Blunt splenic trauma
Overview
Since the 1990s, the management of blunt splenic trauma injuries has changed significantly. In the past, routine splenectomy was the mainstay for both evaluation and treatment of most splenic injuries. With new research and new technology, the routine splenectomy is no longer policy. For the majority of cases, a switch to nonoperative management is now preferred.
Diagnosis
A CT scan grading criteria was created to identify the need for intervention (surgery or embolization) in patients with splenic injury. The criteria were established using 20 CT scans from a database of hemodynamically stable patients with blunt splenic injury. These criteria were then validated in 56 consecutive patients retrospectively and appear to reliably predict the need for invasive management in patients with blunt injury to the spleen (sensitivity of 100%, specificity 88%, overall accuracy was 93%).[1]
The study suggested that the following three CT findings correlate with the need for intervention:
- Devascularization or laceration involving 50% or more of the splenic parenchyma
- Contrast blush greater than one centimeter in diameter (from active extravasation of IV contrast or pseudoaneurysm formation
- A large hemoperitoneum.
-
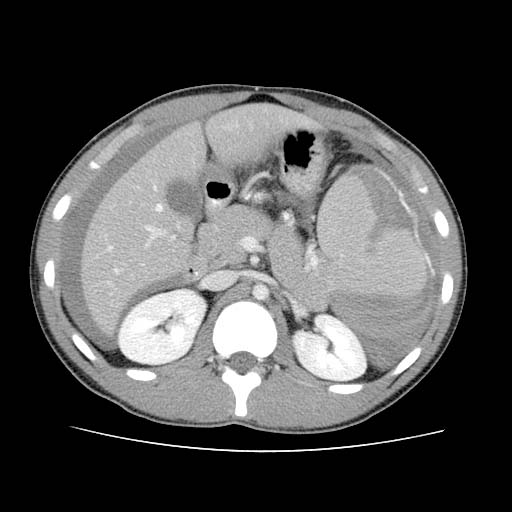 Splenic laceration Image courtesy of RadsWiki and copylefted
Splenic laceration Image courtesy of RadsWiki and copylefted -
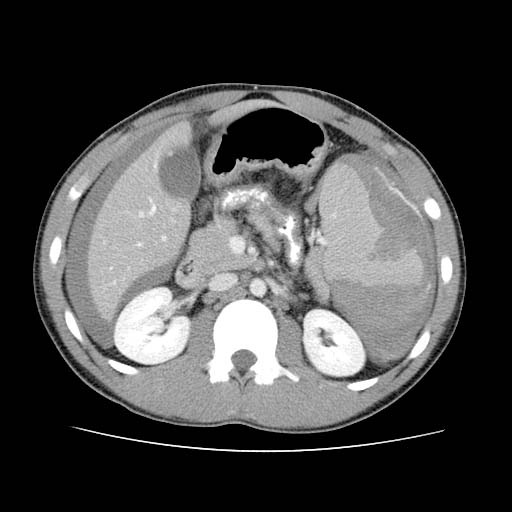 Splenic laceration Image courtesy of RadsWiki and copylefted
Splenic laceration Image courtesy of RadsWiki and copylefted -
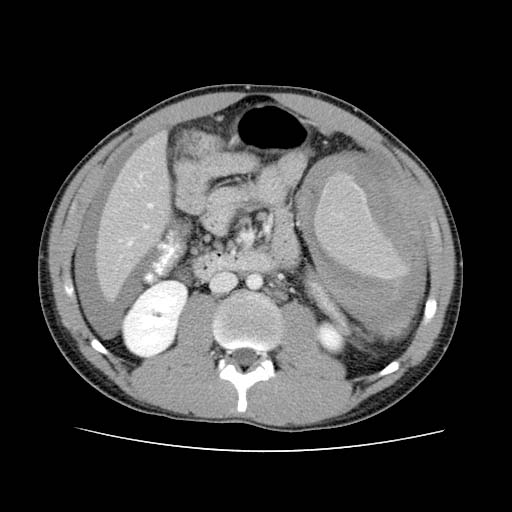 Splenic laceration Image courtesy of RadsWiki and copylefted
Splenic laceration Image courtesy of RadsWiki and copylefted



Treatment
A recent retrospective review of 648 patients admitted with the diagnosis of blunt splenic injury to a Level I trauma center reported that splenic embolization has offered increased use of nonoperative management and higher salvage rates for American Association for the Surgery of Trauma splenic injury grades when compared with prior studies. [2]
References
- ↑ Thompson BE, Thompson BT, Munera F; et al. (2006). "Novel computed tomography scan scoring system predicts the need for intervention after splenic injury". The Journal of trauma. 60 (5): 1083–6. doi:10.1097/01.ta.0000218251.67141.ef. PMID 16688074.
- ↑ Haan JM, Bochicchio GV, Kramer N, Scalea TM (2005). "Nonoperative management of blunt splenic injury: a 5-year experience". The Journal of trauma. 58 (3): 492–8. PMID 15761342.