Follicular thyroid cancer staging: Difference between revisions
No edit summary |
|||
| Line 45: | Line 45: | ||
! style="background: #DCDCDC;" |T4a | ! style="background: #DCDCDC;" |T4a | ||
! style="background: #F5F5F5;" |Intrathyroidal anaplastic carcinoma | ! style="background: #F5F5F5;" |Intrathyroidal anaplastic carcinoma | ||
|} | |} | ||
<br> | <br> | ||
| Line 244: | Line 241: | ||
</gallery> | </gallery> | ||
==Reference== | ==Reference== | ||
{{Reflist|2}} | {{Reflist|2}} | ||
Revision as of 13:31, 2 November 2015
|
Follicular thyroid cancer Microchapters |
|
Differentiating Follicular thyroid cancer from other Diseases |
|---|
|
Diagnosis |
|
Treatment |
|
Case Studies |
|
Follicular thyroid cancer staging On the Web |
|
American Roentgen Ray Society Images of Follicular thyroid cancer staging |
|
Risk calculators and risk factors for Follicular thyroid cancer staging |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]; Associate Editor(s)-in-Chief: Ammu Susheela, M.D. [2]
Overview
According to the American Joint Committee on Cancer (AJCC)[1] there are 4 stages of follicular thyroid cancer based on the clinical features and findings on imaging. Each stage is assigned a letter and a number that designate the tumor size, number of involved lymph node regions, and metastasis.
Staging
| Stage | Description |
|---|---|
| TX | Primary tumor cannot be assessed |
| T0 | No evidence of primary tumor |
| T1 | Tumor ≤2 cm in greatest dimension limited to the thyroid |
| T1a | Tumor ≤1 cm, limited to the thyroid |
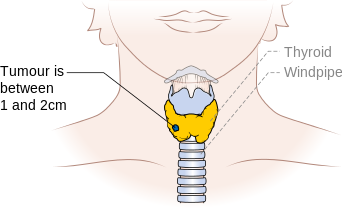
| T1b | Tumor >1 cm but ≤2 cm in greatest dimension, limited to the thyroid |
| T2 | Tumor >2 cm but ≤4 cm in greatest dimension, limited to the thyroid |
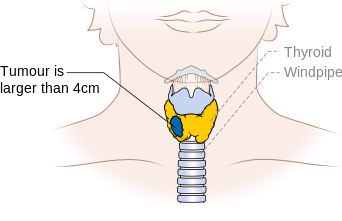
| T3 | Tumor >4 cm in greatest dimension limited to the thyroid or any tumor with minimal extrathyroid extension (e.g., extension to sternothyroid muscle or perithyroid soft tissues) |
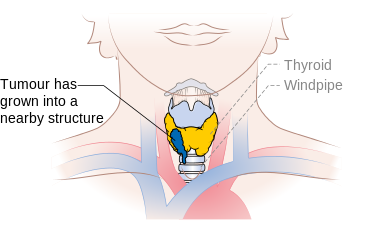
| T4a | Moderately advanced disease |
| Tumor of any size extending beyond the thyroid capsule to invade subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve | |
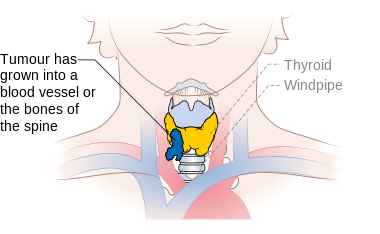
| T4b | Very advanced disease |
| Tumor invades prevertebral fascia or encases carotid artery or mediastinal vessel | |
| T4a | Intrathyroidal anaplastic carcinoma |
| Stage | Description |
|---|---|
| NX | Regional lymph nodes cannot be assessed |
| N0 | No regional lymph node metastasis |
| N1 | Regional lymph node metastasis |
| N1a | Metastases to Level VI (pretracheal, paratracheal, and prelaryngeal/Delphian lymph nodes) |
| N1b | Metastases to unilateral, bilateral, or contralateral cervical (Levels I, II, III, IV, or V) or retropharyngeal or superior mediastinal lymph nodes (Level VII) |
| Stage | Description |
|---|---|
| M0 | No distant metastasis |
| M1 | Distant metastasis |
| Stage | T | N | M |
|---|---|---|---|
| Follicular thyroid carcinoma | |||
| YOUNGER THAN 45 YEARS | |||
| I | Any T | Any N | M0 |
| II | Any T | Any N | M1 |
| 45 YEARS AND OLDER | |||
| I | T1 | Any N | M1 |
| II | T2 | N0 | M0 |
| III | T3 | N0 | M0 |
| T1 | N1a | M0 | |
| T2 | N1a | M0 | |
| T3 | N1a | M0 | |
| IVA | T4a | N0 | M0 |
| T4a | N1a | M0 | |
| T1 | N1b | M0 | |
| T2 | N1b | M0 | |
| T3 | N1b | M0 | |
| T4a | N1b | M0 | |
| IVB | T4b | Any N | M0 |
| Stage IVC | Any T | Any N | M1 |
Papillary and Follicular Thyroid Cancer
Stage I Papillary Thyroid Cancer
- Stage I papillary carcinoma is localized to the thyroid gland. In as many as 50% of cases, there are multifocal sites of papillary adenocarcinomas throughout the gland. Most papillary cancers have some follicular elements, and these may sometimes be more numerous than the papillary formations, but this does not change the prognosis. The 10-year survival rate is slightly better for patients younger than 45 years than for patients older than 45 years
Stage II Papillary Thyroid Cancer
Stage II papillary carcinoma is defined as either: (1) tumor that has spread distantly in patients younger than 45 years, or (2) tumor that is larger than 2 cm but 4 cm or smaller and is limited to the thyroid gland in patients older than 45 years. In as many as 50% to 80% of cases, there are multifocal sites of papillary adenocarcinomas throughout the gland. Most papillary cancers have some follicular elements, and these may sometimes be more numerous than the papillary formations, but this does not appear to change the prognosis.
Stage III Papillary Thyroid Cancer
- Stage III is papillary carcinoma in patients older than 45 years that is larger than 4 cm and is limited to the thyroid or with minimal extrathyroid extension, or positive lymph nodes limited to the pretracheal, paratracheal, or prelaryngeal/Delphian nodes. Papillary carcinoma that has invaded adjacent cervical tissue has a worse prognosis than tumors confined to the thyroid.
Stage IV Papillary Thyroid Cancer
- Stage IV is papillary carcinoma in patients older than 45 years with extension beyond the thyroid capsule to the soft tissues of the neck, cervical lymph node metastases, or distant metastases. The lungs and bone are the most frequent distant sites of spread, though such distant spread is rare in this type of thyroid cancer. Papillary carcinoma more frequently metastasizes to regional lymph nodes than to distant sites. The prognosis for patients with distant metastases is poor.
Stage I Follicular Thyroid Cancer
- Stage I follicular carcinoma is localized to the thyroid gland. Follicular thyroid carcinoma must be distinguished from follicular adenomas, which are characterized by their lack of invasion through the capsule into the surrounding thyroid tissue. While follicular cancer has a good prognosis, it is less favorable than that of papillary carcinoma. The 10-year survival is better for patients with follicular carcinoma without vascular invasion than it is for patients with vascular invasion.
Stage II Follicular Thyroid Cancer
- Stage II follicular carcinoma is defined as either tumor that has spread distantly in patients younger than 45 years, or tumor that is larger than 2 cm but 4 cm or smaller and is limited to the thyroid gland in patients older than 45 years. The presence of lymph node metastases does not worsen the prognosis among patients younger than 45 years. Follicular thyroid carcinoma must be distinguished from follicular adenomas, which are characterized by their lack of invasion through the capsule into the surrounding thyroid tissue. While follicular cancer has a good prognosis, it is less favorable than that of papillary carcinoma; the 10-year survival is better for patients with follicular carcinoma without vascular invasion than for patients with vascular invasion.
Stage III Follicular Thyroid Cancer
- Stage III is follicular carcinoma in patients older than 45 years, larger than 4 cm and limited to the thyroid or with minimal extrathyroid extension, or positive lymph nodes limited to the pretracheal, paratracheal, or prelaryngeal/Delphian nodes. Follicular carcinoma invading cervical tissue has a worse prognosis than tumors confined to the thyroid gland. The presence of vascular invasion is an additional poor prognostic factor. Metastases to lymph nodes do not worsen the prognosis in patients younger than 45 years.
Stage IV Follicular Thyroid Cancer
- Stage IV is follicular carcinoma in patients older than 45 years with extension beyond the thyroid capsule to the soft tissues of the neck, cervical lymph node metastases, or distant metastases. The lungs and bone are the most frequent sites of spread. Follicular carcinomas more commonly have blood vessel invasion and tend to metastasize hematogenously to the lungs and to the bone rather than through the lymphatic system. The prognosis for patients with distant metastases is poor.
-
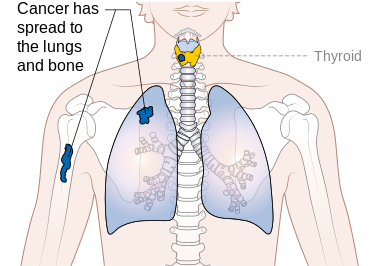
Stage M1 thyroid cancer
-
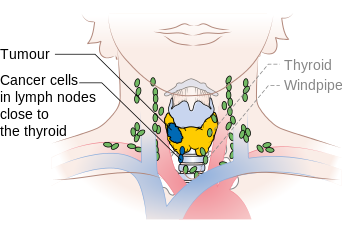
Stage N1a thyroid cancer
-
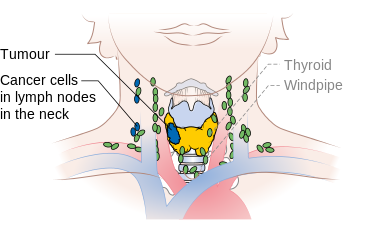
Stage N1b thyroid cancer
-
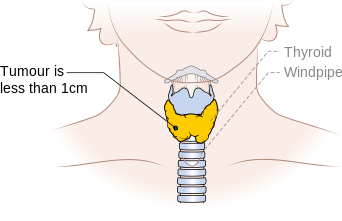
Stage T1a thyroid cancer
-
Stage T1b thyroid cancer
-
Stage T2 thyroid cancer
-
Stage T3 thyroid cancer
-
Stage T4a thyroid cancer
-
Stage T4b thyroid cancer








Reference
- ↑ Stage Information for Thyroid Cancer Cancer.gov (2015). http://www.cancer.gov/types/thyroid/hp/thyroid-treatment-pdq#link/stoc_h2_2- cancer staging Accessed on October, 29 2015