Rheumatic fever pathophysiology
|
Rheumatic fever Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Rheumatic fever pathophysiology On the Web |
|
American Roentgen Ray Society Images of Rheumatic fever pathophysiology |
|
Risk calculators and risk factors for Rheumatic fever pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Lance Christiansen, D.O.; Associate Editor(s)-in-Chief: Cafer Zorkun, M.D., Ph.D. [2]; Anthony Gallo, B.S. [3]
Overview
Rheumatic fever is the result of an autoimmunological sequela to a virulent Streptococcus pyogenes infection in a patient who was immunologically sensitized from prior infections.During a streptococcal infection, activated antigen presenting cells, such as macrophages, present the bacterial antigen to helper T cells. Helper T cells subsequently activate B cells and induce the production of antibodies against the cell wall of streptococcus. However the antibodies may also act against the myocardium and joints, producing the symptoms of rheumatic fever.[1]
Pathophysiology
Pathogenesis
Rheumatic fever is the result of an autoimmunological sequela to a virulent Streptococcus pyogenes infection in a patient who was immunologically sensitized from prior infections. The systemic disease affects the periarteriolar connective tissue and can occur after an untreated Group A streptococcal pharyngeal infection. It is believed to be caused by antibody cross-reactivity which is a Type II hypersensitivity reaction.[1]
Usually, self reactive B cells remain anergic in the periphery without T cell co-stimulation. During a streptococcal infection, activated antigen presenting cells, such as macrophages, present the bacterial antigen to helper T cells. Helper T cells subsequently activate B cells and induce the production of antibodies against the cell wall of streptococcus. However the antibodies may also act against the myocardium and joints, producing the symptoms of rheumatic fever.
Contrary to the immunological protection developed during most infections, infections by Streptococcus pyogenes cause both a protective immunological and pathological autoimmunological stimulation. Repeated infections by Streptococcus pyogenes will cause both a heightened protective and pathological immune response. The immune response helps in combating the streptococcal infection. However, the autoimmunological response causes an inflammatory, systemic, disease process, rheumatic fever.
In acute rheumatic fever, these lesions may occur in endocardium, myocardium or pericardium. The inflammation may cause a serofibrinous pericardial exudates described as “bread-and-butter” pericarditis, which usually resolves without sequelae. Involvement of the endocardium typically results in fibrinoid necrosis and verrucae formation along the lines of closure of the left heart valves. Warty projections arise from the deposition, while subendothelial lesions may induce irregular thickenings called MacCallum plaques.[2]
Gross and Microscopic Pathology
Gross
On gross pathology, the following features are characteristic findings of rheumatic fever:[3]
- "Fish-mouth appearance"
- Slit-like morphology; elliptical cross-sectional flow area (mitral valve) with abnormally small semi-minor axis axis due to valve thickening
- Significant valvular thickening
- Thickening and shortening of the chorda tympani
Microscopic histopathological analysis
On microscopic histopathological analysis, the following features are characteristic findings of rheumatic fever:[3][4][4]
- Caterpillar cells
- Abundant eosinophilic cytoplasm
- Moderately-poorly defined cell border
- Well-defined central ovoid nucleus with a prominent wavy ribbon-like chromatin
- Aschoff bodies found within the heart
- Jumbled collagen, eosinophilic
- Surrounded by T cells
Images
The following are gross and microscopic images associated with rheumatic fever:[5]
-

Aortic stenosis (Tricuspid aorta): gross, an example of aortic stenosis due to rheumatic fever
-
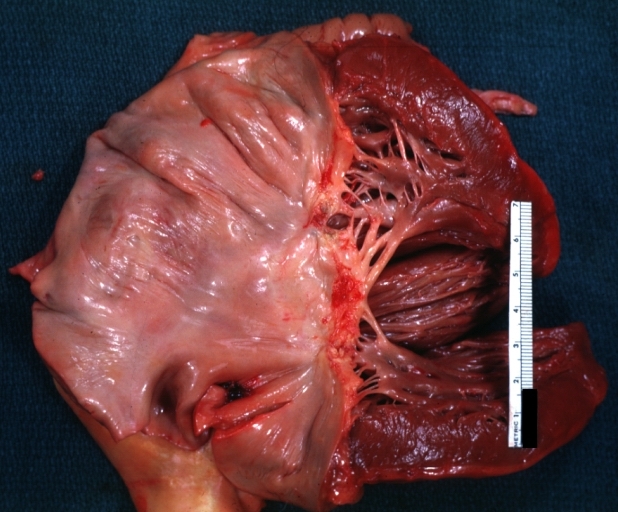
Mitral scarring: gross, an example of mitral scarring due to rheumatic fever (healing phase of an infectious lesion)
-
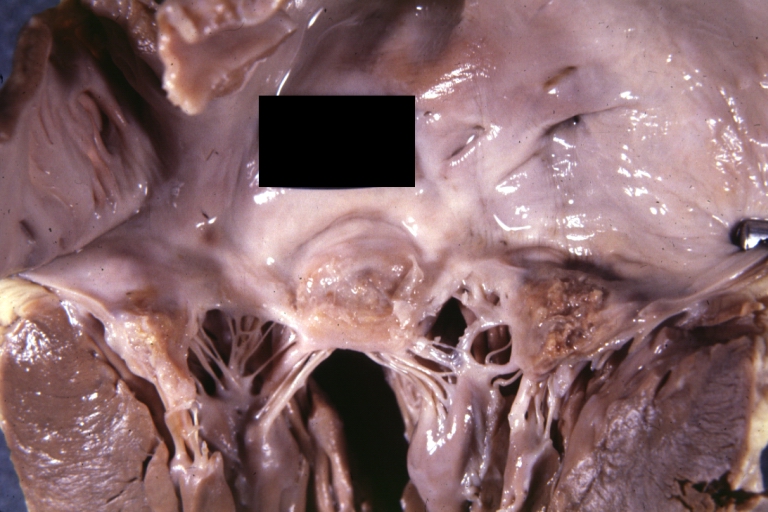
Rheumatic mitral valvulitis: gross, rheumatic mitral valvulitis: Gross, an example of fibrosis, chorda thickening and shortening with thrombus around the large left atrium
-
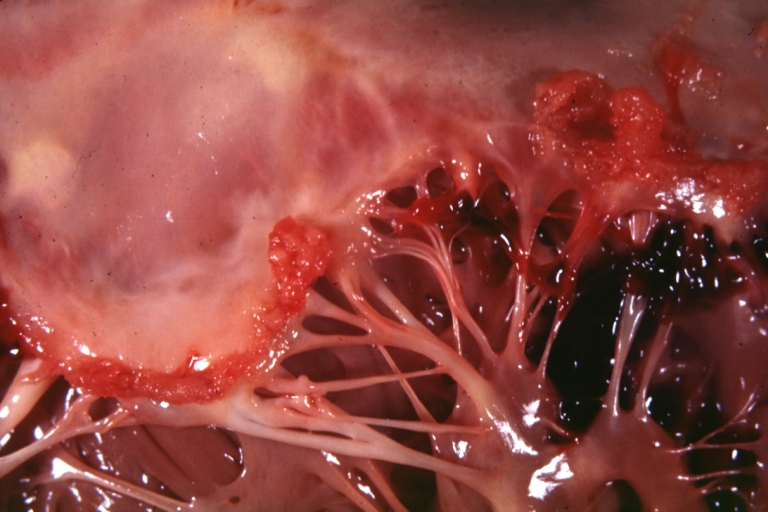
Rheumatic mitral valvulitis: Gross, an example of acute rheumatic fever lesion along line of closure of mitral valve
-
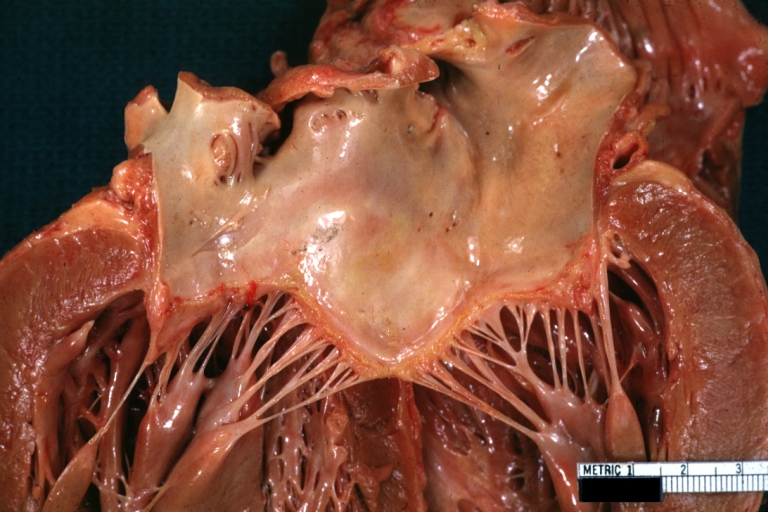
Mitral valve: gross, acute rheumatic fever
-
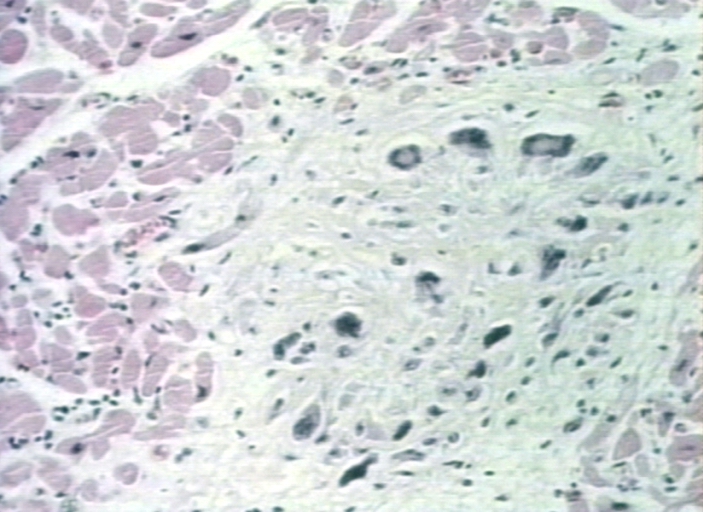
Aschoff bodies: microscopic histopathological analysis, Aschoff bodies in rheumatic heart disease






References
- ↑ 1.0 1.1 Rheumatic Fever. Wikipedia (2015). http://www.mayoclinic.org/diseases-conditions/rheumatic-fever/basics/causes/con-20031399 Accessed on October 12, 2015
- ↑ Chopra P, Gulwani H (2007). "Pathology and pathogenesis of rheumatic heart disease". Indian J Pathol Microbiol. 50 (4): 685–97. PMID 18306530.
- ↑ 3.0 3.1 Rheumatic Heart Disease. Libre Pathology (2015). http://librepathology.org/wiki/index.php/Heart_valves#Rheumatic_heart_disease Accessed on October 12, 2015
- ↑ 4.0 4.1 Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease. St. Louis, MO: Elsevier Saunders. ISBN 0-7216-0187-1.
- ↑ Pathology Education Instructional Resource. University of Alabama at Birmingham (2014). Images courtesy of Propessor Peter Anderson DVM PhD and published with permission of PEIR, Department of Pathology, University of Alabama at Birmingham. http://www.peir.net Accessed on October 12, 2015.