Aortic arch anomalies CT
|
Aortic arch anomalies Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Aortic arch anomalies CT On the Web |
|
American Roentgen Ray Society Images of Aortic arch anomalies CT |
|
Risk calculators and risk factors for Aortic arch anomalies CT |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Associate Editor-In-Chief: Cafer Zorkun, M.D., Ph.D. [2] Keri Shafer, M.D. [3] Priyamvada Singh, MBBS [[4]]
Assistant Editor-In-Chief: Kristin Feeney, B.S. [[5]]
CT
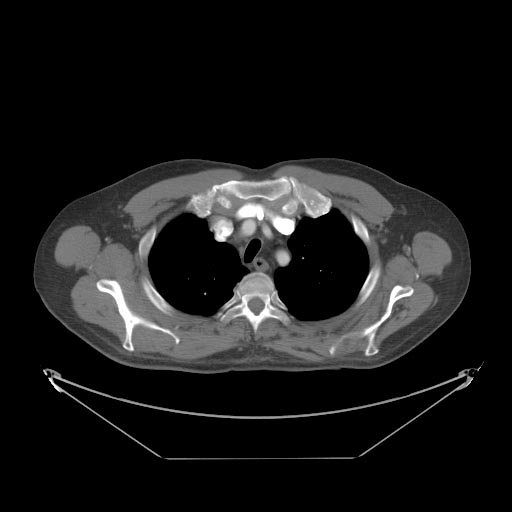
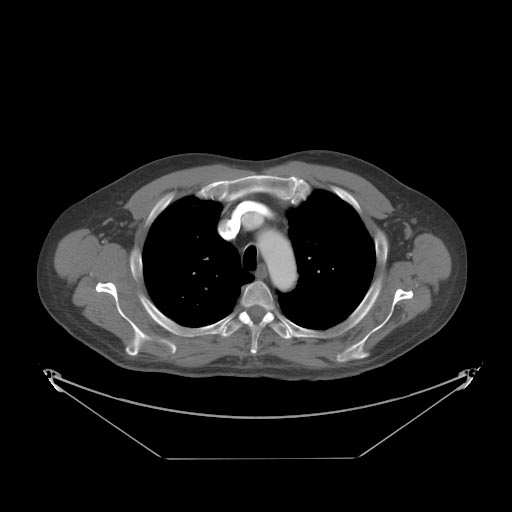
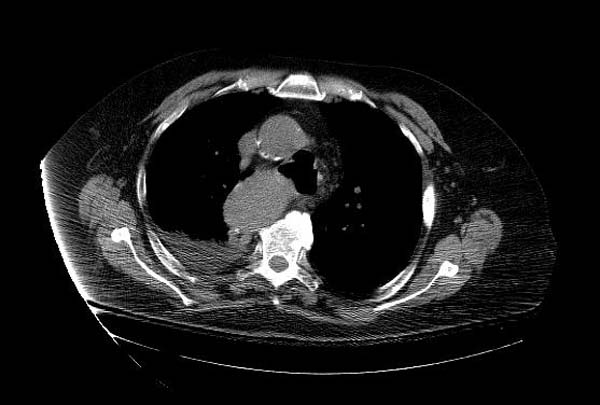
Computed tomography can be used as a diagnostic tool to show the relationship of the aortic arches to the trachea and esophagus and also the degree of tracheal narrowing. Bronchoscopy can be useful in internally assessing the degree of tracheomalacia.
Imaging Findings
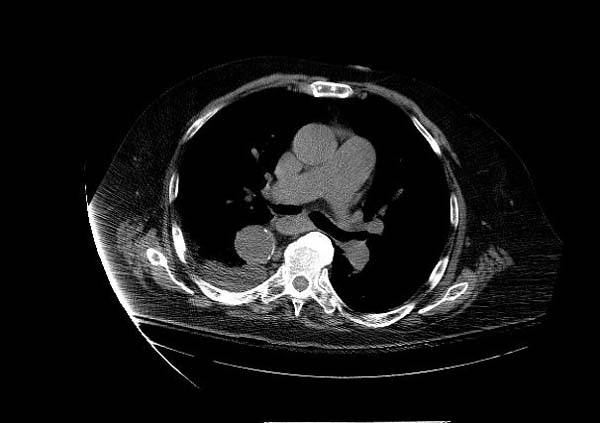
Classification: Double aortic arch Case: A chest CT was performed in the arterial phase. A diagram of the findings is seen. The left common carotid artery arose from the ascending aorta. The aortic arch was to the right of the trachea, and passed posterior to it. The right common carotid and right subclavian arteries arose from the arch in that order. From the posterior arch, the left subclavian artery arose from a large diverticulum (this corresponds to the left “aortic knuckle” seen on the PA film). The descending aorta then crossed to the right again before passing through the diaphragm in the midline. This appearance may be due to right aortic arch with aberrant left subclavian artery, or to double aortic arch with atresia of the left arch, subtype 3. This case is more likely to be the former, as there was no narrowing of the trachea, and subtype 3 double aortic arch is rare. The anatomic difference between these two anomalies is persistence or not of an atretic segment of the left arch.

Classification: Bovine arch Case: A multi-slice CT was performed to deteremine the relationship of the aortic arches.
-
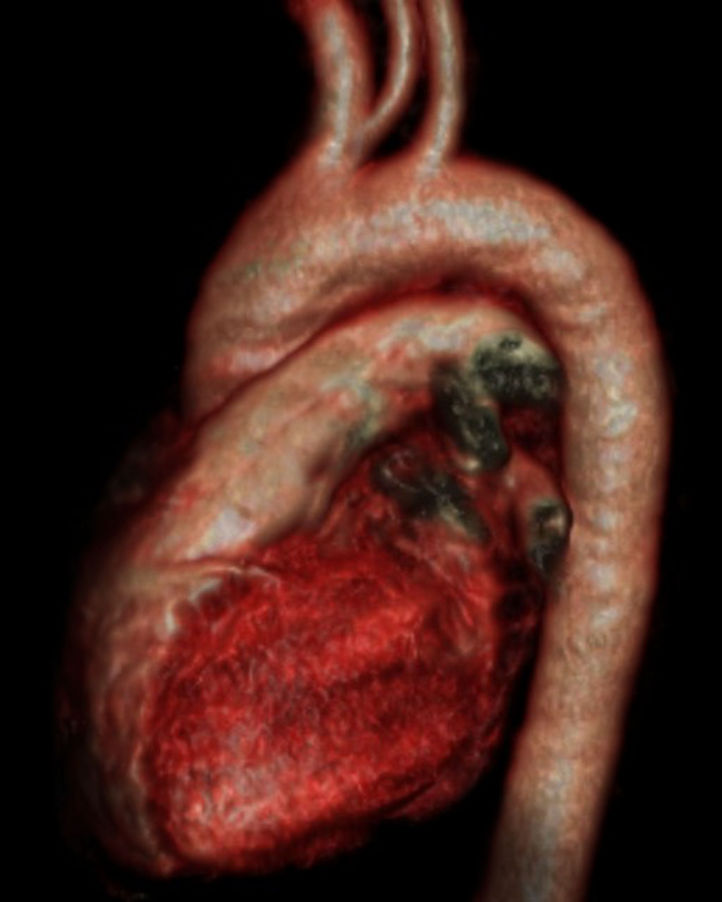
Bovine arch
-

MSCT: Bovine arch
-
MSCT: Bovine arch
-

MSCT: Bovine arch
-

MSCT: Bovine arch
-
MSCT: Bovine arch
-
File:'''Case:''' A multi-slice CT was performed to deteremine the relationship of the aortic arches.
-
Right Aortic Arch
-
Right Aortic Arch








References
Additional Reading
- Moss and Adams' Heart Disease in Infants, Children, and Adolescents Hugh D. Allen, Arthur J. Moss, David J. Driscoll, Forrest H. Adams, Timothy F. Feltes, Robert E. Shaddy, 2007 ISBN 0781786843
- Hurst's the Heart, Fuster V, 12th ed. 2008, ISBN 978-0-07-149928-6
- Willerson JT, Cardiovascular Medicine, 3rd ed., 2007, ISBN 978-1-84628-188-4
External Links
Acknowledgements
The content on this page was first contributed by: C. Michael Gibson, M.S., M.D.