Rocky Mountain spotted fever medical therapy: Difference between revisions
No edit summary |
|||
| Line 1: | Line 1: | ||
{{Rocky Mountain spotted fever}} | {{Rocky Mountain spotted fever}} | ||
{{CMG}} | {{CMG}}{{AE}}{{SR}} | ||
==Overview== | ==Overview== | ||
Revision as of 14:59, 12 August 2015
|
Rocky Mountain spotted fever Microchapters |
|
Differentiating Rocky Mountain spotted fever from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Rocky Mountain spotted fever medical therapy On the Web |
|
American Roentgen Ray Society Images of Rocky Mountain spotted fever medical therapy |
|
Directions to Hospitals Treating Rocky Mountain spotted fever |
|
Risk calculators and risk factors for Rocky Mountain spotted fever medical therapy |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]Associate Editor(s)-in-Chief: Sujit Routray, M.D. [2]
Overview
Treatment
Appropriate antibiotic treatment should be initiated immediately when there is a suspicion of Rocky Mountain spotted fever on the basis of clinical and epidemiologic findings. Treatment should not be delayed until laboratory confirmation is obtained.
If the patient is treated within the first 4-5 days of the disease, fever generally subsides within 24-72 hours after treatment with an appropriate antibiotic (usually in the tetracycline class). In fact, failure to respond to a tetracycline antibiotic argues against a diagnosis of RMSF. Severely ill patients may require longer periods before their fever resolves, especially if they have experienced damage to multiple organ systems. Preventive therapy in non-ill patients who have had recent tick bites is not recommended and may, in fact, only delay the onset of disease.
-

Removal of an embedded tick using fine-tipped tweezers
-
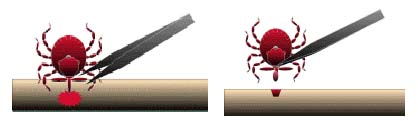
Tick removal process

What is the best way to remove a tick?
- Use fine-tipped tweezers or notched tick extractor, and protect your fingers with a tissue, paper towel, or latex gloves. Persons should avoid removing ticks with bare hands.
- Grasp the tick as close to the skin surface as possible and pull upward with steady, even pressure. Do not twist or jerk the tick; this may cause the mouthparts to break off and remain in the skin. (If this happens, remove mouthparts with tweezers. Consult your health care provider if illness occurs.)
- After removing the tick, thoroughly disinfect the bite site and wash your hands with soap and water.
- Do not squeeze, crush, or puncture the body of the tick because its fluids may contain infectious organisms. Skin accidentally exposed to tick fluids can be disinfected with iodine scrub, rubbing alcohol, or water containing detergents.
- Save the tick for identification in case you become ill. This may help your doctor to make an accurate diagnosis. Place the tick in a sealable plastic bag and put it in your freezer. Write the date of the bite on a piece of paper with a pencil and place it in the bag.
Do folklore remedies work?
No. Folklore remedies, such as the use of petroleum jelly or hot matches, do little to encourage a tick to detach from skin. In fact, they may make matters worse by irritating the tick and stimulating it to release additional saliva or regurgitate gut contents, increasing the chances of transmitting the pathogen. These methods of tick removal should be avoided.
Antimicrobial regimen
- Preferred regimen: Doxycycline 100 mg q12h
- Alternative regimen: Chloramphenicol especially in pregnant women, but needs close monitoring.
- Pediatric regimen: Doxycycline 2.2 mg/kg PO bid (under 45 kg (100 lbs))
- Note: Patients should be treated for at least 3 days after the fever subsides and until there is evidence of clinical improvement; Standard duration of treatment is 7-14 days.