: Assessment of digital blood flow and palmar collateral circulation. Int J Clin Monit Comput 2:29, 1985</ref> | |||
Modifications to the test have been proposed to improve reliability.<ref name="pmid17643672">{{cite journal |author=Asif M, Sarkar PK |title=Three-digit Allen's test |journal=Ann. Thorac. Surg. |volume=84 |issue=2 |pages=686–7 |year=2007 |month=August |pmid=17643672 |doi=10.1016/j.athoracsur.2006.11.038 |url=http://linkinghub.elsevier.com/retrieve/pii/S0003-4975(06)02283-1}}</ref> | |||
Despite this lack of association with outcomes, the Allen Test is often performed in clinical practice. | |||
=== How to Perform The Allen Test === | === How to Perform The Allen Test === | ||
| Line 84: | Line 90: | ||
If color does not return or returns after 7 seconds, then the ulnar artery supply to the hand is not sufficient and the radial artery therefore cannot be safely cannulated. | If color does not return or returns after 7 seconds, then the ulnar artery supply to the hand is not sufficient and the radial artery therefore cannot be safely cannulated. | ||
Revision as of 18:21, 23 February 2010
Editors-in-Chief: C. Michael Gibson, M.S., M.D.,
Advantages of the Radial Approach to Cardiac Catheterization
- Reduced bleeding
- Early patient ambulation
- Greater patient satisfaction
- Absence of retroperitoneal hematomas, femoral pseudo aneurysms, arterial / venous fistulas
- Reduced length of stay
In a meta-analysis of publications from 1980 to 2008, radial artery catheterization was associated with a 73% relative risk reduction in the risk of major bleeding (2.3% vs 0.05%, p<0.001) compared to femoral access. While the risk of the composite endpoint of death, myocardial infarction (MI) and stroke tended to be less frequent among patients undergoing radial artery catheterization (3.8% vs 2.5%, p = .058), there was no difference in mortality alone. Radial artery access also was associated with a 0.4% reduction in length of stay (p=0.001).[1]
Potential Pitfalls of the Radial Approach to Cardiac Catheterization
- Spasm
- Vessel tortuosity
- Guide catheter support may be reduced
- Loss of radial artery pulse in 4% of cases
- Potential increase in the duration of the procedure and fluroscopy time
Radial Artery Anatomy
In the Forearm
- Radial recurrent artery - arises just after the radial artery comes off the brachial artery. It travels superiorly to anastomose with the radial collateral artery.
- Palmar carpal branch of radial artery - a small vessel which arises near the lower border of the pronator quadratus
- Superficial palmar branch of the radial artery - arises from the radial artery, just where this vessel is about to wind around the lateral side of the wrist.
At the Wrist
- Dorsal carpal branch of radial artery - a small vessel which arises beneath the extensor tendons of the thumb
- First dorsal metacarpal artery - arises just before the radial artery passes between the two heads of the first dorsal interosseous muscle and divides almost immediately into two branches which supply the adjacent sides of the thumb and index finger; the lateral side of the thumb receives a branch directly from the radial artery.
In the Hand
- Princeps pollicis artery - arises from the radial artery just as it turns medially to the deep part of the hand.
- Radialis indicis - arises close to the princeps pollicis. The two arteries may arise from a common trunk, the first palmar metacarpal artery.
- Deep palmar arch - terminal part of radial artery.
Additional images
-
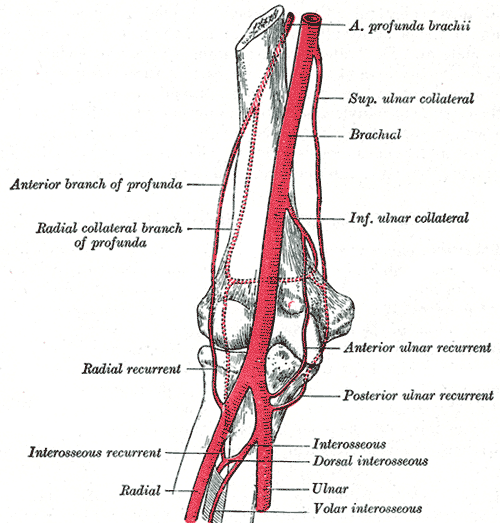
Diagram of the anastomosis around the elbow-joint.
-
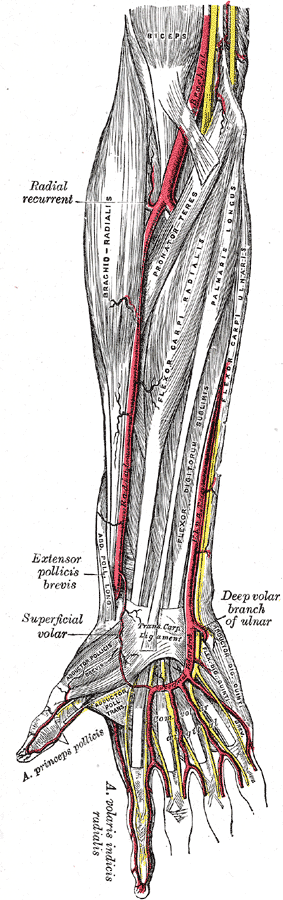
The radial and ulnar arteries.
-
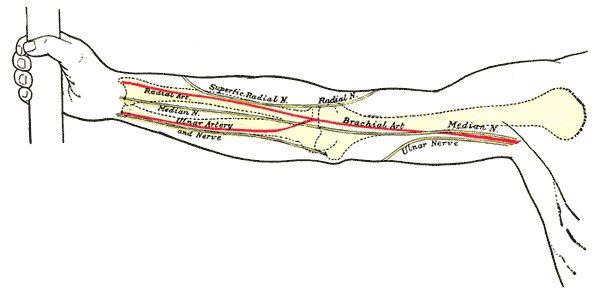
Front of right upper extremity, showing surface markings for bones, arteries, and nerves.
-
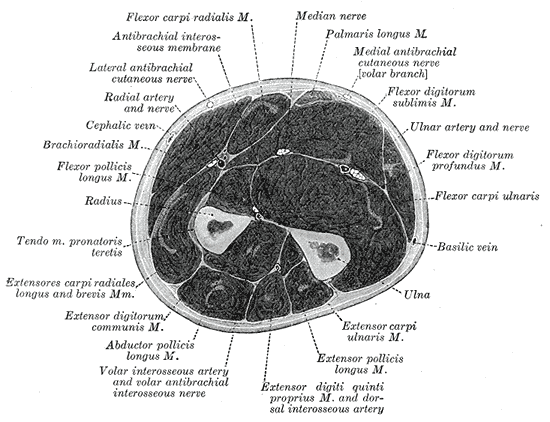
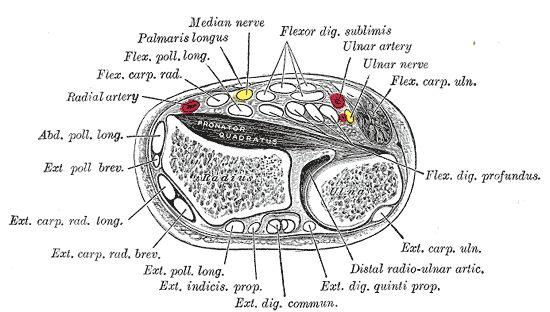
Cross-section through the middle of the forearm.
-
Transverse section across distal ends of radius and ulna.
-
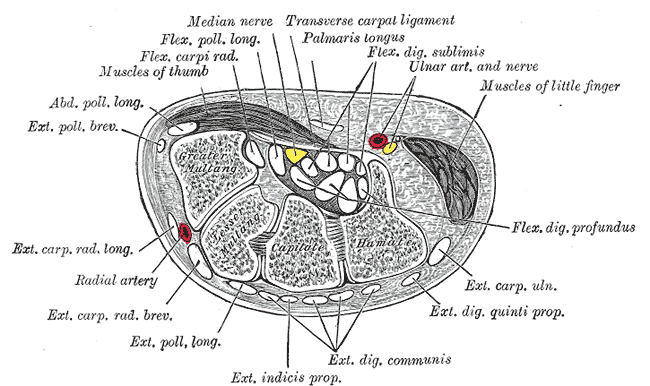
Transverse section across the wrist and digits.





Contraindications to Utilization of the Radial Approach to Cardiac Catheterization
- Cellulitis or other infections over the radial artery
- Absence of palpable radial artery pulse
- Positive Allen test (see below), indicating that only one artery supplies the hand
- Coagulation defects (relative)
Performance of the Allen Test Before the Procedure
The hand is normally supplied by blood from the ulnar and radial arteries. The arteries undergo anastomosis in the hand. Thus, if the blood supply from one of the arteries is cut off, the other artery can supply adequate blood to the hand. A minority of people lack this dual blood supply. An Allen Test should be performed before the procedure to confirm that there is sufficient blood flow in the ulnar artery should there be a loss of patency in the radial artery due to either thrombosis or spasm which can result in gangrenous finger or had loss. People who have a single blood supply in one hand often have a dual supply in the other, allowing the practitioner to take blood from the side with dual supply. This test is named after Edgar Van Nuys Allen.[2]
The utility of the Allen's test has been questioned,[3] and no direct association with ischemic complications of radial artery cannulation have ever been demonstrated. In 1983, Slogoff and colleagues reviewed 1,782 radial artery cannulations and found that 25% of them resulted in complete radial artery occlusion, without apparent adverse effects.[4] A number of reports have been published in which permanent ischemic sequelae occurred even in the presence of a normal Allen's test.[5][6] In addition, the results of Allen's tests do not appear to correlate with distal blood flow as demonstrated by fluorescein dye injections[7] or photoplethysmography.[8]
Modifications to the test have been proposed to improve reliability.[9]
Despite this lack of association with outcomes, the Allen Test is often performed in clinical practice.
How to Perform The Allen Test
1) The hand is elevated and the patient/person is asked to make a fist for about 30 secs.
2) Pressure is applied over the ulnar and the radial arteries so as to occlude both of them.
3) Still elevated, the hand is then opened. It should appear blanched (pallor can be observed at the finger nails).
4) Ulnar pressure is released and the color should return in 7 secs.
Inference: Ulnar artery supply to the hand is sufficient and it is safe to cannulate the radial artery
If color does not return or returns after 7 seconds, then the ulnar artery supply to the hand is not sufficient and the radial artery therefore cannot be safely cannulated.
Choosing the Left or Right Side for the Radial Approach
If the internal mammary artery must be canulated, then the left radial artery should be used.
Obtaining Radial Access
Initial Insertion of the Catheters
To reduce spasm, 500 micrograms of diltiazem can be administered via the sidearm prior to insertion of the right and left sided catheters.
Catheter selection
Many operators choose to start with the right coronary artery as the right sided catheter may allow for directing the wire as you make your way up around the arch. Once the wire is around the arch, it should remain there for exchanges. A JL 3.5 catheter may be used to engage the left coronary artery when catheterization is performed from the right arm.
References:
- ↑ Jolly SS, Amlani S, Hamon M, Yusuf S, Mehta SR (2009). "Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: a systematic review and meta-analysis of randomized trials". American Heart Journal. 157 (1): 132–40. doi:10.1016/j.ahj.2008.08.023. PMID 19081409. Retrieved 2010-02-23. Unknown parameter
|month=ignored (help) - ↑ Template:WhoNamedIt
- ↑ Jarvis MA, Jarvis CL, Jones PR, Spyt TJ (2000). "Reliability of Allen's test in selection of patients for radial artery harvest". Ann. Thorac. Surg. 70 (4): 1362–5. PMID 11081899. Unknown parameter
|month=ignored (help) - ↑ Slogoff s, Keats AS, Arlund C. On the safety of radial artery cannulation. Anesthesiology 1983; 59:42-7
- ↑ Thompson SR, Hirschberg A: Allen's test re-examined. Crit Care Med 16:915, 1988
- ↑ Wilkins RG: Radial artery cannulation and ischaemic damage: A review. Anaesthesia 40:896-899, 1985
- ↑ McGregor AD: The Allen test-an investigation of its accuracy by fluorescein angiography. J Hand Surg [Br] 12:82-85, 1987
- ↑ Stead SW, Stirt JA: Assessment of digital blood flow and palmar collateral circulation. Int J Clin Monit Comput 2:29, 1985
- ↑ Asif M, Sarkar PK (2007). "Three-digit Allen's test". Ann. Thorac. Surg. 84 (2): 686–7. doi:10.1016/j.athoracsur.2006.11.038. PMID 17643672. Unknown parameter
|month=ignored (help)