Stress cardiomyopathy
| Stress cardiomyopathy | |
 | |
|---|---|
| Schematic representation of Takotsubo cardiomyopathy (A) compared to the situation in a normal person (B). | |
| ICD-9 | 429.83 |
| DiseasesDB | 33976 |
| MeSH | 054549 |
|
Stress cardiomyopathy Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Unstable angina/non ST elevation myocardial infarction in Stress (Takotsubo) Cardiomyopathy |
|
Case Studies |
|
Stress cardiomyopathy On the Web |
|
American Roentgen Ray Society Images of Stress cardiomyopathy |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]
Synonyms and keywords: Takotsubo cardiomyopathy; Tako-tsubo syndrome; Left Ventricular Apical Ballooning Syndrome; Ampulla-Shaped Cardiomyopathy; Broken Heart Syndrome; transient apical dysfunction
Overview
Stress cardiomyopathy is a cardiac syndrome characterized by a reversible transient apical ventricular dysfunction.
Differentiating Stress Cardiomyopathy from other Conditions
Other conditions that stress cardiomyopathy should be distinguished from include:
- Acute Coronary Syndrome (common)
- Myocarditis (uncommon)
- Pheochromocytoma induced cardiomyopathy (rare)
Epidemiology and Demographics
The exact incidence is unknown, but it is estimated that apical ballooning syndrome may account for 1-2% of patients who present with an acute myocardial infarction. The cardiomyopathy appears to occur almost exclusively in post-menopausal women, although a few cases have been reported in younger women and males.[1] In one of the largest series of 256 patients, [2] post-menopausal women made up 81% of enrolled patients, while 8% were younger women, and 11% were men.
Risk Factors
Often there is a history of a recent severe emotional or physical stress.[1] Case series looking at large groups of patients report that some patients develop apical balloon syndrome after an emotional stressor, while others have a preceding clinical stressor (such as an asthma attack or sudden illness). Roughly one third of patients have no preceding stressful event [3]. The syndrome has been reported to occur after earthquakes, [4] after non-cardiac surgery, [5] and in patients with noncardiac medical emergencies. [6]
Although it had been previously reported that an identifiable stressful event occurred in most patients (90%) prior to onset of stress cardiomyopathy, only 71% of patients in Eitel et al.’s study experienced a clearly identifiable emotional or physical trigger [7]. Thus, it cannot be assumed that all stress cardiomyopathy patients experience a common trigger, and a stress cardiomyopathy diagnosis cannot be discounted if a trigger is not present.
Natural History, Complications and Prognosis
Provided that the individual survives their initial presentation, the left ventricular function improves within days to weeks.[8]
Complications[9]
- Heart failure
- Cardiogenic shock
- Left ventricular outflow tract obstruction
- Mitral regurgitation[10][11]
- Ventricular arrhythmias
Prognosis
The recurrence rate is about 3%[12][13]. The in-hospital mortality is very low (1-2%), typically related to the underlying disease in those with physical stressors. Long term survival is good.
Diagnosis
History
A directed history should be obtained to evaluate if the patient has a history of emotional stress such as the death of a loved one or loss of job.
Symptoms
- The typical presentation of patients with stress cardiomyopathy includes acute onset of chest pain or shortness of breath, and is similar to an acute coronary syndrome
Physical examination
- Bulging out of the left ventricular apex with a hypercontractile base of the left ventricle is often noted.
Electrocardiogram
The EKG findings are often confused with those of an acute anterior wall myocardial infarction.[1][14] While the ECG may reveal ST-segment elevation, it may also reveal non-specific ST/T wave abnormality, usually in the precordial leads. The 12-lead ECG alone is not helpful in differentiating apical ballooning syndrome from a traditional thrombotic ST-elevation myocardial infarction. Evolutionary changes occur over 2 to 3 days that are characteristic and include resolution of the ST-segment elevation and development of diffuse and frequently deep T-wave inversion.

The diagnosis of takotsubo cardiomyopathy may be difficult upon presentation. The EKG findings are often confused with those found during an acute anterior wall myocardial infarction.[1][14]
Biomarker Studies
Cardiac biomarkers of myonecrosis, especially troponin, are invariably elevated.
Echocardiography

Cardiac Catheterization
Coronary angiography usually demonstrates normal coronary arteries or mild coronary atherosclerosis. The left ventriculogram usually reveals characteristic regional wall motion abnormalities which involve the mid and usually the apical segments. There is sparing of the basal systolic function, and the wall motion abnormality extends beyond the distribution of any one single coronary artery.

The diagnosis is made by the pathognomic wall motion abnormalities, in which the base of the left ventricle is contracting normally or are hyperkinetic while the remainder of the left ventricle is akinetic or dyskinetic. This is accompanied by the lack of significant coronary artery disease that would explain the wall motion abnormalities.
Magnetic Resonance Imaging
The use of MRIs as a valuable diagnostic tool in differentiating cardiomyopathy from acute myocardial infarction and myocarditis cases. Cardiac magnetic resonance imaging is helpful in excluding a myocardial infarction due to the absence of delayed gadolinium hyperenhancement.
The Eitel study is the largest (n=256), (multi-center) cardiovascular MRI imaging series of stress cardiomyopathy [15]. Stress cardiomyopathy can be accurately diagnosed by identifying a typical pattern of LV dysfunction, myocardial edema, absence of significant necrosis/fibrosis, and markers of myocardial inflammation. There are four distinct patterns of regional ventricular ballooning: apical (82%), biventricular (34%), midventricular (17%), and basal (1%). Because patients with RV involvement tended to be older, hospitalized for longer, and have markers of heart failure, biventricular ballooning on MRI “may portend a longer and more severe course of disease compared with patients with isolated (LV) involvement.” Dysfunctions in the right ventricle are important to identify due to its effects on morbidity, treatment, and outcome. During follow up MRIs, patients exhibited normalization of LVEF (66%) and inflammatory markers in the absence of significant fibrosis in all patients.
MRI Examples
The MRIs below show a patients heart with apical ballooning and then later after resolution of the apical ballooning.
MRI during apical balllooning: <youtube v=23w6f71zTXI/> ____
MRI following resolution of apical ballooning: <youtube v=qE0YrlQ5d1o/>
The Various Patterns of Wall Motion Abnormalities
It should be that the wall motion abnormalities are not always anteroapical.
-
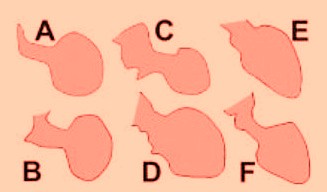
Different end-systolic left ventricular (LV) silhouettes.

A, [16]; B, [17]; C, [18]; D, [19]; E, [20]; and F, [21]. There is wide heterogeneity among the different patterns, varying from a relatively small akinetic apical area in C to a wide global akinesia in D and E. [22]
Mayo Criteria
Mayo Clinic Criteria for Apical Ballooning Syndrome. All 4 must be present [23]:
- Transient hypokinesis, akinesis or dyskinesis of the left ventricular mid-segments with or without apical involvement. The regional wall motion abnormalities extend beyond a single epicardial vascular distribution. A stressful trigger is often, but not always present
- Absence of obstructive coronary disease or angiographic evidence of acute plaque rupture.
- New electrocardiographic abnormalities (either ST-segment elevation and/or T- wave inversion) or modest elevation in cardiac troponin.
- Absence of pheochromocytoma and myocarditis
Treatment
The treatment of stress cardiomyopathy is supportive as the condition is reversible. Initial treatment should be similar to that of an acute coronary syndrome with therapy directed at relieving myocardial ischemia with administration of aspirin, intravenous heparin and beta blockers. Once a diagnosis of stress cardiomyopathy has been confirmed and an acute coronary syndrome excluded, consideration should be given to continuing beta-blocker therapy empirically since catecholamines are suspected of contributing to the syndrome. Diuretics are effective for the treatment of congestive heart failure. Angiotensin converting enzyme inhibitors may be used if the diagnosis is uncertain, until there is complete recovery of systolic function. Insofar as the left ventricular function and apical wall motion return to normal within days or weeks, long-term anti-coagulation does not appear to be necessary.
References
- ↑ 1.0 1.1 1.2 1.3 Azzarelli S, Galassi AR, Amico F, Giacoppo M, Argentino V, Tomasello SD, Tamburino C, Fiscella A. (2006). "Clinical features of transient left ventricular apical ballooning". Am J Cardiol. 98 (9): 1273–6. PMID 17056345.
- ↑ Eitel I, von Knobelsdorff-Brekenhoff F, Bernhardt P, et al. Clinical characteristics and CV magnetic resonance findings in stress (Takotsubo) cardiomyopathy. JAMA 2011; 306:277-286.
- ↑ Elesber, AA (2007). "Four-Year Recurrence Rate and Prognosis of the Apical Ballooning Syndrome". J Amer Coll Card. 50 (5): 448–52. Unknown parameter
|month=ignored (help) - ↑ Yamabe H, Hanaoka J, Funakoshi T; et al. (1996). "Deep negative T waves and abnormal cardiac sympathetic image (123I-MIBG) after the Great Hanshin Earthquake of 1995". Am. J. Med. Sci. 311 (5): 221–4. PMID 8615397.
- ↑ Berman M, Saute M, Porat E; et al. (2007). "Takotsubo cardiomyopathy: expanding the differential diagnosis in cardiothoracic surgery". Ann. Thorac. Surg. 83 (1): 295–8. doi:10.1016/j.athoracsur.2006.05.115. PMID 17184686.
- ↑ Akashi YJ, Sakakibara M, Miyake F (2002). "Reversible left ventricular dysfunction "takotsubo" cardiomyopathy associated with pneumothorax". Heart. 87 (2): E1. PMID 11796564.
- ↑ Eitel I, von Knobelsdorff-Brekenhoff F, Bernhardt P, et al. Clinical characteristics and CV magnetic resonance findings in stress (Takotsubo) cardiomyopathy. JAMA 2011; 306:277-286.
- ↑ Akashi YJ, Barbaro G, Sakurai T, Nakazawa K, Miyake F (2007). "Cardiac autonomic imbalance in patients with reversible ventricular dysfunction takotsubo cardiomyopathy". QJM. 100 (6): 335–43. doi:10.1093/qjmed/hcm028. PMID 17483198.
- ↑ Brunetti ND, Ieva R, Rossi G, Barone N, De Gennaro L, Pellegrino PL, Mavilio G, Cuculo A, Di Biase M (2008). "Ventricular outflow tract obstruction, systolic anterior motion and acute mitral regurgitation in Tako-Tsubo syndrome". International Journal of Cardiology. 127 (3): e152–7. doi:10.1016/j.ijcard.2007.04.149. PMID 17692942. Retrieved 2011-04-16. Unknown parameter
|month=ignored (help) - ↑ Haghi D, Röhm S, Suselbeck T, Borggrefe M, Papavassiliu T (2010). "Incidence and clinical significance of mitral regurgitation in Takotsubo cardiomyopathy". Clinical Research in Cardiology : Official Journal of the German Cardiac Society. 99 (2): 93–8. doi:10.1007/s00392-009-0078-1. PMID 19774331. Retrieved 2011-04-16. Unknown parameter
|month=ignored (help) - ↑ http://circimaging.ahajournals.org/content/early/2011/04/15/CIRCIMAGING.110.962845.abstract
- ↑ Barkhattov TP (1991). "[The pathological preliminary period]". Felʹdsher I Akusherka (in Russian). 56 (8): 51–4. PMID 1765184. Unknown parameter
|month=ignored (help);|access-date=requires|url=(help) - ↑ Prasad A, Lerman A, Rihal CS (2008). "Apical ballooning syndrome (Tako-Tsubo or stress cardiomyopathy): a mimic of acute myocardial infarction". American Heart Journal. 155 (3): 408–17. doi:10.1016/j.ahj.2007.11.008. PMID 18294473. Retrieved 2011-04-16. Unknown parameter
|month=ignored (help) - ↑ 14.0 14.1 Bybee KA, Motiei A, Syed IS, Kara T, Prasad A, Lennon RJ, Murphy JG, Hammill SC, Rihal CS, Wright RS (2006). "Electrocardiography cannot reliably differentiate transient left ventricular apical ballooning syndrome from anterior ST-segment elevation myocardial infarction". J Electrocardiol. PMID 17067626.
- ↑ Eitel I, von Knobelsdorff-Brekenhoff F, Bernhardt P, et al. Clinical characteristics and CV magnetic resonance findings in stress (Takotsubo) cardiomyopathy. JAMA 2011; 306:277-286.
- ↑ Abe Y, Kondo M, Matsuoka R, Araki M, Dohyama K, Tanio H. Assessment of clinical features in transient left ventricular apical ballooning. J Am Coll Cardiol. 2003;41:737-742.
- ↑ San Roman Sanchez D, Medina O, Jimenez F, Rodriguez JC, Nieto V. Dynamic intraventricular obstruction in acute myocardial infarction. Echocardiography. 2001;18:515-518.
- ↑ Wittstein IS, Thiemann DR, Lima JA, et al. Neurohumoral features of myocardial stunning due to sudden emotional stress. N Engl J Med. 2005;352:539-548.
- ↑ Rivera JM, Locketz AJ, Fritz KD, et al. “Broken heart syndrome” after separation (from OxyContin). Mayo Clin Proc. 2006;81:825-828.
- ↑ Desmet WJ, Adriaenssens BF, Dens JA. Apical ballooning of the left ventricle: first series in white patients. Heart. 2003;89:1027-1031.
- ↑ Reyburn AM, Vaglio JC Jr. Transient left ventricular apical ballooning syndrome. Mayo Clin Proc. 2006;81:824.
- ↑ Ibanez B. Takotsubo Syndrome: A Bayesian Approach to Interpreting Its Pathogenesis Mayo Clin Proc. 2006; 81: 732-735
- ↑ Prasad A (2007). "Apical ballooning syndrome: an important differential diagnosis of acute myocardial infarction". Circulation. 115 (5): e56–9. doi:10.1161/CIRCULATIONAHA.106.669341. PMID 17283269.