Cervical cancer pathophysiology
|
Cervical cancer Microchapters |
|
Diagnosis |
|---|
|
Treatment |
|
Case Studies |
|
Cervical cancer pathophysiology On the Web |
|
American Roentgen Ray Society Images of Cervical cancer pathophysiology |
|
Risk calculators and risk factors for Cervical cancer pathophysiology |
Editor-In-Chief: C. Michael Gibson, M.S., M.D. [1]}Associate Editor(s)-in-Chief: Monalisa Dmello, M.B,B.S., M.D. [2] Aida Javanbakht, M.D.
Overview
Cervical cancer arises at squamous-columnar junction. It could happen as a primary malignant tumor or as a metastasis from other tumors.
Pathophysiology
Pathogenesis:
- Human papillomaviruses, a sexually transmitted virus, subtypes 16 and 18 (High risk) play an important role in the pathogenesis of cervical cancer. Once HPV enters an epithelial cell, begins to make the proteins. Two of the proteins (E6 and E7) interfere with cell functions that normally prevent excessive growth. Those proteins induce the cells to grow in uncontrolled ways and prevent cell death. Many times these infected cells are recognized by the immune system and eliminated. Sometimes these infected cells are not destroyed, and a persistent infection results. As the persistently infected cells continue to grow, they may develop mutations in cellular genes that promote even more abnormal cell growth, leading to the formation of an area of precancerous cells and, ultimately, a cancerous tumor.[1]
- Cervical carcinoma has its origins at the squamous-columnar junction; it can involve the outer squamous cells, the inner glandular cells, or both. The precursor lesion is dysplasia: cervical intraepithelial neoplasia (CIN) or adenocarcinoma in situ, which can subsequently become invasive cancer. This process can be quite slow. Longitudinal studies have shown that in patients with untreated in situ cervical cancer, 30% to 70% will develop invasive carcinoma over a period of 10 to 12 years. However, in about 10% of patients, lesions can progress from in situ to invasive in a period of less than 1 year. As it becomes invasive, the tumor breaks through the basement membrane and invades the cervical stroma. Extension of the tumor in the cervix may ultimately manifest as ulceration, exophytic tumor, or extensive infiltration of underlying tissue, including the bladder or rectum.[2]
- Important factors in causing cervical cancer:
Immune system condition of the patient.
Smocking.
Subtypes of the HPV.
High numbers of sexual partners.
Genetic:
Any mutation in TNFa-8, TNFa-572, TNFa-857, TNFa-863, and TNF G-308A has been reported in causing cervical cancer. Also, TLR9 1486 T/C and G2848A polymorphisms have association with cervical cancer.[3]
Associated Conditions:
Long term using oral contraceptives has been associated with cervical cancer. It could be because of increase high risk sexual behavior in women. [4]
Gross Pathology:
It could be like a polyp in cervix.
Microscopic pathology
- Prominent nucleoli.
- Blurred or scalloped epithelial-stromal interface.
- Loss of nuclear polarity.
- Pseudoglandular pattern because of acantholysis and central necrosis.
-
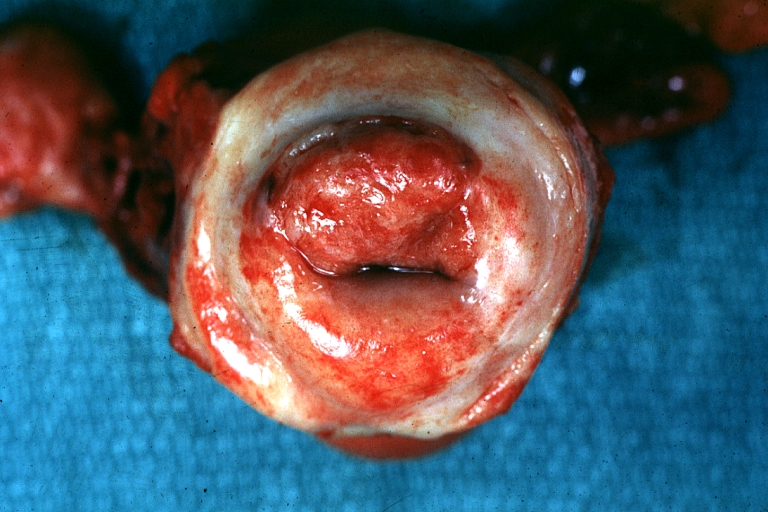
Uterus: Cervical Carcinoma: Gross, an excellent example of tumor (labeled as invasive)
Image courtesy of Professor Peter Anderson DVM PhD and published with permission © PEIR, University of Alabama at Birmingham, Department of Pathology -
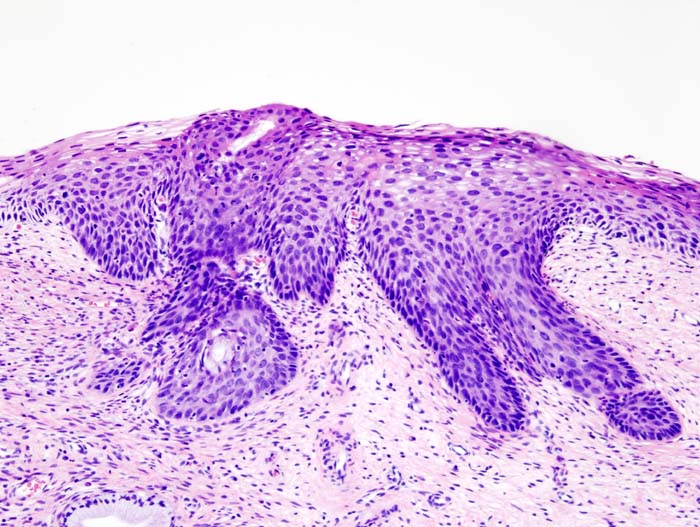
Histopathologic image (H&E stain) of cervical intraepithelial neoplasia.

_CIN3.jpg)
Video
{{#ev:youtube|J3kULzKGzws}}
References
- ↑ http://www.cancer.gov/about-cancer/causes-prevention/risk/infectious-agents/hpv-fact-sheet
- ↑ http://www.cancer.gov/types/cervical/hp/cervical-treatment-pdq#link/_532_toc
- ↑ Yang S, Liu L, Xu D, Li X (September 2018). "The Relationship of the TLR9 and TLR2 Genetic Polymorphisms with Cervical Cancer Risk: a Meta-Analysis of Case-Control Studies". Pathol. Oncol. Res. doi:10.1007/s12253-018-0465-x. PMID 30215163.
- ↑ Gierisch JM, Coeytaux RR, Urrutia RP, Havrilesky LJ, Moorman PG, Lowery WJ, Dinan M, McBroom AJ, Hasselblad V, Sanders GD, Myers ER (November 2013). "Oral contraceptive use and risk of breast, cervical, colorectal, and endometrial cancers: a systematic review". Cancer Epidemiol. Biomarkers Prev. 22 (11): 1931–43. doi:10.1158/1055-9965.EPI-13-0298. PMID 24014598.